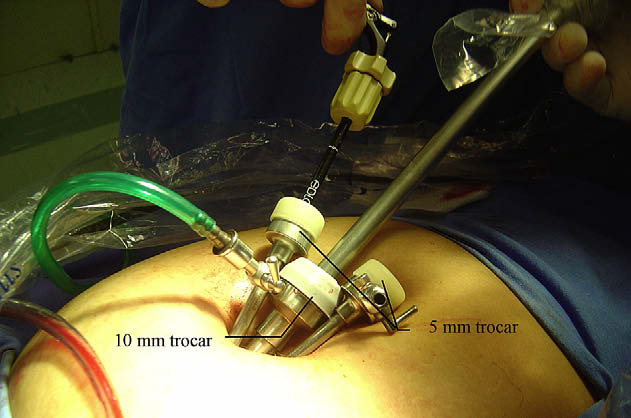
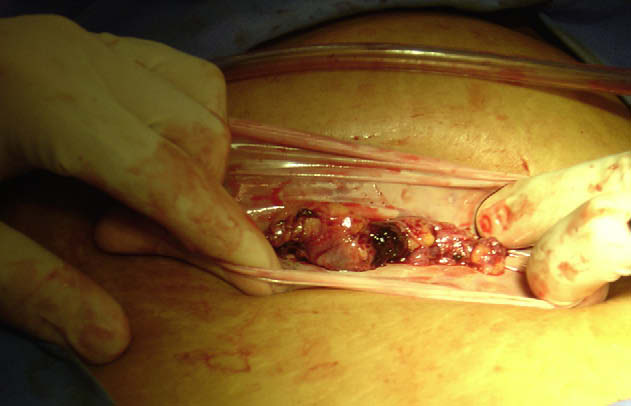
 Savaris. Ectopic pregnancy managed with LESS technique. Fertil Steril 2009.
Savaris. Ectopic pregnancy managed with LESS technique. Fertil Steril 2009.reid.org.br
TERMO INICIAL DA PRESCRIÇÃO NOS CRIMES SExUAIS CONTRA CRIANÇAS E ADOLESCENTES: O AR TERMO INICIAL DA PRESCRIÇÃO NOS CRIMES SEXUAIS CONTRA CRIANÇAS E ADOLESCENTES: O ART. 111, V, DO CP (LEI 12.650/2012) Publicada na edição de 18.05.2012 do Diá-rio Oficial da União e de aplicação imediata , a Lei 12.650 trouxe nova hipótese de termo inicial texto para discussão recebido em