Hand Surgery, Vol. 11, No. 3 (2006) 1–4
TRANSDERMAL ANAESTHESIA FOR PERCUTANEOUS TRIGGER FINGER RELEASE Laboratory for the Research of the Musculoskeletal SystemUniversity of Athens, Athens, GreeceDepartment of Hand Surgery and MicrosurgerKifissia, 15125 Athens, Greece
Received 19 June 2005; Accepted 10 November 2006
ABSTRACT
The purpose of this study was to evaluate the safety and efficiency of transdermal anaesthesia using eutectic mixture of lidocaineand prilocaine (EMLA) in patients undergoing percutaneous trigger finger release and to compare it with lidocaine infiltration.
In this prospective, randomised study percutaneous release of the A1 annular pulley was performed to treat stenosing tenosynovitis
(trigger finger syndrome) in 50 patients (50 fingers). The procedure was performed either under transdermal anaesthesia usingEMLA applied transcutaneously 120 minutes prior to the operation (Group A, n = 25) or using local infiltration anaesthesia usinglidocaine (Group B, n = 25). Pain experienced during administration of anaesthesia and during the operation was assessed usinga 10-point Visual Analogue Pain Scale (VAPS), while all patients rated the effectiveness of anaesthesia with a 5-point scale.
There were no significant differences between the two groups in the VAPS during the operation (1.33 ± 0.52 versus 1.59 ± 0.87)
and the satisfaction scores (4.6 ± 0.2 versus 4.4 ± 0.3). The VAPS score during the administration of anaesthesia was statisticallysignificantly less in the EMLA group (0 versus 5.96 ± 2.41). All patients were satisfied with the final result of the operation.
Percutaneous trigger finger release can be performed as an office procedure with the use of EMLA avoiding the use of injectable
Keywords: Anaesthesia; Eutectic Mixture of Lidocaine and Prilocaine; Percutaneous Release; Trigger Finger.
Correspondence to: Dr. Christos K. Yiannakopoulos, Byzantiou 2, 171 21 Nea Smyrni, Athens, Greece. Tel: (+30) 697-209-9911, Fax: (+30) 210-363-6181,
C. K. Yiannakopoulos & I. A. IgnatiadisINTRODUCTION Table 1 Patient Demographic and Results.
Surgical release of the A1 annular pulley is recommended
when conservative treatment of trigger finger syndrome has
n = 25 n = 25
failed. The release can be performed either as an open pro-
cedure or percutaneously with success and without serious
complications.1 With either technique the use of local injectable
anaesthesia is necessary. Local anaesthesia is accompanied
with injection pain and occasionally with systemic symptoms
attributed to the absorption of the local anaesthetic used, usu-
ally lidocaine. EMLA® cream (Astra Zeneca, Halandri, Athens,
Greece) is used in patients of almost every age, from neonates
to geriatric patients, to provide transcutaneous anaesthesia
which enables the performance of a variety of procedures and
operations, including arterial and venous cannulation, split
VAPS = Visual analogue pain scale; EMLA = Eutectic mixture of local
thickness skin grafting, mechanical ulcer debridement, carpal
tunnel syndrome anaesthesia, prevention of acute and chronicpain etc.2–7
The purpose of this study was to investigate the safety and
landmarks on the skin of the palm were marked, the skin was
efficacy of EMLA cream as an alternative method of local anaes-
cleaned and the finger MCP joint was held in hyperextension
thesia in percutaneous trigger finger release and to compare it
by an assistant. The proximal and distal ends of the A1 pul-
ley were determined and marked using surface landmarks.8The position of the needle was confirmed by asking the patientto flex and extend the corresponding finger. Intratendinous
MATERIALS AND METHODS
position of the needle caused mild pain. The proximal end
A prospective, randomised trial was performed including
and the stoma of the A1 pulley were identified with palpation
50 patients with stenosing tenosynovitis (trigger finger syn-
and release was performed in a proximal to distal direction. A
drome), who underwent percutaneous A1 pulley release. The
typical grating sound and a similar sensation during A1 pul-
study was approved from the Ethics and Research Commit-
ley release ensured the success of the release. The patient
tee of our Institution. All patients had a palpable, tender
was asked to flex and extend the finger. Absence of trigger-
tendon nodule and characteristic mechanical triggering. On
ing was regarded as a sign of complete release. The wound
the whole, 50 trigger fingers were treated surgically. The
was covered with a soft compressive bandage and the patient
patients were randomly allocated in two Groups. In Group A
was advised to keep his/her hand elevated for 48 hours, while
(n = 25) skin anaesthesia was provided using EMLA and in
active finger motion was encouraged as soon as the patient was
Group B (n = 25) the skin was infiltrated with 3 ml lidocaine
1%. The demographical data of all patients are presented in
Pain experienced during the administration of anaesthesia and
during the operation was assessed by an independent research
The patient arrived at the office two and a half hours prior
nurse using a 10-point Visual Analogue Pain Scale (VAPS), while
to the scheduled operation time, where a thick layer of 5 mg
all patients rated the effectiveness of anaesthesia during the
EMLA® cream was applied on the palmar skin correspond-
procedure on a 5-point scale. A score of 1 was considered as a
ing to the location of the A1 pulley to be released and the
measure of insufficient anaesthesia and a score of 5 as a measure
cream was then covered with an occlusive dressing (Tega-
of excellent anaesthesia. Normally distributed continuous data
derm, 3M, St. Paul, MN). The dressing was removed prior
were analysed with a paired Student’s t-test and categorical data
to the operation and the cream was wiped off. The opera-
were analysed with the chi-square test with Yates’ continuity
tions were performed under forearm tourniquet using the tip
correction. A p value of <0.05 was considered statistically
of an 18-gauge needle, mounted on a 3 ml syringe. The surface
Transdermal Anaesthesia for Percutaneous Trigger Finger ReleaseDISCUSSION
The average duration of the operation in Groups A and B was
Percutaneous trigger finger release is a safe procedure and its
3.2 ± 1.5 and 3.4 ± 1.2 minutes, respectively and no case had
efficacy has been proved by clinical and cadaveric studies.9–11
to be cancelled because of insufficient anaesthesia (Table 1).
Complications following surgical management of trigger fin-
The two groups did not differ significantly in age, sex and finger
ger are not very common but when occurring they may be
operated. There were no significant intraoperative complica-
severe.11,12 The most important complications are digital nerve
tions or any recurrences. There were no infections, nerve or
transection, inadvertent A2 pulley release and tendon bow-
vessel injuries or incomplete pulley release. Skin blanching was
stringing. Complications such as scar tenderness, infection,
noted in four patients upon removal of the occlusive dressing
haematoma and stiffness may be more common after an open
in Group A. There were no significant differences between the
procedure, while complications such as digital nerve injury or
two groups in the VAPS during the operation and satisfaction
tendon bowstringing may appear both after open and percuta-
scores (Fig. 1). The difference in the VAPS score during admin-
neous procedures. Probably, the most common complications
istration of anaesthesia was statistically significant in favour of
after percutaneous release using a needle are incomplete release
the EMLA group. The VAPS score for anaesthesia was in the
and flexor tendon injury. The first complication can be pre-
EMLA group 0, while in the infiltration group 5.96 ± 2.41.
vented if complete resolution of triggering is ascertained with
The mean VAPS score, representing the level of pain during
finger movement. The second complication is usually not sig-
the operation was in Group A 1.33 ± 0.52 and in Group B
nificant and can be avoided with a meticulous technique and
1.59 ± 0.87. This difference was not significant. All patients
who received infiltration anaesthesia considered the injection
Local anaesthetics are used whenever a surgical procedure or
as the most painful part of the procedure. The patients were
intervention is going to cause pain and discomfort to the patient.
reviewed one, six and 12 weeks after the operation. All patients
The most common hand operations are carpal tunnel decom-
returned to work and their previous activities within two days.
pression and trigger finger release, which is performed as office
Full unobstructed range of finger flexion was obtained and the
procedures under local anaesthesia. Local anaesthesia can be
final cosmetic result was excellent. In most patients, only a small
performed using an appropriate local anaesthetic agent admin-
spot of skin discolouration could be noted at the site of the nee-
istered in three ways: topical application, local infiltration and
dle insertion. All patients were satisfied with the final result of
field block.11 Infiltration anaesthesia is effective but has the dis-
advantage of painful and uncomfortable injections, especiallywhen large or sensitive areas are to be anaesthetised. Localinfiltration anaesthesia may also have several complications:anaesthesia failure, pain or burning on injection, haematoma,infection, persistent anaesthesia, overdose, hypersensivity reac-tions, etc.2,11 EMLA, an acronym for Eutectic Mixture of LocalAnesthetics containing lidocaine 2.5% and prilocaine 2.5%, canbe used prior to local anaesthetic infiltration to reduce painassociated with procedures such as carpal tunnel syndromeand prominent ear correction.2,12
With the use of EMLA percutaneous trigger finger release can
be performed easily and safely in the outpatient clinic or inthe office, reducing the costs of surgical treatment. The onlydisadvantage is the need to apply the cream at least 120 minutesprior to the operation to optimise its effectiveness. In our study,EMLA has provided adequate anaesthesia to perform percu-taneous release and was well tolerated. The most importantlimitations in the use of EMLA is the delay necessary to obtain
Fig. 1 The VAPS scores between Groups A and B (*p < 0.05).
anaesthesia since skin penetration of topical anaesthetics is
C. K. Yiannakopoulos & I. A. Ignatiadis
time-dependent and the limited depth of dermal anaesthesia,
5. Lawrence T, Desai VV, Topical anaesthesia to reduce pain associated with
which is approximately 5 mm after 90 minutes.13
carpal tunnel surgery, J Hand Surg [Br] 27:462–464, 2002.
EMLA use is virtually complication-free and the most com-
6. Olday SJ, Walpole R, Wang JY, Radial artery cannulation: topical ametho-
caine gel versus lidocaine infiltration, Br J Anaesth 88:580–582,
mon side-effect is transient skin blanching noted upon removal
of the dressing.14 Blood levels of lidocaine and prilocaine
7. Wahlgren CF, Lillieborg S, Split-skin grafting with lidocaine-prilocaine
after application of EMLA cream are well below toxic levels.15
cream: a meta-analysis of efficacy and safety in geriatric versus non-
Methaemoglobinaemia attributed to a metabolite of prilocaine
geriatric patients, Plast Reconstr Surg 107:750–756, 2001.
prohibits its use in infants younger than six months.16
8. Wilhelmi BJ, Snyder N, Verbesey JE, Ganchi PA, Lee WP, Trigger finger
In conclusion, release using EMLA anaesthesia is safe, non-
release with hand surface landmark ratios: an anatomic and clinical study, Plast Reconstr Surg 108:908–915, 2001.
invasive and more comfortable than infiltration anaesthesia. The
9. Bain GI, Turnbull J, Charles MN, Roth JH, Richards RS, Percutaneous
major drawback is the necessity to apply the cream at least
A1 pulley release: a cadaveric study, J Hand Surg [Am] 20:781–784,
120 minutes before the operation. The two to three hours of
extra time may be a substantial inconvenience for many patients
10. Eastwood DM, Gupta KJ, Johnson DP, Percutaneous release of the trigger
and this should be discussed with them before scheduling the
finger: an office procedure, J Hand Surg [Am] 17:114–117, 1992.
11. Smith DW, Peterson MR, DeBerard SC, Local anesthesia. Topical appli-
cation, local infiltration, and field block, Postgrad Med 106:57–60, 1999.
12. Slator R, Goodacre TE, EMLA cream on the ears — is it effective? A
References
prospective, randomised controlled trial of the efficacy of topical anaes-
1. Benson LS, Ptaszek AJ, Injection versus surgery in the treatment of trigger
thetic cream in reducing the pain of local anaesthetic infiltration for
finger, J Hand Surg [Am] 22:138–144, 1997.
prominent ear correction, Br J Plast Surg 48:150–153, 1995.
2. Avramidis K, Lewis JC, Gallagher P, Reduction in pain associated with open
13. Bjerring P, Arendt-Nielsen L, Depth and duration of skin analgesia to
carpal tunnel decompression, J Hand Surg [Br] 25:147–149, 2001.
needle insertion after topical application, Br J Anaesth 64:173–177,
3. Galinkin JL, Rose JB, Harris K, Watcha MF, Lidocaine iontophoresis versus
eutectic mixture of local anesthetics (EMLA) for IV placement in children,
14. Stymne B, Lillieborg S, Plasma concentrations of lignocaine and prilocaine
Anesth Analg 94:1484–1488, 2002.
after a 24-hour application of analgesic cream (EMLA) to leg ulcers, Br J
4. Lok C, Paul C, Amblard P, Bessis D, Debure C, Faivre B, Guillot B, Ortonne
Dermatol 145:530–534, 2001.
JP, Huledal G, Kalis B, EMLA cream as a topical anesthetic for the repeated
15. Buckley MM, Benfield P, Eutectic lidocaine/prilocaine cream. A review
mechanical debridement of venous leg ulcers: a double-blind, placebo-
of the topical anaesthetic/analgesic efficacy of a eutectic mixture of local
controlled study, J Am Acad Dermatol 40:208–213, 1999.
anaesthetics (EMLA), Drugs 46:126–151, 1993.
Campo Grande, MS. Quarta, 09 de Abril de 2008. 3. PLANOS DE TRABALHO DO PROJETO 3 -1. IDENTIFICAÇÃO DO ACADÊMICO Acadêmico: 187 - PSICOLOGIA -FORMAÇÃO DE PSICÓLOGO 3 -2. IDENTIFICAÇÃO DO PLANO DE TRABALHO Título: Efeito de antagonistas de receptores de adenosina, sobre o nível de ansiedade de camundongos. adenosina, ansiedade, labirinto em cruz elevado 3 -3. P
Cancer & Blood Type Prepared by Dr Jason Mallia, Doctor of Integrative Medicine (Australia) What is contained here to be treated as information only and not misconstrued for professional advice. Please consult your health practitioner for more information. So what is the mainstream understanding of cancer? Cancer is a general term for a group of diseases characterized by abnormal gr
 Hand Surgery, Vol. 11, No. 3 (2006) 1–4
TRANSDERMAL ANAESTHESIA FOR PERCUTANEOUS
Hand Surgery, Vol. 11, No. 3 (2006) 1–4
TRANSDERMAL ANAESTHESIA FOR PERCUTANEOUS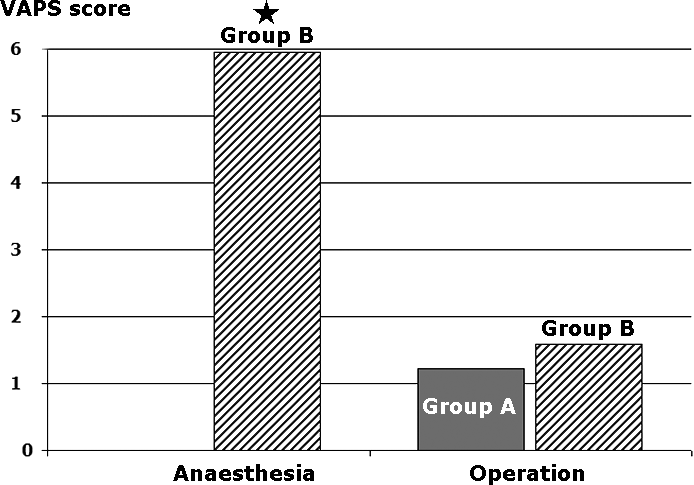 Transdermal Anaesthesia for Percutaneous Trigger Finger Release
DISCUSSION
Transdermal Anaesthesia for Percutaneous Trigger Finger Release
DISCUSSION