Microsoft word - final report wcb project july05-dec07rev26march08.doc
Final Report: WorkSafeBC Project RS2003/04-022
Original Project Title: Evaluation of electronically recorded peak flow monitoring and weekly change in spirometry as substitutes for inhalation challenge testing in red cedar asthma. However, as explained in Research Problem subsection in the main body of the report, the project was revised to evaluate: The use of induced sputum as an additional diagnostic indicator of an asthmatic reaction to red cedar after specific inhalation challenge testing. Investigators: Raja T. Abboud MD FRCPC, Professor Emeritus, and Moira Chan-Yeung MD FRCPC, Professor Emeritus, Respiratory Division, UBC Dep’t of Medicine, at VGH, 7th Floor 2775 Laurel St, Vancouver, V5Z 3J5, phone 604-875-4122, Fax 604-875-4695 Date of Final Revision: 26 March 2008 Research Period Covered: June 2005 - Dec 2007
1. MAIN RESEARCH FINDINGS: • The aim of this study was to evaluate biomarkers of asthma activation in induced sputum
before and after specific inhalation challenge testing with plicatic acid, to determine which biomarkers would be useful in confirming occupational asthma, when applied to workers both during work exposure and off work.
• In a total of 19 subjects with suspected red cedar asthma having red cedar inhalation
challenge testing, sputum was induced with hypertonic saline about 6 hours after methacholine challenge on the control day and about 6 hours after plicatic acid inhalation challenge the next day.
• Eleven subjects developed bronchoconstriction after plicatic acid (Reactors), confirming
the diagnosis of red cedar asthma, while 8 did not (Non-reactors), excluding red cedar asthma. In Reactors, after plicatic acid inhalation compared to control day, median values of sputum eosinophils increased from 6.5% to 25.0%, eosinophil cationic protein (ECP) increased from 260 to 456 ng/ml, and eotaxin from 58 to 133 pg/ml (p<0.01), but LTB4 and LTC4 did not increase significantly. There were no significant changes in eosinophil counts. ECP, eotaxin, LTB4, or LTC4 in Non-reactors.
• Conclusions:
o 1. The markers of eosinophil activation, ECP and eotaxin, in induced sputum are
better indicators of a positive reaction to specific inhalation challenge in red cedar asthma than leukotrienes.
o 2. The results suggest that sputum induction while subjects are working and after
being off work for 2 weeks, to evaluate changes in eosinophil counts and %, as well as eotaxin, could confirm the diagnosis of red cedar asthma and reduce the requirement for red cedar inhalation challenge testing.
All rights reserved. The Workers’ Compensation Board of B.C. encourages
the copying, reproduction, and distribution of this document to promote
health and safety in the workplace, provided that the Workers’
Compensation Board of B.C. is acknowledged. However, no part of this
publication may be copied, reproduced, or distributed for profit or other
commercial enterprise or may be incorporated into any other publication
without written permission of the Workers’ Compensation Board of B.C.
Additional copies of this publication may be obtained by contacting:
Phone (604) 244-6300 / Fax (604) 244-6295
Final Report: WorkSafeBC Project RS2003/04-022
2. EXECUTIVE SUMMARY Western red cedar asthma is the most common occupational asthma in British Columbia, Canada. Diagnosis usually requires confirmation by the demonstration of immediate or delayed bronchoconstriction to inhalation of plicatic acid, the low molecular weight compound in red cedar wood implicated as the agent causing the asthma. The cedar inhalation challenge procedure requires 2½ days of testing, usually starting on Monday after the subject has been off work over the weekend. Subjects’ asthma should be stable off inhaled bronchodilators, but inhaled corticosteroids are allowed to keep the asthma stable for testing. On the first day of the cedar challenge testing, methacholine inhalation challenge is performed to determine non-specific bronchial reactivity, and spirometry and peak flow are followed in the Clinic Lab hourly for at least 6 hours after challenge. This serves a control day for the next day, when subjects are challenged with purified red cedar extract (plicatic acid). The subject monitors peak flow hourly at home until sleep time, and again the next morning on awakening and before leaving home; these again serve as control measurements for the 2nd day, the red cedar challenge day. On the 2nd day the subject is challenged with inhalation of plicatic acid and spirometry is followed every 10 minutes for the first hour to detect an immediate reaction, and then spirometry and peak flow are checked hourly for up to 6-7 hours to detect a sustained or delayed reaction. Again, subject monitors peak flow in the evening at home, and the next morning at home. Subject returns to the Clinic on the morning of the 3rd for recheck of spirometry and keep flow, and for reviewing test results. The aim of this study was to evaluate biomarkers of asthma activation in induced sputum before and after specific inhalation challenge testing with plicatic acid, to determine which biomarkers would be useful in confirming occupational asthma, when applied to workers both during work exposure and off work.
During the study period, a total of 42 subjects were evaluated for suspected red cedar asthma by red cedar inhalation challenge testing. Out of these 42, 22 subjects consented to take part in the research study by having induced sputum on the control day and again on the red cedar extract (plicatic acid) challenge day, yielding a participation rate of 52 %. Sputum was induced with hypertonic saline about 6 hours after methacholine on the control day and about 6 hours after plicatic acid the next day. However induced sputum samples were not obtained on the plicatic acid challenge day in 3 subjects, leaving 19 subjects who had sputum induction before and after cedar challenge. Eleven subjects developed bronchoconstriction after plicatic acid (Reactors), confirming the diagnosis of red cedar asthma, while 8 did not (Non-reactors), excluding red cedar asthma. In one reactor, the sputum sample was frozen during transportation to the processing laboratory, leaving 18 subjects (10 Reactors and 8 Non-reactors) for comparison of sputum results before and after cedar challenge. We determined cell counts and differential cell staining, and assayed eosinophil cationic protein (ECP), the leukotrienes LTB4 and LTC4, and eotaxin by specific ELISA. In Reactors, after plicatic acid inhalation compared with control day, median values of sputum eosinophils increased from 6.5% to 25.0% (p<0.001), there was a trend for an increase in ECP from 260 to 456 ng/ml, and eotaxin increased from 58 to 133 pg/ml (p<0.001). However, there was no consistent change in LTB4 and LTC4. Non-reactors had no consistent changes in any parameter.
Final Report: WorkSafeBC Project RS2003/04-022
We conclude that the markers of eosinophil activation, increased eosinophil counts and as % of cells, and increase in ECP and eotaxin, in induced sputum are better indicators of a positive reaction to specific inhalation challenge in red cedar asthma than leukotrienes. The results suggest that sputum induction while subjects are working and after being off work for 2 weeks, to evaluate changes in eosinophil counts and %, as well as eotaxin, could confirm the diagnosis of red cedar asthma and reduce the requirement for red cedar inhalation challenge testing.
Final Report: WorkSafeBC Project RS2003/04-022
3. MAIN BODY OF REPORT RESEARCH PROBLEM
The purpose of this research was to evaluate additional diagnostic procedures in evaluating red
cedar asthma to reduce the necessity for performing red cedar inhalation challenges. Although
the original title of this project indicates that the project was evaluating electronic peak flow
monitoring and weekly monitoring of spirometry in occupational asthma, this evaluation was
considered not feasible because there was a change in the referral pattern of subjects, with
decrease in the number of referred subjects and most were outside the greater Vancouver area.
The project was modified to evaluate the use of induced sputum (1,2), before and after specific
inhalation challenge testing, as an additional diagnostic indicator of an asthmatic reaction to red
The project required a longer period of subject recruitment than the initially projected 2 years,
for two reasons: 1) starting in 2003, there was a significant decline in the number of subjects
referred for evaluation of red cedar asthma, 2) the project could not start until July 2005, after the
UBC Ethics Board approved the use of induced sputum as a research procedure. The number of
subjects referred for red cedar inhalation challenge testing remained low in 2005 and 2006, but
the number increased significantly in 2007.
METHODOLOGY
Inhalation challenge testing for red cedar asthma. This follows the protocol standardized and
established previously in our department by Dr. Chan-Yeung (3). In brief subjects were tested
after being off work for at least 2 days, if their asthma was stable on treatment. They withheld
inhaled bronchodilators, but were kept on their usual dose of inhaled corticosteroid. On the
morning of the first day of testing they had methacholine inhalation testing to determine non-
Final Report: WorkSafeBC Project RS2003/04-022
specific bronchial reactivity. Their FEV1 was then checked hourly with a computerized table
top spirometer for at least 6 hr after completion of inhalation challenge; this served as a control
day for the cedar challenge the next day. Peak flow was determined with a Mini-Wright peak
flow meter hourly for the same time period, and then monitored hourly until sleep time, and then
The next day, specific inhalation challenge testing was done using 2 minute nebulizations of
plicatic acid (the compound in red cedar causing the asthma) starting at a concentration of 0.625
mg/ml with check of FEV1 at 0.5 and 10 minutes. If there was no reaction, inhalation challenge
and spirometry monitoring were repeated with nebulizations of doubling concentrations of
plicatic acid up to the highest concentration of 10 mg/ml. The inhalation challenge was stopped
if the subject developed a drop in FEV1 of 20% or greater, or after the nebulization of the highest
concentration of 10 mg/ml. FEV1 . Then FEV1 and peak flow were monitored hourly for up to 6-
7 hours after challenge. The patients then monitored their peak flow at home as on the previous
day. The next morning, their peak flow recordings and symptoms were reviewed, and peak flow
and FEV1 were checked in the Clinic. They were then informed of the results of the testing and
recommendations regarding work and treatment. A report was sent to the referring physician, to
Sputum induction as a research procedure. This was done after obtaining informed consent, and
follows the technique developed in McMaster University (6) and utilized with slight
modifications in our centre previously (1,5). The sputum induction was done 6 hrs after
completion of methacholine nebulization, and up to 6-7 hrs after the plicatic acid challenge
similar to previously (1), so as not to miss a late reaction. However, if the subject developed a
Final Report: WorkSafeBC Project RS2003/04-022
definite and sustained late reaction to plicatic acid, salbutamol inhalation would be given to
control the broncho-constriction and then sputum induction would be started. Induced sputum
was obtained after 7 minutes of nebulization of 3 % hypertonic saline, then 7 minutes of 4%
saline, then if required after a 3rd nebulization of 5% saline. The subject’s FEV1 was monitored
before and after each nebulization of hypertonic saline, and salbutamol by metered dose inhaler
was given if the FEV1 decreased by 10% or more. Sputum induction was stopped if the subject
produced adequate amounts of mucus or was bothered by the procedure.
Processing and Analysis of induced sputum samples. The sputum samples were kept on ice
packs and taken within 1½ hours to the Research Laboratory at St. Paul’s Hospital as no trained
technician was available at that time at VGH. The sample was processed throughout the study
by the same technician trained at McMaster University in their protocol (6). The mucus was
collected, weighed and suspended in dithiothreitol (DTT) solution to dissolve the mucus, and a
cell count was determined. Cytospin smears were prepared for staining to determine differential
cell counts. The mucus suspension was then centrifuged to obtain a cell free supernatant which
was frozen in aliquots at –70 o C for assay of asthma biomarkers. The remaining sample of
induced sputum was frozen at –70 o C for assay of biomarkers which might be affected by the
Subjects tested. Inhalation challenge testing for red cedar asthma for all subjects was approved
by WorkSafe BC, since the subjects’ time off work and the cost of the inhalation challenge
testing were covered by WCB. The research testing was approved by the University of B.C
Ethics Review Board, and informed consent was obtained from all subjects. In 2005 and 2006 a
total of 19 subjects had cedar inhalation challenge, of whom 9 consented to sputum induction for
research purposes. In 2007 there was a significant increase in referrals, and a total of 23 subjects
Final Report: WorkSafeBC Project RS2003/04-022
had red cedar inhalation challenge. Of these, 13 consented to having induced sputum. The total
number of subjects consenting to take part in the study was 22, out of a total of 42 subjects
having cedar inhalation challenge, yielding a participation rate of 52 %. However, sputum before
and after plicatic acid challenge was obtained in 19 subjects. Of these 11 reacted to plicatic acid
confirming the diagnosis of red cedar asthma , while 8 did not, virtually excluding the diagnosis.
However, in one subject (#5), the induced sputum sample on the control day was frozen during
transportation to the processing Lab, rendering it unusable. This left only 18 samples ( 10
reactors and 8 non-reactors) suitable for comparison before and after challenge.
The number of subjects having induced sputum to evaluate red cedar asthma before and after
challenge in this study, compares favourably with the two previous studies evaluating induced
sputum in occupational asthma, one from Dr. Chan-Yeung’s Lab in Vancouver (1) which
evaluated 17 subjects with red cedar asthma, and the other by Lemiere et al.(2) at McMaster
Difficulties /challenges encountered. The major difficulty encountered previously was the low
number of subjects referred for inhalation challenge for red cedar asthma during 2005 and 2006.
However the number of referrals improved in 2007, and 20 patients were referred during this
year, which is similar to our experience previously in 2002 and 2003. Another problem was the
low rate of subjects accepting sputum induction among those undergoing inhalation challenge
testing. This was partly due to a language barrier in some of the subjects making it difficult to
use the informed consent form written in English. We tried to overcome this by the use of
professional interpreters or family members to explain the procedures and the informed consent.
Final Report: WorkSafeBC Project RS2003/04-022
Analysis of Induced Sputum for markers of asthma activation. We used ELISA plates from MBL
Int’l Corp for analysis of eosinophil cationic protein (ECP), from Cayman Chemical Inc. for
analysis of LTB4 & LTC4 & cysteinyl leukotrienes (Cys-LT), and from R & D systems Inc. for
eotaxin, following the manufacturers’ procedure and standards, and as used in the literature (2, 7,
8). Samples and standards were done in duplicate; the assay was repeated with a different sample
volume if the result did not fall in the recommended range of the standard curve. We were able
to measure ECP, and LTB4 and LTC4 in the induced sputum samples treated with dithiethreitol
(DTT), but were unable to detect eotaxin. This is because the DTT treatment resulted in
degradation of eotaxin (9). However, we measured eotaxin in the remaining portions of the
induced sputum samples not treated with DTT.
A problem with the technique of induced sputum preparation is that the DTT treatment may lead
to disintegration of some biomarkers, and some mediators and cytokines may be completely lost
after this treatment (9). Recently a study suggested treating the induced sputum supernatants with
protease inhibitors to protect the biomarkers and removing the dithiothreitol by dialysis before
any assays or storage at –70 o C (10). However, this procedure is time consuming and not simple.
A simpler procedure which we have now followed is to process two samples of sputum from the
coughed out induced sample, one treated with DTT for the cell counts and differentials, and
another without DTT for measuring biomarkers, as used by other investigators on expectorated
Exhaled breath condensates (ECB). Collection of EBC has been suggested as a simple non-
invasive technique for evaluating biomarkers of asthma activation in the exhaled breath (13). The
technique is simple, where the subject breathes quietly for 10 to 20 minutes though a mouthpiece
Final Report: WorkSafeBC Project RS2003/04-022
and the exhaled breath passes into a cooling chamber, where the water vapor condenses, and the
fluid can be collected for analysis of biomarkers. We have started collecting EBC for assaying
bio-markers, such as eotaxin (14) and leukotrienes (15, 16) to indicate an asthmatic reaction.
Reported levels in the literature in EBC for eotaxin (14) and for leukotrienes (15,16) in subjects
with asthma were within the assay ranges of the ELISA kits we used. We used the system
developed by Respiratory Research Inc. (www.respiratoryresearch.com ; Charlottesville, Va,
USA) where the subject breathes quietly through a mouthpiece for at least 10 minutes, and the
exhaled breath passes through a plastic collection tube, cooled by a metal jacket previously kept
in a freezer, resulting in a collection of about 1.0 mL of fluid condensed from the breath over 10
minutes of quiet breathing. This is a very safe and well tolerated procedure without any risk. The
advantage of this technique is that it can be used in the field and does not require a specialized
laboratory for analysis within a few hours of sampling, as in the case of induced sputum, and the
sample can be collected and kept frozen for later analysis in Vancouver.
Can Induced Sputum testing be used as an alternate to specific inhalation challenge ?
A multicentre study of occupational asthma from Eastern Canada (17) reported that induced
sputum showed a reduction in eosinophils and eosinophil cationic protein in occupational asthma
after a 2 week period off work compared to that obtained during work. They suggested that if the
results of peak flow monitoring and induced sputum eosinophil counts at work and off work both
support the diagnosis of occupational asthma, the results may be an alternate to specific
inhalation challenge testing. In their study, they did not report the results of other markers of
eosinophil activation. If further studies indicate that the use of induced sputum biomarkers of
asthma activation as well as eosinophil counts, yields a high sensitivity and specificity in
Final Report: WorkSafeBC Project RS2003/04-022
diagnosing occupational asthma, it may be become applicable as a tool for evaluating suspected
occupational asthma at work and off work, without the need for inhalation challenge testing.
RESEARCH FINDINGS.
Table 1 compares mean data for subjects with confirmed red cedar asthma and that for subjects
who did not react to plicatic acid and consequently did not have red cedar asthma. There was no
significant difference in age, FEV1, atopic status. Only one subject with red cedar asthma was a
current smoker while 3 out of the 8 subjects with non-cedar asthma were current smokers.
The assays of induced sputum before and after plicatic acid challenge were completed in 18
subjects, because in one subject ( #5), the induced sputum sample prior to plicatic acid challenge
got frozen during transportation from our Clinic Lab to the Research Laboratory and was thus
rendered unusable for diagnostic purposes, and so an induced sputum sample prior to plicatic
acid challenge was not available for this subject. Instead, we obtained an induced sputum sample
28 hours after completion of the plicatic acid challenge when he had recovered from the
asthmatic reaction; this was compared with the sample obtained 6 hours after challenge during
the late asthmatic reaction, and the data for this subject are shown separately.
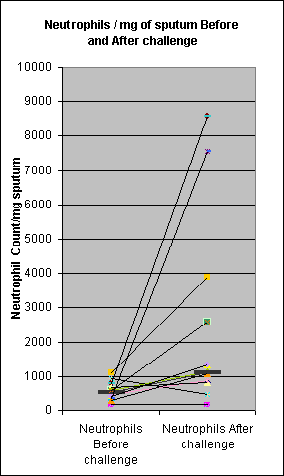
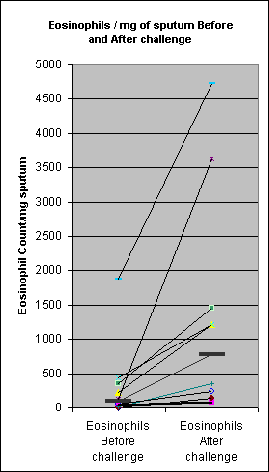
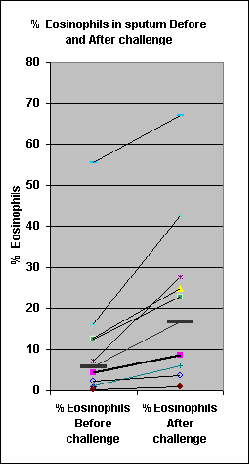
Fig 1 shows that was a significant increase in neutrophil counts (p<0.01) and eosinophil counts
and eosinophil percentage (p<0.001), all increased after plicatic acid challenge in patients with
red cedar asthma, compared with induced sputum results on the control day prior to plicatic acid
challenge, while there were no significant changes in the subjects who did not react to plicatic
acid (data not shown). Fig 2 (top panel) shows that eosinophil cationic protein increased in all
but 2 subjects having an asthmatic reaction to plicatic acid with an increase in the median values,
Final Report: WorkSafeBC Project RS2003/04-022
but the results were not statistically significant (Wilcoxon rank sign test). There was no
consistent change in LTB4. Median values for LTC4 were higher after PA challenge, but the
results were not statistically significant. There were no significant changes in the subjects who
did not react to plicatic acid (Fig 2, bottom panel).
Eotaxin could not be detected in the induced sputum samples treated with DTT. However we
measured eotaxin levels in the remaining part of the induced sputum sample not treated with
DTT, and simultaneously measured LTB4 to calculate the eotaxin/LTB4 ratio. Fig 3 shows that
in the subjects with red cedar asthma there was a significant increase (p< 0.001) in eotaxin
levels in induced sputum after plicatic acid challenge, while there were no significant changes in
LTB4. There was also a significant increase in the eotaxin/LTB4 ratio (p<0.001) after plicatic
The subject (# 5) whose baseline pre-challenge induced sputum was not usable for analysis
because it got frozen during transportation, reacted to plicatic acid challenge confirming the
diagnosis of red cedar asthma. He had high levels of neutrophil and eosinophil counts in induced
sputum as well as elevated ECP, LTB4, LTC4, and eotaxin levels 6 hours after challenge
(Table 2). All values except the ECP had decreased the next day when he was recovering from
his asthmatic reaction 28 hours after inhalation (Table 2). It is likely that ECP remained high,
presumably because he still had elevated eosinophils, which were releasing ECP. It is very likely
that his levels would have been even lower in the sputum obtained on the control day had it not
Final Report: WorkSafeBC Project RS2003/04-022
Our results indicate that evaluation of induced sputum provides confirmation of a positive
bronchial reaction to specific inhalation challenge testing in the diagnosis of occupational
asthma. Induced sputum results could provide additional evidence to support a positive reaction
to inhalation challenge testing in subjects who develop a borderline bronchial reaction (FEV1
response) to plicatic acid. The cell counts and differential cell counts showed a significant
increase in eosinophil counts in Reactors as compared to Non-reactors to red cedar asthma
extract. The majority of Reactors showed an increase in eosinophilic cationic protein (ECP), a
biomarker released from eosinophils. All reactors showed an increase in eotaxin, a chemo-
attractant for eosinophils released during the asthmatic reaction. There were no significant
increases in LTB4 or LTC4 following the late reaction to plicatic acid. The response in red cedar
asthma differs from that reported in isocyanate-induced asthma where there was release of LTB4
(7); however isocyanate asthma may initiate a predominantly neutrophilic rather than
Results of assays of asthma biomarkers in Exhaled Breath Condensates (EBC)
We were unable to detect eotaxin or leukotrienes in EBC of asthma subjects having a positive
reaction to plicatic acid . However, eotaxin and leukotienes in EBC were readily detected in
European centres (14-16), where EBC was collected by specialised apparatus (e.g. Jaeger Eco-
Screen), where the exhaled breath condenses in a flask kept cooled by a refrigerating unit. Failla
et al (16) reviewed the literature and reported median values for cysteinyl-leukotrienes (cys-LT)
of about 20 pg/ml in normal subjects, increasing to about 60 in allergic rhinitis, and higher to
about 70 in asthma. In contrast, Debley and co-workers (18), using the RT-Tube of Respiratory
Research (the system we tried) reported that EBC had to be concentrated 6 to 12 fold to enable
Final Report: WorkSafeBC Project RS2003/04-022
measurement of cys-LT; they reported median values in adults with mild asthma of 4.3 pg/ml
A possibility we considered was that there could be loss of biomarkers due to their adhesion to
the plastic collection tubes. We checked this, by comparing levels of biomarkers collected from a
few normal volunteers and asthma subjects, in tubes with and without prior coating with 1%
bovine serum albumin and 0.01% Tween 20, as recommended by two investigators from Sweden
(19). Preliminary results indicate that eotaxin was detectable at very low levels in
unconcentrated EBC collected in coated tubes but not in uncoated tubes from asthma patients,
indicating that coating prevents some loss of biomarkers. However, there may be other factors
affecting results collected by the RT tubes. Another possibility to be considered is that the
cooling effect of the metal jacket does not last long enough and is not sufficient to prevent
degradation of biomarkers during the 10 or 20 minutes of collection. More evaluation and quality
control procedures are needed to standardize the methodology of collecting EBC and its
reproducibility , before it can be applied for evaluation of occupational asthma. However, since
this is a non-invasive technique to obtain biomarkers from the respiratory tract, and since
European reports are encouraging, further research is warranted.
Induced sputum as a research procedure was obtained before and after plicatic acid challenge in
18 subjects undergoing inhalation challenge testing for suspected red cedar asthma. Ten subjects
had reacted to the inhalation challenge testing with a significant decrease in FEV1 confirming the
diagnosis of red cedar asthma, while 8 did not, virtually excluding the diagnosis. The reactors
showed an increase in neutrophil counts and highly significant increases in eosinophil counts and
Final Report: WorkSafeBC Project RS2003/04-022
% eosinophils in induced sputum after plicatic acid challenge. There was a trend for an increase
in eosinophilic cationic protein (ECP), and a highly significant increase in eotaxin, but no
significant increase in the leukotrienes LTB4 and LTC4. These results indicate that markers of
eosinophilic activation in induced sputum are better indicators of a positive asthmatic reaction to
IMPLICATIONS for FUTURE RESEARCH ON OCCUPATIONAL ASTHMA
Our results suggest that using the combination of changes in eosinophil counts and percentage of
cells, and eotaxin concentration, and possibly ECP before and after challenge would be good
indicators of predicting an asthmatic reaction to plicatic acid. We will obtain statistical
consultation to evaluate the sensitivity and specificity of these biomarkers separately and in
combination, in diagnosing red cedar asthma.
Establishing induced sputum at work and off work as an alternate to specific inhalation challenge
testing may require a trial comparing induced sputum results thus obtained, with subsequent
POLICY and PREVENTION
It appears from some workers’ descriptions that some mills have high dust levels and poor
ventilation and may not be meeting WorkSafeBC standards. This project was not specifically
designed to assess policy or prevention.
Final Report: WorkSafeBC Project RS2003/04-022
DISSEMINATION/KNOWLEDGE TRANSFER
R.A. presented this research project in detail at the UBC Wednesday (VGH-St Paul’s)
Respiratory Medicine Seminars on 19 March 2008, and it was well received and generated
interest in the use of induced sputum biomarkers as an alternate to specific inhalation challenge
testing. A poster is being presented at the “Lung Health Research and Policy Day” Meeting to be
held at the Sheraton Wall Center Hotel on 27 March 2008 (Abstract attached at end of this
report). An Abstract has been submitted to the European Respiratory Society for consideration
for presentation at their meeting in October 2008 in Berlin (Abstract attached at end). R.A. is
also planning to submit an Abstract for presentation to the Canadian Respiratory Clinical
Research Consortium Meeting held on 19 June 2008 in Montreal in conjunction with the 1st
Canadian Respiratory Conference 19-21 June 2008.
A paper will be prepared for submission to one of the prime journals in Respiratory Medicine. It
is planned to present the results of this study at a Canadian Lung Conference this summer and to
the European Respiratory Society in Berlin in October 2008. Copies of the published article will
Final Report: WorkSafeBC Project RS2003/04-022
References:
1. Obata H., Ditrrick M, Chan H, Chan-Yeung M. Sputum eosinophils and exhaled nitric oxide during
late asthmatic reaction in patients with red cedar asthma. Eur Respir J 1999; 13:489-495.
2. Lemiere C, Pizzichini MM, Balkissoon R, et al. Diagnosing occupational asthma. Eur Respir J 1999;
3. Chan-Yeung M, Lam S, Koerner S. Clinical features and natural history of occupational asthma due
to western red cedar (Thuja plicata). Am J Med 1982; 72:411-415.
4. Pin I, Gibson PJ, Kolendowicz R, et al. Use of induced sputum cell counts to investigate airway
inflammation in asthma. Thorax 1992; 47: 25-29.
5. Chan-Yeung M, Obata H, Dittrick M, Chan H, Abboud R. Airway inflammation, exhaled ntitric
oxide, and severity of asthma in patients with western red cedar asthma. Am J Respir Crit Care Med 1999; 159: 1434-1438.
6. Pizzichini E, Pizzichini MMM, Efthiniadis A, Hargreave FE, Dolovich J. Measurement of
inflammatory indices in induced sputum: effects of selection of sputum to minimize salivary contamination. Eur Respir J. 1996; 9:1174-1180.
7. Lemiere C, Pelissier S, Tremblay C, et al. Leukotrienes and isocyanate-induced asthma: a pilot study.
8. Yamada H, Yamaguchi M, Yamamoto K, et al. Eotaxin in induced sputum of asthmatics:
relationships with eosinophil cationic protein in sputum. Allergy 2000; 55:392-397.
9. Kelly MM, Keatings V, Leigh R, et al. Analysis of fluid phase mediators. Eur Respir J 2002;
10. Erin EM, Jenkins GR, Kon OM, et al. Optimized dialysis and protease inhibition of sputum
dithiothreitol supernatants. Am. J. Respir. Crit. Care Med 2008; 177:132-141.
11. Tsang KWT, Pak-Leung H, Wah-Kit L, et al. Inhaled fluticasone reduces sputum inflammatory
indices in severe bronchiectasis. Am J Respir Crit Care Med 1998; 158:723-727-727.
12. Woolhouse IS, Bayley DL, Stockley RA. Effect of sputum processing with dithiothreitol on the
detection of inflammatory mediators in chronic bronchitis and bronchiectasis. Thorax 2002; 57: 667-671.
13. Kharitonov SA, Barnes PJ. Exhaled biomarkers. Chest 2006; 160:1541-1546.
Final Report: WorkSafeBC Project RS2003/04-022
14. Ko FW, Lau CY, Leung TF, Lam CW, Lai CK, Hui DS. Exhaled breath condensate levels of eotaxin
and macrophage-derived chemokine in stable adult asthma patients. Clin Exp Allergy 2006; 36: 44-51.
15. Bucchioni E, Csoma Z, Allegra L, Chung KF, Barnes PJ, Kharitonov SA. Adenosine 5' –
monophosphate increases levels of leukotrienes in breath condensate in asthma. Respir Med 2004; 98:651-655.
16. Failla M, Crimi N, Vancheri C. Exhaled bronchial cysteinyl leukotrienes in allergic patients. Curr
Opin Allergy Clin Immunol 2007; 7:25-31.
17. Girard F, Chaboillez S, Cartier A, Côté J, Hargreave FE, Labrecque M, Malo JL , Tarlo SM,
Lemière C. An effective strategy to diagnose occupational asthma: use of induced sputum. Am J Respir Crit Care Med 2004;170:845-850.
18. Debley JS, Hallstrand TS, Monge T, et al. Methods to improve measurement of cysteinyl leukotrienes
in exhaled breath condensate from subjects with asthma and healthy controls. J Allergy Clin Immunol. 2007; 120:1216-1217.
19. Tufvesson B, Bjermer L. Methodological improvements for measuring eicosanoids and cytokines
in exhaled breath condensates. Respir Med 2006; 100: 34-38.
Final Report: WorkSafeBC Project RS2003/04-022
Table 1: Comparison of subjects with confirmed red cedar asthma reacting to plicatic acid challenge, and those with asthma not due to red cedar (negative challenge)
Baseline Lung Function FEV1 L Mean (SD)
Plicatic acid Challenge Positive Immediate Reaction %
Final Report: WorkSafeBC Project RS2003/04-022
Table 2: Induced sputum results in Subject # 5 with red cedar asthma, 6 hrs and 28 hrs after plicatic acid inhalation challenge.
Final Report: WorkSafeBC Project RS2003/04-022
Figure 1. Neutrophil count and eosinophil count in induced sputum in the patients with red cedar asthma before and after plicatic acid challenge. (Bars indicate median values) There was a significant increase in neutrophil (p<0.01) and eosinophil counts(p<0.001), and in the percentage of eosinophils (p<0.001) after plicatic acid challenge in the subjects reacting to plicatic acid. In contrast, there were no significant increases in neutrophil or eosinophil counts in the subjects who did not react to plicatic acid (data not shown). Figure 2. Eosinophil cationic protein (ECP), LTB4, and LTC4 in induced sputum in subjects with and without red cedar asthma, before and after inhalation challenge with plicatic acid. (Bars indicate median values) Top panel: subjects with confirmed red cedar asthma: There was a trend for an increase in ECP after inhalation challenge with plicatic acid, no change in LTB4, and a non-significant changes in LTC4. Bottom panel: subjects with asthma not due to red cedar: There was no consistent change in any of the mediators Figure 3 LTB4 and Eotaxin levels in induced sputum not treated with dithiothreitol, in subjects with red cedar asthma before and after plicatic acid challenge: There was no significant change in LTB4, but there was a statistically significant increase in eotaxin levels (p<0.001) and in the eotaxin/LTB4 ratio (p<0.001), after plicatic acid challenge in subjects with red cedar asthma.
Final Report: WorkSafeBC Project RS2003/04-022
Final Report: WorkSafeBC Project RS2003/04-022
Figure-2 ECP Before and After LTB4 Before & After LTC4 Before and After Challenge Challenge Challenge challenge challenge challenge challenge challenge challenge ECP, LTB4 and LTC4 in reactors ECP Before and After LTB4 Before & After LTC4 Before and After Challenge Challenge Challenge pg/ml 4 6000 challenge challenge challenge challenge challenge challenge ECP, LTB4 and LTC4 in non reactors
Final Report: WorkSafeBC Project RS2003/04-022
Figure 3. Eotaxin and LTB4 levels in induced sputum not treated with dithiothreitol. Eotaxin Before & After Eotaxin/LTB4 ratio Before LTB4 Before & After Challenge and After Challenge Challenge tio be a 0.1 Challenge Challenge Challenge Challenge Challenge Challenge
Final Report: WorkSafeBC Project RS2003/04-022
Abstract for Poster Presentation at Centre for Lung Health Research &Policy Day, 27 Mar 08, Sheraton Wall Centre Title: Eosinophil cationic protein and eotaxin are better biomarkers of asthma activation than leukotrienes in induced sputum after specific inhalation challenge testing in subjects with western red cedar asthma Authors: Raja Abboud MD FRCPC, Selvarani Vimalanathan, PhD, Moira Chan-Yeung MD FRCPC, Respiratory Medicine Division, University of British Columbia at Vancouver General Hospital, and Vancouver Coastal Health Research Institute, Vancouver, B.C. Abstract: Western red cedar asthma is the most common occupational asthma in British Columbia. The diagnosis is usually confirmed by the demonstration of immediate or delayed bronchoconstriction to inhalation of plicatic acid, the low molecular weight compound causing the asthma ( Chan-Yeung M, et al. Am J Med 1982; 72: 25-29). Our aim was to evaluate biomarkers of asthma activation in induced sputum before and after specific inhalation challenge testing with plicatic acid, to determine which biomarkers would be useful in confirming occupational red cedar asthma. Testing for these biomarkers in induced sputum in workers exposed to red cedar both during work exposure and off work, could then be used to confirm the diagnosis without performing the time consuming inhalation challenge test with plicatic acid and risking side effects. We studied a total of 18 subjects with suspected red cedar asthma who had specific inhalation challenge testing. Induced sputum was obtained after informed consent, by ultrasonic nebulization of hypertonic saline, 6 hours after methacholine on the control day, and 6 hours after plicatic acid the next day. Ten subjects developed bronchoconstriction after plicatic acid (Reactors), confirming the diagnosis of red cedar asthma, while 8 did not (Non-reactors) excluding the diagnosis. In Reactors, median values in induced sputum after plicatic acid inhalation compared to the control day increased as follows: sputum eosinophils from 6.5% to 25.0%, eosinophil cationic protein (ECP) from 260 to 456 ng/ml, and eotaxin from 58 to 133 pg/ml (p<0.01). However, there were no significant increases in the leukotrienes LTB4 and LTC4 . Non-reactors did not show any significant changes in any parameter. We conclude that the markers of eosinophil activation, ECP and eotaxin, are better biomarkers than leukotrienes of a positive reaction to specific inhalation challenge in red cedar asthma. Supported by a research grant from WorkSafeBC.
Final Report: WorkSafeBC Project RS2003/04-022
Abstract Submitted to European Respiratory Society Meeting Oct 2008 Title: Evaluation of biomarkers of asthma activation in induced sputum before and after specific inhalation challenge testing for western red cedar asthma Raja Abboud, [email protected], MD1,2, Selvarani Vimalanathan, [email protected],2 and Moira Chan-Yeung, [email protected], MD1,2. 1Medicine, Respiratory Division, University of British Columbia, Vancouver, B.C., Canada and 2Vancouver Coastal Health Research Institute, Vancouver General Hospital, Vancouver, B.C., Canada. Body: Western red cedar asthma is the most common occupational asthma in British Columbia, Canada. Diagnosis often requires confirmation by the demonstration of immediate or delayed bronchoconstriction to inhalation of plicatic acid, the low molecular weight compound implicated as the causative agent ( Chan-Yeung M, et al. Am J Med 1982; 72: 25-29). The aim of this study was to evaluate biomarkers of asthma activation in induced sputum before and after specific inhalation challenge testing with plicatic acid, to determine which biomarkers would be useful in confirming occupational asthma, when applied to workers both during work exposure and off work. Induced sputum was obtained after informed consent from a total of 18 subjects with suspected red cedar asthma having inhalation challenge testing. Sputum was induced with hypertonic saline 6 hours both after methacholine on the control day and plicatic acid the next day. Ten subjects developed bronchoconstriction after plicatic acid (Reactors), confirming the diagnosis of red cedar asthma, while 8 did not (Non-reactors). In Reactors, after plicatic acid inhalation compared to control day, median values of sputum eosinophils increased from 6.5% to 25.0%, eosinophil cationic protein (ECP) increased from 260 to 456 ng/ml, and eotaxin from 58 to 133 pg/ml (p<0.01), but LTB4 and LTC4 did not increase significantly. Non-reactors did not show any significant changes in any parameter. We conclude that the markers of eosinophil activation, ECP and eotaxin, are better indicators of a positive reaction to specific inhalation challenge in red cedar asthma than leukotrienes. Supported by a WorkSafeBC grant
Dr. Victoria Maxwell, DVM, MBA, Luitpold Pharmaceuticals, Inc. Degenerative joint disease (DJD) = osteoarthritis Why we see DJD in young horses • Rigors of “use trauma” allow the forces of destruction to outweigh normal repair Two long bones together = diarthual joint • Range of motion anterior/posterior aka forward/backward • External support structures – skin, tendon, ligament
management | qof A total of eight points are available to practices for the correct management and treatment of obesity. Dr PAul lAmbDen explainsObesity is rapidly becoming the United Kingdom’s biggest health problem with associated deaths estimated at between 10-30,000 a year from obesity alone. Nearly two-thirds (70 per cent) of men and 63 per cent of women are over-weight or obese and it
 Final Report: WorkSafeBC Project RS2003/04-022
Final Report: WorkSafeBC Project RS2003/04-022
 Final Report: WorkSafeBC Project RS2003/04-022
Final Report: WorkSafeBC Project RS2003/04-022
Figure-2
Final Report: WorkSafeBC Project RS2003/04-022
Final Report: WorkSafeBC Project RS2003/04-022
Figure-2