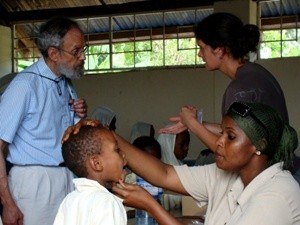
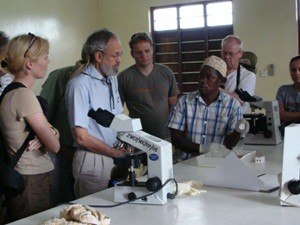
Report of my experiences with a tropical medicine expedition for healthcare professionals in Tanzania, 2009 Arthur Dover, MD, DTMH In my opinion, the training for healthcare providers in the areas of clinical tropical medicine and travelers health in non-tropical countries has yet to reach an adequate standard. Each year, more and more tourists choose travel destinations in tropical and subtropical regions, often without immunization or malaria chemoprophylaxis. Returning travellers still succumb to malaria and other tropical infectious diseases simply because the infections are recognized too late, if at all, by medical professionals in American and European hospitals. Practice-oriented training program for doctors and other travel medicine professionals is essential to the prompt, correct diagnosis and treatment of tropical infectious diseases. A very special two-week Tanzanian excursion lay ahead of us, which we would later come to regard as an incredible experience. I traveled with my wife Dilma, who works as a nurse in my travel clinic in California. Upon landing at Kilimanjaro International Airport, we met the other 12 travelers - medical colleagues from Belgium, Switzerland and Germany. Arriving at the Arusha Coffee Lodge, we met our excursion leader, Kay Schaefer (MD, PhD, MSc, DTM&H), a consultant in Tropical Medicine and Travelers' Health in Cologne, Germany. He had added Tanzania as a new destination for his "Tropical Medicine Expeditions" to East Africa. Since 1995 he has organized tropical medicine expeditions to Kenya and Uganda (in total 32 excursions with over 250 participants from `round the world') for healthcare professionals. These are done in collaboration with leading medical institutions and hospitals in East Africa. He and local experts supervise individual on-site bedside teaching, lead laboratory exercises (hands-on microscopy of parasites in blood, stool and urine), and give lectures. The curriculum (60 CME hours) covers the epidemiology, clinical manifestations, diagnosis, treatment, prevention and control of Africa's most important tropical infectious diseases. In addition, the participants gain insight into the local healthcare system and explore the fantastic scenery and prolific flora and fauna in East Africa during epidemiologic field excursions. In the colonial atmosphere of the lodge, Dr. Schaefer outlined the planned course of the trip. He described the itinerary taking us from Arusha to Karatu in the Ngorongoro Conservation Area, continuing on to Lake Eyasi in the East African Rift Valley and then back to Arusha. This would cover approximately 450 miles in comfortable 4x4 extended Land-Cruisers with safe, experienced local drivers. During the second week we were to travel by plane from Arusha to Zanzibar to visit hospitals, clinics and field projects. The next morning, we discussed malaria. Dr. Schaefer emphasized that malaria tropica (Plasmodium falciparum) is a medical emergency. Cerebral malaria can kill within a matter of hours. For this reason alone, doctors in the US and Europe should ask each patient with a fever if he or she has visited the tropics within the past 6 months. Later that same day we saw how life-threatening cerebral malaria can be, in an 8-month-old boy with convulsions and a fever of 104° F, admitted to the pediatric unit at the St. Elisabeth Hospital in Arusha (Photo 1). He immediately received IV dextrose solution and diazepam. With the help of a paracetamol suppository and fanning motions, a nurse tried to reduce the fever. Afterwards, the attending physician examined him and took a thin blood smear, explaining "It is much more important to stabilize the life-threatening condition, before any thought can be given to a diagnosis. Anyway, in most cases, it's malaria. Nevertheless, one should at least consider the possibility of meningitis, and perform a lumbar puncture in case the malaria therapy with quinine doesn't take effect." During the rainy season, the Anopheles mosquitoes breed very rapidly, and a distinct rise in malaria cases can be seen in hospitals, above all in the pediatric wards. Malaria tropica is still the number one killer of children under the age of 5 years in Africa. A most important progress in malaria control is the development and distribution of impregnated bed nets. We visited a production facility on the outskirts of Arusha (Photo 2). The nets' fibers are permeated with Permethrin, a "knock-down" repellent, creating a physical and also chemical barrier against the mosquitoes. The French entomologist Dr. Kouchner, who works in the area, assured us that this protection lasts for at least 5 years - even after multiple washings. The bed nets are manufactured in several sizes and are used in different malaria control projects worldwide with great success, according to the World Health Organization. Father Pat Patten is priest, physician and pilot all rolled into one. Over 30 years ago this American founded the Flying Medical Service (FMS) at the foot of nearby Mount Meru (15,000 ft). With small planes, healthcare workers reach very remote regions, otherwise inaccessible. We visited the headquarters of this small donation-funded organization. Two physicians from our group had the opportunity to spend two days with an FMS team. In outlying Maasai villages they examined pregnant women and inoculated small children. After their return, everyone wanted to learn about their experience. "A complete and utter contrast to our high-tech medicine in Europe. It's incredible how people can be helped with so little equipment and medication," said Dr. Pöttgen from Frankfurt. Along the journey toward Tarangire National Park we drove through a vast steppe landscape where sleeping sickness is endemic. After a lecture by Dr. Chalamka on human African trypanosomiasis in Magugu Hospital, we visited the wards. On a rusty pallet lay a 30-year-old man with severe meningoencephalitis. The day before he had been diagnosed with sleeping sickness. At his bedside, we discussed with Dr. Chalamka the advantages and disadvantages of Melarsoprol therapy, a highly toxic arsenic compound. He concluded by informing us that "with increasing frequency, tourists in East African national parks are being bitten by the tsetse fly. Regarding differential diagnosis, travellers to tropical regions returning home with a fever should be examined for malaria as well as sleeping sickness, insofar as they have visited endemic areas. Both diseases can be detected in a thin blood smear." In a field laboratory, we learned this important technique (Photo 3). The day ended with a field excursion through the Lake Manyara National Park, where we ventured into the habitat of antelopes - the main reservoir of the Trypanosomiasis rhodesiense parasite. An experienced public health expert and an entomologist from the Ministry of Health in Tanzania explained the control measures taken in surrounding villages. The following morning, we travelled along the edge of the magnificent Ngorongoro Crater (UNESCO World Heritage), reaching the Endulen Mission Hospital, staffed by a Dutch physician. She described the brucellosis cases, also known as undulant fever, which are often seen in the hospital. The patients complain of sudden fever and enlargement of the spleen and liver. The treatment calls for doxycycline and streptomycin. "Unfortunately, the patients, primarily the Maasai, return after a while with the same symptoms. They seem to have difficulty making a habit of cooking (pasteurizing) their cow's milk before drinking it, and therefore they infect themselves over and over again." As in the other hospitals we visited, we saw patients with pneumonia, AIDS, tuberculosis, malnutrition, and infants with diarrhea and dehydration.
As we drove across the sweeping Serengeti steppe and over to the Olduvai Gorge (the Cradle of Mankind), I observed the tall Maasai warriors with their cattle herds or trekking great distances across the arid plain in the heat of the day. Today the Maasai live as they have for centuries and are apparently not interested in changing their lifestyle. At the Meserani Snake Park in Arusha, we saw many live venomous African snakes about which Dr. Schaefer had lectured the prior evening. Snakes usually avoid humans and retreat into hiding when disturbed. On the other hand, the puff adder is fairly sluggish and is therefore most often a threat when approached. Then there is the black mamba, by far the quickest and most poisonous snake in Africa. Its neurotoxic venom paralyzes the respiratory muscles and can lead to death by suffocation within minutes. The owner of the snake park, Dr. Berry Bale, is widely known as a snake expert. In return for snakes taken to him by the locals, he produces and provides antivenoms and also teaches about correct treatment following bites. In the early evening we boarded our plane to fly from Arusha to Zanzibar. A hot and humid climate welcomed us when we arrived. The pelting tropical rain evaporated on the asphalt runway. Dr. Jiddawi, assistant minister for health in Zanzibar, received us in the modest arrival hall with a hearty "Inshallah." He is, as are most Zanzibaris, a devout practicing Muslim. The drive from the airport to our hotel north of Stone Town (another UNESCO World Heritage site) was like an enchanted journey through the One Thousand and One Nights. Along the roadside, merchants hawked their wares by candlelight. In their faces I recognized traces of Africa, India, Arabia and Europe. Our bus driver informed us that most of them are in fact Zanzibaris, and that the population has mixed with other races and peoples over the centuries. What unites them is Islam and the Kiswahili language. After the morning prayer, Dr. Khalfan, director of the Schistosomiasis/Elephantiasis Institute, welcomed us in his office in Stone Town. From here he coordinates prevention and control projects on Zanzibar. He is rightfully proud to report to us that in 2008, hardly any new cases of lymphatic filariasis were registered on Zanzibar after mass drug administration. Zanzibar was the first area to complete five rounds of treatment for the entire population using a combination of albendazole and ivermectin, reducing both the prevalence and intensity of Wuchereria bancrofti. "Factors crucial to its success include high-level political commitment, the development of appropriate social mobilization strategies, the involvement of communities in drug distribution, and the introduction of morbidity management for individuals with lymphedema. Unfortunately, with Schistosomiasis we're not that far along yet," he commented. During the drive to a school in Kinyasini in the northern part of Zanzibar, Dr. Khalfan explained why this is so. "It's mainly because the schoolchildren bathe during the day in ponds and rivers. They get infected, they are treated, and then they infect themselves all over again when they jump in the water. It's a vicious circle." An hour later we witnessed this phenomenon as we drove past a group of children in the midday heat - over 90° F (32° C), with relatively high humidity - splashing or doing their wash in a creek (Photo 4). Here they come in close contact with freshwater snails, the intermediate host for Schistosoma haematobium, hundreds of whose shells we found in the surrounding reeds. It is no surprise to learn that infection with urinary schistosomiasis is extremely high here. It wasn't easy to bid farewell to our colleagues. Over the course of the past two weeks, we grew together as a family, learning from each other as well as from the course. We had covered the better part of all major tropical infectious diseases, in a wide variety of hospitals, clinics and research centers. On numerous excursions we gained familiarity and appreciation not only for the Tanzanian healthcare system and its public health challenges but the land, the people and the extraordinary flora and fauna. (Formerly CDC, US Public Health Services), Watsonville, California, USA, Source: http://www.istm.org/
5. Verifiche oggettive: analisi dei dati 5.1 Il tema della misurazione della Follia e della classificazione dei disturbi Psichiatrici Nel ‘700, l’Illuminismo apre la strada ai metodi di ricerca scientifica in Psichiatria, come accade anche in tutti gli altri campi del sapere e del conoscere. A cominciare dalla ben nota Frenologia1 (secondo la quale le singole funzioni psichiche dipenderebbe
Patient Instructions for Admit Day of Procedure (Peter Lougheed Centre) Admit Day of Procedure (ADOP) refers to a person being admitted to hospital on the day of their surgery or procedure. Unless your doctor has given you other instructions to prepare you for your procedure, please follow the instructions below. To fi nd out the time of your surgery, please phone the hospital the day befo
 Report of my experiences with a tropical medicine expedition
Report of my experiences with a tropical medicine expedition