This article was downloaded by:[Lachmann, Thomas]On: 28 February 2008Access Details: [subscription number 791040317]Publisher: Psychology PressInforma Ltd Registered in England and Wales Registered Number: 1072954Registered office: Mortimer House, 37-41 Mortimer Street, London W1T 3JH, UK
Journal of Clinical and ExperimentalNeuropsychology
Publication details, including instructions for authors and subscription information:Procedural learning eliminates specific slowing down ofresponse selection in patients with idiopathic ParkinsonsyndromeThomas Lachmann ab; Bettina Schumacher ac; Michael Joebges c; HorstHummelsheim c; Cees van Leeuwen b
a University of Kaiserslautern, Kaiserslautern, Germany
b Laboratory for Perceptual Dynamics, Brain Science Institute, RIKEN, Wako-shi,Japan
c University of Leipzig, Leipzig, Germany
To cite this Article: Lachmann, Thomas, Schumacher, Bettina, Joebges, Michael, Hummelsheim, Horst and vanLeeuwen, Cees (2007) 'Procedural learning eliminates specific slowing down of response selection in patients withidiopathic Parkinson syndrome', Journal of Clinical and Experimental Neuropsychology, 30:3, 319 - 326To link to this article: DOI: 10.1080/13803390701399278URL:
This article maybe used for research, teaching and private study purposes. Any substantial or systematic reproduction,re-distribution, re-selling, loan or sub-licensing, systematic supply or distribution in any form to anyone is expresslyforbidden.
The publisher does not give any warranty express or implied or make any representation that the contents will becomplete or accurate or up to date. The accuracy of any instructions, formulae and drug doses should beindependently verified with primary sources. The publisher shall not be liable for any loss, actions, claims, proceedings,demand or costs or damages whatsoever or howsoever caused arising directly or indirectly in connection with orarising out of the use of this material.
JOURNAL OF CLINICAL AND EXPERIMENTAL NEUROPSYCHOLOGY2008, 30 (3), 319–326
Procedural learning eliminates specific slowing down of response selection in patients with idiopathic Parkinson syndrome Thomas Lachmann,1,2 Bettina Schumacher,1,3 Michael Joebges,3 Horst Hummelsheim,3 and Cees van Leeuwen2
1University of Kaiserslautern, Kaiserslautern, Germany2Laboratory for Perceptual Dynamics, Brain Science Institute, RIKEN, Wako-shi, Japan3University of Leipzig, Leipzig, Germany
Patients with idiopathic Parkinson syndrome and normally aged controls participated in a psychological refrac-tory period experiment. Two tasks were presented on each trial: auditory discrimination of high versus low tones,followed by visual classification of letters versus their mirror images. Speeded responses to both tasks wererequired. Stimulus onset asynchrony between the tasks was varied (short vs. long). Both groups showed equalresponse times overall, but patients were slower on the second task in the short stimulus onset asynchrony condi-tion. This effect was eliminated with practice. The results were interpreted in terms of reduced capacity for cogni-tive processes involving decision making as a secondary symptom of the Parkinson syndrome.
Downloaded By: [Lachmann, Thomas] At: 21:04 28 February 2008
The idiopathic Parkinson syndrome (IPS) has an
ever, a number of studies have suggested consider-
incidence rate of 1% of all over-65-year-olds in typ-
ing cognitive deficits as well (see Brown & Marsden,
ical western countries. Proteinaceous inclusion
1987, for an overview). General cognitive slowing
bodies accumulate within neurons, leading to cell
down (bradyphrenia) has been proposed (Naville,
death in specific vulnerable areas. The process
1922; Smith et al., 1998) but such symptoms could
advances in a predictable sequence to other areas.
also be attributed to normal aging (Phillips et al.,
During early stages, synuclein accumulations can
1999), dementia, or late-life depression (Butters
be detected as precursors of the inclusion bodies in
et al., 2004). Others have argued for more specific
the medulla oblongata and olfactory bulb and later
deficits (Sullivan & Sagar, 1989; Brown &
in the substantia nigra. In addition, other nuclear
Marsden, 1987), involving mainly two specific func-
substances of the midbrain and basal forebrain are
tions: visuo-spatial processing (Amick, Cronin-
the focus of initially subtle and subsequently more
Golomb, & Gilmore, 2003; Lee, Harris, & Calvert,
severe changes. At this point the disease reaches its
1998; Natsopoulos, Bostantzopoulou, Katsarou, &
symptomatic phase. Patients show rigor, hypo-
Grouios, 1993; Pirozzolo, Hansch, Mortimer,
kinesia, or tremor. During the end-stages, the
Webster, & Kuskowsky, 1982; Proctor, Riklan,
pathological progression encroaches upon the tel-
Cooper, & Teuber, 1964; Taylor, Saint-Cyr, & Lang,
encephalic cortex, and additional symptoms like
1986) and memory search (Ivory, Knight, Longmore,
postural instability occur (Braak et al., 2002).
& Caradoc-Davies, 1999; Pirozzolo et al., 1982).
Parkinson (1817) originally considered IPS as an
Regarding visuo-spatial processing: McDowell
exclusively motor system disease. Since then, how-
and Harris (1997), using questionnaires, found that
Thanks are due to Max David from the Parkinson self-help group in Leipzig, to Steffen Huebner (Leipzig) and Andreas Widmann
(Leipzig) for technical support, and to Daniel Tranel and anonymous reviewers for their helpful remarks on an earlier draft of thispaper.
Address correspondence to Thomas Lachmann, University of Kaiserslautern, Pfaffenbergstr. 103, 67663 Kaiserslautern, Germany
2007 Psychology Press, an imprint of the Taylor & Francis Group, an Informa business
patients reported problems with depth and motion
cessing task and study the effect of practice. To this
perception but not with color, brightness, and
aim we use the psychological refractory period
shape perception. Lee et al. (1998) showed that IPS
(PRP) paradigm (Szameitat, Lepsien, von Cramon,
patients have impairments in mental rotation
Sterr, & Schubert, 2006; Szameitat, Schubert,
tasks, in which visuo-spatial representations have
to be manipulated internally. Other experimental
The PRP paradigm belongs to the family of
studies, however, failed to find visuo-spatial orien-
dual-task paradigms. Cognitive processing capa-
tation problems in IPS patients (Hsieh, Hwang,
city is limited, so when two tasks that require cent-
ral processes are performed simultaneously,
Regarding memory search, Appollonio et al.
performance is usually worse than when these
(1994) and Breen (1993) found free-recall impair-
tasks are performed independently (Telford, 1931;
ment in IPS, whereas recognition memory was nor-
Welford, 1952). When they are performed in rapid
mal. Brown and Marsden (1987) and Flowers,
succession, performance is degraded most when
Pearce, and Pearce (1984) similarly found specific
the difference between the onset of the first and
deficits in memory retrieval. It was concluded that
second task (stimulus onset asynchrony, SOA) is
although patients were able to adopt adequate pro-
minimal. These results are an effect of the central
cessing strategies, they were less efficient in using
information-processing bottleneck (Pashler, 1984;
these (Breen, 1993). Press, Mechanic, Tarsy, and
Pashler & Johnston, 1998; Welford, 1952), which
Manoach (2002) investigated memory search in
may be identified with the frontal system. Szameitat
IPS patients using a classical Sternberg task
et al. (2002) located PRP-related activity in
(Sternberg, 1966). Multiple items are kept in mem-
various frontal areas (inferior frontal sulcus, mid-
ory, and participants must search for a given item
dle frontal gyrus) and the intraparietal sulcus.
within this memory set. Linear increase in memory
These brain areas were activated in a dual-task
search time as a function of the number of items in
situation but not when the tasks were performed
Downloaded By: [Lachmann, Thomas] At: 21:04 28 February 2008
memory set is understood as memory search rate.
Press et al. (2002) found a slower memory search
In the PRP bottleneck paradigm (Pashler, 1984,
rate in IPS patients than in normal controls.
1994), the SOA is systematically varied with differ-
Wilson, Kasniak, Klawans, and Garron (1980) had
ent levels of a task complexity variable (e.g.,
previously found reduced retrieval rates in IPS
Lachmann & van Leeuwen, 2007; Schwarz &
patients. Posner, Walker, Friedrich, and Rafel
Ischebeck, 2001). Priority is given to the first task.
(1984) failed to find such a difference, but reported
To involve the central bottleneck, this task must
a general increase in reaction time (RT).
require a decision (as in a choice response task),
Visuo-spatial perception and memory retrieval
but should otherwise be kept simple. Binary classi-
studies both involve manipulating information
fication of tones is typically used (Pashler, 1994).
internally in the service of guiding behavior. Such
Central processing of the second task will have to
central processes are typically a function of the
wait until the bottleneck is cleared from the first
frontal network (Taylor et al., 1986), which is lim-
task. As a result RT increases with decreasing
ited in its processing capacity. To alleviate its work-
SOA. The waiting time for clearance, however, will
load, proceduralization (Anderson, 1982) results in
be equal for all these processes, independently of
the formation of automatized behavioral routines
their level of complexity. In a factorial design, this
for efficient task execution. Deficits in procedurali-
means that effects of SOA and central processing
complexity will have additive effects.
for capacity limitations in IPS patients (Haaland,
In contrast, processes prior to the central bottle-
Harrington, O’Brien, & Hermanowicz, 1997;
neck stage of the second task may overlap with the
Pascual-Leone et al., 1993; Sommer, Grafman,
bottleneck stage of the first task, without diminish-
Clark, & Hallett, 1999). Press et al. (2002) found
ing the rate of processing for either task. With
that the reduction in memory search rate in IPS
decreasing SOA, an increasing proportion of pre-
patients disappeared after the first experimental
bottleneck second-task processes will overlap. Thus,
session. The authors suggested that there was a
the complexity of these processes will increasingly
delay in proceduralization of memory search.
be buried in the overlap if the SOA is diminished.
Our aim is to establish whether there is a delay in
As a result, we would observe a subadditive inter-
proceduralization in IPS patients in visuospatial
action of second task complexity with decreasing
processing. We investigate to what extent the
involvement of the frontal system disappears with
Thus, using the PRP paradigm allows us to dis-
practice. To do so we need to show the involve-
tinguish between perceptive, central-cognitive and
ment of the frontal system in our visuo-spatial pro-
motor processes for a given task. If there are RT
differences between IPS patients and controls, the
lack a task complexity variable, with which SOA
PRP effects tell us why, where, and how. By look-
could interact, as in the PRP bottleneck paradigm.
ing at practice effects, we may observe effects of
In addition, they fail to provide us with data on
Previous dual-task studies with IPS patients
have yielded mixed results. Malapani, Pillon,
EXPERIMENT
Dubois, and Agid (1994) found that IPS patientsperformed equal to controls on visual and auditory
go/no-go tasks, but when the two tasks were pre-sented simultaneously the speed of performance in
Participants
the former showed a greater drop than that in thelatter. This indicates that IPS patients find com-
We recruited a total of 28 participants through
plex decision making particularly hard. Other
advertisement in the monthly magazine of a local
studies supported this hypothesis (Brown &
Parkinson self-help group. A total of 16 of them
Marsden, 1991; Dalrymple-Alford, Kalders, Jones,
were in the patients group (experimental group), 10
& Watson, 1994; Fournet et al., 1996; Horstink,
of whom were females. Average age in this group
Berger, van Spaendonck, van den Bercken, &
was 66 years, ranging from 52–75. Patients’ IPS
Cools, 1990; Robertson, Hazlewood, & Rawson,
diagnosis was validated by experienced neurolo-
gists specialized on the area of IPS, according to
In contrast, Hein, Schubert, and von Cramon
brain bank criteria. The Hoehn and Yahr state of
(2005) found no greater drop in performance in
all patients was diagnosed as between 2.0 and 2.5.
IPS patients than in normal controls when two
Duration of illness, medication, and laterality of
tasks were presented close in time. Similarly,
the patients are reported in Table 1. According to
Hsieh (2000) presented two tasks with an SOA of
Press et al. (2002), medication, and its correspond-
Downloaded By: [Lachmann, Thomas] At: 21:04 28 February 2008
50, 150, or 650 ms. The first task was a tone dis-
ing dopaminargic state, has no influence on the
crimination task, the second a digit identification
performance in a typical RT task, such as memory
task (replication of Pashler, 1989). She found
increased RT and error rates for the first task. For
Participants of the control group were 12 family
the second task she found increased RT for IPS,
members of the patients, 8 of whom were females.
but no interaction with SOA. Hsieh concluded
Average age was 67 years, ranging from 52–81.
that extra motor execution time might have pro-
Participants in the control group were selected for
duced the group main effect. The main problem
reporting no history of neurological disorders and
with all these experiments, however, is that they
not receiving any psychopharmacological drugs.
Description of the patients with IPS participating in the experiment
Note. IPS = idiopathic Parkinson syndrome. F = female, M = male. aIn years. bIn mg.
Patients and controls received 10 euros for their
respond to the tone first and that, although both
participation. All participants had normal or cor-
tasks were important, they should focus on
rected-to-normal seeing and hearing abilities. An
responding to the tones. At the beginning of a trial,
interview was held prior to the experiment with
a fixation cross was shown for 300 ms in the center
all participants to assure normal intelligence and
of the screen, followed by a tone. High or low
to exclude ailments such as acute untreated
tones were used with equal frequency in the experi-
depression or other psychiatric or psychological
ment. The visual stimulus was presented with
illnesses that might influence the level of cognitive
either a short (50-ms) or long (400-ms) SOA. Vis-
ual stimuli were shown until the response occurred. All stimuli occurred with equal frequency within
Stimuli
the experiment. Whenever participants failed torespond to the tone within 1,600 ms, the text:
Tones were presented for 33 ms at either 900
“Please respond faster to the tone!” appeared on
(high) or 300 Hz (low) using standard sound card
the screen in addition to the feedback. If the
and speakers. The letters F, R, g, and their mirror
response time in the first 16 trials was above 1,600
images were presented visually. Letters were com-
ms on average, the program was interrupted
posed of straight-line segments drawn on a 5-cm
briefly, and a full-screen text appeared: “Please try
(horizontal) by 7-cm (vertical) grid and were dis-
to be a bit faster! Average response time to the
played on a 14-inch standard PC monitor. The vis-
tone: [e.g., 1,892] ms.” When a response to a tone
ual angel was about 5° horizontally and about 6.5°
was given faster than 200 ms, the sentence: “Please
vertically. There was no fixation of the partici-
do not guess the tone!” appeared. No feedback was
given for correct responses. The next trial started2 s later. Procedure
A total of six blocks of 24 trials was presented, in
Downloaded By: [Lachmann, Thomas] At: 21:04 28 February 2008
Participants were seated at 60-cm distance from
which equal numbers of long and short SOA trials
the monitor in a sound-attenuated and darkened
were randomly intermixed. Halfway through and
room. They were instructed to rest their hands on a
at the end of each block participants were offered
wooden panel, 50 cm long, which contained four
an optional short break. After each block they
response keys, two on the left-hand side and two
received feedback on their within-block average
on the right-hand side, one next to each other. As
response times and percentages correct on both
keys, 7.5 × 7.5-cm standard light push-buttons
were used. The keys on the left side contained thelabels “high” and “low.” The keys on the right side
contained the labels “normal” and “mirrored.”
Participants started with a 25-trials training ses-
Individual mean response times and error rates
sion of the auditory discrimination task, for which
were positively correlated in the first task (R =
they were instructed to respond as fast and accu-
.586, p < .01); in the second task no correlation was
rately as possible depending on whether the tone
presented was “high” or “low,” using the responsekeys on the left-hand side. Subsequently they were
Task 1: Auditory classification
trained for 30 trials on the letter discriminationtask. There, in each trial a fixation cross appeared
The overall mean RT was 946 ms (SD = 504),
for 300 ms prior to the presentation of a letter in
and the mean error rate was 8.6%. Analysis of var-
the center of the screen. Participants were
iance (ANOVA) on RT, with factors group (IPS
instructed to respond as fast as possible whether
vs. control) as between-subjects factor and SOA
the letter presented was “normal” or “mirrored”
(long vs. short) and reflection (normal vs. mirrored
by using the response keys on their right-hand side.
items in the second task) as within-subjects factors,
Speed and accuracy feedback were given during
resulted in a main effect of SOA, F(1, 26) = 51.88,
the training sessions. Following a correct trial, the
p < .001. Performance was weaker with short
response time in ms was briefly presented in green;
(1,018 ms, SD = 550) than with long SOA (877 ms,
following an incorrect response, the time was given
SD = 444), and for reflection, F(1, 26) = 8.725, p <
in red. Feedback on the auditory task was given in
.01, faster for normal (925 ms, SD = 483) than for
the lower left corner of the screen, on the visual
mirrored letters (967 ms, SD = 523). The interac-
task in the lower right corner of the screen.
tion of SOA and reflection reached significance,
After training participants were instructed to
F(1, 26) = 5.10, p < .05; for short SOA, normal let-
perform both tasks together. They were told to
ters yielded 977 ms (SD = 507), mirrored 1,060 ms
(SD = 588), and for long SOA, normal letters
independent process. The other interaction is that
yielded 874 ms (SD = 453) and mirrored 879 ms
of Reflection × SOA, F(1, 26) = 9.29, p < .001. Fig-
(SD = 436). Thus, the interaction is based on the
ure 2 shows that for short SOA, normal letters are
restriction of the effect of reflection to short SOA.
faster (1,719 ms, SD = 722) than mirrored (1,885
For group, (F = 0) no other effect approached sig-
ms, SD = 889) but not for long SOA. The direction
nificance. The same analysis on error rates yielded
of this interaction, too, is opposite to what would
have been expected from an automatic, bottleneck-independent process.
The same analysis on error rates resulted in a
Task 2: Visual classification
main effect of group, F(1, 26) = 5.268, p < .05—
The mean RT for the second task was 1,564 ms
more errors were made in the patients group
(SD = 770 ms), and the mean error rate was 7.6%.
(9.9%) than in the control group (4.5%)—and of
ANOVA on RT, with factors group (patients vs.
SOA, F(1, 26) = 7.808, p < .05—more errors were
controls) as between-subjects factor and SOA and
made for short (8.8%) than for long SOA (6.4%).
reflection as within-subjects factors, resulted in
No interactions reached significance.
main effects for SOA, F(1, 26) = 268.37, p < .001,
The present study involves many trial repeti-
with faster responses for long (1,336 ms, SD = 649)
tions. It is therefore possible to investigate the
than for short SOA (1,801 ms, SD = 813), and for
question of whether practice can remedy the spe-
reflection, F(1, 26) = 11.10, p < .005, with faster
cific deficit in IPS patients. To study this question,
responses for normal (1,522 ms, SD = 718) than
the complete session was divided into four practice
for mirrored letters (1,607 ms, SD = 817). No main
stages (I–IV). An ANOVA with factors group,
effect of group was obtained (F < 1; controls = 1,527
SOA, and practice resulted in main effects of SOA,
ms, SD = 685; patients = 1,595 ms, SD = 833). F(1, 26) = 296.3, p < .001, and practice, F(3, 78) =
Two interactions reached significance. Figure 1
53.30, p < .001. The first result duplicates that of
Downloaded By: [Lachmann, Thomas] At: 21:04 28 February 2008
shows the interaction Group × SOA, F(1, 26) =
the first analysis; the second shows that practice
5.36, p < .05. Patients (1,861 ms, SD = 905) were
leads to improvement in both groups. As before,
slower than controls (1,727 ms, SD = 677) for
there was no group main effect. Significant interac-
short SOA but not for long SOA. The direction of
tions were obtained of Group × SOA, F(1, 26) =
the interaction is opposite to what would have
4.69, p < .001, of SOA × Practice, F(3, 78) = 5.00,
resulted if the difference between the two groups
p < .005, and a triple interaction of Group × SOA
had been based on an automatic, bottleneck-
× Practice, F(3, 78) = 2.99, p < .05. Figure 1. Interaction of group and stimulus onset asynchrony Figure 2. Interaction of reflection and stimulus onset asyn-
(SOA); reaction times (RTs) and 95% confidence interval of
chrony (SOA); reaction times (RTs) and 95% confidence inter-
IPS patients versus controls on the secondary mirror image task
val for normal versus mirrored letters on the secondary task
for short (50-ms) and long (400-ms) SOA between the first and
for short (50-ms) and long (400-ms) SOA between the first and
Post hoc analyses showed that the effect of SOA
times with mirrored than with normal letters), a
remained in all practice stages separately, F(1, 26) =
complexity variation of the second task, on the
68–226, p < .001. An interaction of Group × SOA,
response times of the first task when SOA between
however, was found in Practice Stage I, F(1, 26) =
the two tasks is short. With long SOA between
5.76, p < .05, but not in any of the subsequent
these tasks, such cross-talk does not occur.
stages (see Table 2 for detailed data information).
In the second task, IPS patients made more
The same ANOVA was run on error rates.
errors than did controls, but showed no differences
Main effects were found for SOA, F(1, 26) =
overall in response times. For RT an interaction
8.95, p < .01, and group, F(1, 26) = 5.47, p < .05,
between SOA and reflection was obtained; higher
duplicating former results, and for practice, F(1,
RT for mirrored letters than for normal letters was
26) = 4.07, p < .05, with decreasing error rates
only found in the short SOA condition, whereas
with practice in both groups (see Table 2 for
there were no effects in the long SOA condition.
detailed data information). No interactions were
Had this pattern of interaction been opposite (big-
ger effect for long SOA), this would mean evidencefor automatic processing of reversed letters. The
Discussion
present result, however, suggests that letterreversal involves the central bottleneck, equally in
Patients with IPS and age-matched controls per-
both groups of participants. This result indicates
formed a dual-task experiment using a PRP para-
that, in accordance with Ruthruff, Miller, and
Lachmann (1995), the central bottleneck is
classification, the second task visual classification
involved in visuo-spatial manipulations (such as
of normal versus mirrored letters. For the first
task, no group differences were obtained. Equally
IPS patients and normal controls showed no dif-
in the two groups, both the first and second task
ference in overall performance on the second task,
Downloaded By: [Lachmann, Thomas] At: 21:04 28 February 2008
showed main effects of SOA. This means that a
contrary to the notion of general cognitive slowing
bottleneck has occurred in this experiment. At
present, the debate is still on about whether limited
The IPS patients, however, were showing spe-
capacity resources of the bottleneck are allocated
cific cognitive slowing down when the SOA
in an all-or-none fashion (Pashler, 1984, 1989;
between the first and second task was short. If this
Welford, 1952), or whether capacity sharing
were caused by primary motor symptoms of the
between tasks is allowed (Navon & Miller, 2002;
disease, this would have occurred in both SOA
Tombu & Jolicoeur, 2002). When there are effects
conditions. IPS patients, therefore, may find it par-
of SOA on both tasks this implies, according to the
ticularly difficult to combine overlapping decision
logic of the PRP paradigm, that resource sharing
has taken place between the first and second task.
With practice, the effect of SOA was reduced in
In other words, the limited capacity has not been
both groups. Proceduralization means that both
devoted exclusively to the two tasks in sequence,
tasks can be executed more efficiently together. In
but has been divided over the tasks, resulting in a
accordance with Press et al. (2002), we may ascribe
slowing of both. In accordance with this explana-
the initially weaker performance in IPS patients to
tion, there is an effect of reversal (longer response
lack of proceduralization. Performance of IPS
Reaction times and error rates for different SOA levels in controls and Parkinson patients for different levels of practice
Note. IPS = idiopathic Parkinson syndrome. SOA = stimulus onset asynchrony. Reaction times in ms. Error rates in percentages.
patients approached that of the controls already
in medicated Parkinson’s disease patients: The cent-
after about the first 25% of the trials within a sin-
ral executive seems to work. Journal of Neurology,Neurosurgery and Psychiatry, 60, 313–317.
Haaland, K. Y., Harrington, D. L., O’Brien, S., &
Not only is it difficult to assess cognitive deficits
Hermanowicz, N. (1997). Cognitive motor learn-
in Parkinson patients, it is also possible that they
ing in Parkinson’s disease. Neuropsychology, 11,
reflect secondary symptoms, resulting from a
vicious circle of lack of practice, lack of confid-
Hein, G., Schubert, T., & von Cramon, D. Y. (2005).
ence, and avoidance behavior in performing cer-
Closed head injury and perceptual processing in dual-task situations. Experimental Brain Research, 160,
tain tasks, and depression. The currently observed
deficit may be in fact such a secondary symptom.
Horstink, M. W., Berger, H. J., van Spaendonck, K. P.,
Let this be so; the value of the present study is that
van den Bercken, J. H., & Cools, A. R. (1990).
this deficit can easily be remedied by practice.
Bimanual simultaneous motor performance andimpaired ability to shift attention in Parkinson’s dis-ease. Journal of Neurology, Neurosurgery and Psychi-
Original manuscript received 20 November 2006
Revised manuscript accepted 11 April 2007
Hsieh, S. (2000). The psychological refractory period in
Parkinson’s disease. Perceptual and Motor Skills, 91,893–902.
Hsieh, S., Hwang, W.-J., Tsai, J.-J., & Tsai, C.-Y.
(1996). Visuospatial orienting of attention in Par-
REFERENCES
kinson’s disease. Perceptual and Motor Skills, 82,1307–1315.
Amick, M. M., Cronin-Golomb, A., & Gilmore, G. C.
Ivory, S.-J., Knight, R. G., Longmore, B. E., & Caradoc-
(2003). Visual processing of rapidly presented stimuli
Davies, T. (1999). Verbal memory in non-demented
is normalized in PS, but proximal stimulus strength is
patients with idiopathic Parkinson’s disease.
enhanced. Vision Research, 43, 2827–2835. Neuropsychologia, 37, 817–828.
Downloaded By: [Lachmann, Thomas] At: 21:04 28 February 2008
Anderson, J. R. (1982). Acquisition of cognitive skill.
Lachmann, T., & van Leeuwen, C. (2007). Goodness
Psychological Review, 89, 369–406.
takes effort. Perceptual organization in dual-task
Appollonio, I., Grafman, J., Clark, K., Nichelli, P.,
settings. Psychological Research, 71, 152–169.
Zeffiro, T., & Hallett, M. (1994). Implicit and
Lee, A. C., Harris, J. P., & Calvert, J. E. (1998). Impair-
explicit memory in patients with Parkinson’s disease
ments of mental rotation in Parkinson’s disease. Neu-
with and without dementia. Archives of Neurology,ropsychologia, 36, 109–114.
Malapani, C., Pillon, B., Dubois, B., & Agid, Y. (1994).
Braak, H., Del Tredici, K., Bratzke, H., Hamm-
Impaired simultaneous cognitive task performance in
Clement, J., Sandmann-Keil, D., & Rub, U. (2002).
Parkinson’s disease: A dopamin-related dysfunction.
Staging of the intracerebral inclusion body pathology
associated with idiopathic Parkinson’s disease (pre-
McDowell, S.-A., & Harris, J. P. (1997). Visual problems
clinical and clinical stages). Journal of Neurology,
in Parkinson’s disease: A questionnaire survey. Behavioural Neurology, 10, 77–81.
Breen, E. K. (1993). Recall and recognition memory in
Natsopoulos, D., Bostantzopoulou, M.-S., Katsarou, Z.,
Parkinson’s disease. Cortex, 29, 91–102.
& Grouios, G. (1993). Space deficits in PD
Brown, F. B., & Marsden, C. D. (1987). Neuropsychol-
patients: Quantitative or qualitative differences
ogy and cognitive function in Parkinson’s disease: An
from normal controls. Behavioural Neurology, 6,
overview. In C. D. Marsden, & S. Fahn (Eds.),
Movement disorders II (pp. 99–123). London:
Naville, F. (1922). Les complications et les sequelles de
l’encéphalite épidemique [The complications and
Brown, F. B., & Marsden., C. D. (1991). Dual task per-
effects of the epidemic encephalitis]. Encephale, 17,
formance and processing resources in normal subjects
and patients with Parkinson’s disease. Brain, 114,
Navon, D., & Miller, J. (2002). Queuing or sharing? A
critical evaluation of the single-bottleneck notion.
Butters, M. A., Whyte, E. M., Nebes, R. D., Begley,
Cognitive Psychology, 44, 193–251.
A. E., Dew, M. A., Mulsant, B. H., et al. (2004). The
Parkinson, J. (1817). An essay on the shaking palsy.
nature and determinants of neuropschological func-
tioning in late-life depression. Archives of General
Pascual-Leone, A., Grafman, J., Clark, K., Steward, M.,
Massaquoi, S., Lou, J.-S., et al. (1993). Procedural
Dalrymple-Alford, J. C., Kalders, A. S., Jones, R. D., &
learning in Parkinson’s disease and cerebellar degen-
Watson, R. W. (1994). A central executive deficit in
eration. Annals of Neurology, 34, 594–602.
patients with Parkinson’s disease. Journal of Neurology,
Pashler, H. (1984). Processing stages in overlapping
Neurosurgery, and Psychiatry, 57, 360–367.
tasks: Evidence for a central bottleneck. Journal of
Flowers, K. A., Pearce, I., & Pearce, J. M. S. (1984). Experimental Psychology: Human Perception & Per-
Recognition memory in Parkinson’s disease. Journalof Neurology, Neurosurgery and Psychiatry, 47,
Pashler, H. (1989). Dissociations and dependencies
between speed and accuracy: Evidence for a two-
Fournet, N., Moreaud, O., Roulin, J. L., Naegele, B.,
component theory of divided attention in simple
Pollak, P., & Pellat, J. (1996). The phonological loop
tasks. Cognitive Psychology, 21, 469–514.
Pashler, H. E. (1994). Dual-task interference in simple
nonmedicated Parkinson’s disease. Journal of
tasks: Data and theory. Psychological Bulletin, 116,
the International Neuropsychological Society, 4,
Pashler, H., & Johnston, J. C. (1989). Chronometric
Sommer, M., Grafman, J., Clark, K., & Hallett, M.
evidence for central postponement in temporally
(1999). Learning in Parkinson’s disease: Eyeblink
overlapping tasks. Quarterly Journal of Experimental
conditioning, declarative learning, and procedural
learning. Journal of Neurology, Neurosurgery and
Phillips, J. G., Schiffter, T., Nicholls, M. E. R.,
Bradshaw, J. L., Iansek, R., & Saling, L. L. (1999).
Sternberg, S. (1966). High-speed scanning in human
Does old age or Parkinson’s disease cause bradyphre-
memory. Science, 153, 652–654.
nia. Journals of Gerontology: Biological Sciences and
Sullivan, E. V., & Sagar, H. J. (1989). Nonverbal recog-
Medical Sciences, 54, 404–409.
nition and recency discrimination deficits in Parkin-
Pirozzolo, F. H., Hansch, E. C., Mortimer, J. A.,
son’s disease and Alzheimer’s disease. Brain, 112,
Webster, D. D., & Kuskowsky, M. A. (1982).
Dementia in Parkinsons’s disease: A neuropsycholog-
Szameitat, A. J., Lepsien, A. J., von Cramon, D. Y.,
ical analysis. Brain and Cognition, 1, 71–83.
Sterr, A., & Schubert, T. (2006). Task-order
Posner, M. I., Walker, F. J. F., Friedrich, F. A., &
coordination in dual-task performance and the lateral
Rafel, R. D. (1984). Effects of pariental injury on
pre-frontal cortex: An event-related fMRI study. Psy-
covert orienting of attention. Journal of Neuro-chological Research, 70, 541–552.
Szameitat, A. J., Schubert, T., Müller, K., & von
Press, D. Z., Mechanic, D. J., Tarsy, D., & Manoach, D.
Cramon, D. Y. (2002). Localization of executive
S. (2002). Cognitive slowing in Parkinson’s disease
functions in dual-task performance with fMRI. Jour-
resolves after practice. Journal of Neurology, Neuro-nal of Cognitive Neuroscience, 14, 1184–1199. surgery and Psychiatry, 73, 524–528.
Taylor, A. E., Saint-Cyr, J. A., & Lang, A. E. (1986).
Proctor, F., Riklan, M., Cooper, I. S., & Teuber, H.-L.
Frontal lobe dysfunction in Parkinson’s disease. The
(1964). Judgment of visual and postural vertical by
cortical focus of neostriatal outflow. Brain, 109,
Parkinsonian patients. Neurology, 14, 287–292.
Robertson, C., Hazlewood, R., & Rawson, M. D.
Telford, C. W. (1931). The refractory phase of voluntary
Downloaded By: [Lachmann, Thomas] At: 21:04 28 February 2008
(1996). The effects of Parkinson’s disease on the
and associative responses. Journal of Experimental
capacity to generate information randomly. Neu-ropsychologia, 34, 1069–1078.
Tombu, M., & Jolicoer, P. (2002). All-or-none bottle-
Ruthruff, E., Miller, J., & Lachmann, T. (1995). Does
neck versus capacity sharing accounts for the psycho-
mental rotation require central mechanisms? Journal
logical refractory period phenomenon. Psychologicalof Experimental Psychology: Human Perception and
Welford, A. T. (1952). The “psychological refractory
Schwarz, W., & Ischebeck, A. (2001). On the interpreta-
period” and the timing of high-speed performance—a
tion of RT vs. SOA functions: Application to dual
review and a theory. British Journal of Psychology,
task and precue-utilization paradigms. Journal ofMathematical Psychology, 45, 452–479.
Wilson, R. S., Kasniak, A. W., Klawans, H. L., & Gar-
Smith, M. C., Goldman, W. P., Janer, K. W., Baty, W.,
ron, D. C. (1980). High speed memory scanning in
Jack, D., & Morris, J. C. (1998). Cognitive speed in
parkinsonism. Cortex, 16, 67–72.
opmærksom på: Behandling af ADHD og andre kroniske tilstande skal altid varetages af en professionel behandler. Kroniske og alvorlige tilstande egner sig aldrig til selv-behandling. Vær kritisk i valget af behandler og vælg en, der er veluddannet, og som du har tillid til. En klassisk homøopatisk behandling er baseret på velfun-derede behandlingsprincipper, og det er dem, der henvis
Copyright 2003. American Cavy Breeders Association. All rights reserved ANTIBIOTICS What I Use I will discuss the commonly used antibiotics forkidneys and can potentially cause fatal antibiotic-cavies and describe several medical situations where Iinduced diarrhea in cavies. I personally use Amikacinwould, or have, used them. I must point out that eachbecause its side effects are report
 This article was downloaded by:[Lachmann, Thomas]On: 28 February 2008Access Details: [subscription number 791040317]Publisher: Psychology PressInforma Ltd Registered in England and Wales Registered Number: 1072954Registered office: Mortimer House, 37-41 Mortimer Street, London W1T 3JH, UK
Journal of Clinical and ExperimentalNeuropsychology
Publication details, including instructions for authors and subscription information:Procedural learning eliminates specific slowing down ofresponse selection in patients with idiopathic ParkinsonsyndromeThomas Lachmann ab; Bettina Schumacher ac; Michael Joebges c; HorstHummelsheim c; Cees van Leeuwen b
a University of Kaiserslautern, Kaiserslautern, Germany
b Laboratory for Perceptual Dynamics, Brain Science Institute, RIKEN, Wako-shi,Japan
c University of Leipzig, Leipzig, Germany
To cite this Article: Lachmann, Thomas, Schumacher, Bettina, Joebges, Michael, Hummelsheim, Horst and vanLeeuwen, Cees (2007) 'Procedural learning eliminates specific slowing down of response selection in patients withidiopathic Parkinson syndrome', Journal of Clinical and Experimental Neuropsychology, 30:3, 319 - 326To link to this article: DOI: 10.1080/13803390701399278URL:
This article maybe used for research, teaching and private study purposes. Any substantial or systematic reproduction,re-distribution, re-selling, loan or sub-licensing, systematic supply or distribution in any form to anyone is expresslyforbidden.
This article was downloaded by:[Lachmann, Thomas]On: 28 February 2008Access Details: [subscription number 791040317]Publisher: Psychology PressInforma Ltd Registered in England and Wales Registered Number: 1072954Registered office: Mortimer House, 37-41 Mortimer Street, London W1T 3JH, UK
Journal of Clinical and ExperimentalNeuropsychology
Publication details, including instructions for authors and subscription information:Procedural learning eliminates specific slowing down ofresponse selection in patients with idiopathic ParkinsonsyndromeThomas Lachmann ab; Bettina Schumacher ac; Michael Joebges c; HorstHummelsheim c; Cees van Leeuwen b
a University of Kaiserslautern, Kaiserslautern, Germany
b Laboratory for Perceptual Dynamics, Brain Science Institute, RIKEN, Wako-shi,Japan
c University of Leipzig, Leipzig, Germany
To cite this Article: Lachmann, Thomas, Schumacher, Bettina, Joebges, Michael, Hummelsheim, Horst and vanLeeuwen, Cees (2007) 'Procedural learning eliminates specific slowing down of response selection in patients withidiopathic Parkinson syndrome', Journal of Clinical and Experimental Neuropsychology, 30:3, 319 - 326To link to this article: DOI: 10.1080/13803390701399278URL:
This article maybe used for research, teaching and private study purposes. Any substantial or systematic reproduction,re-distribution, re-selling, loan or sub-licensing, systematic supply or distribution in any form to anyone is expresslyforbidden.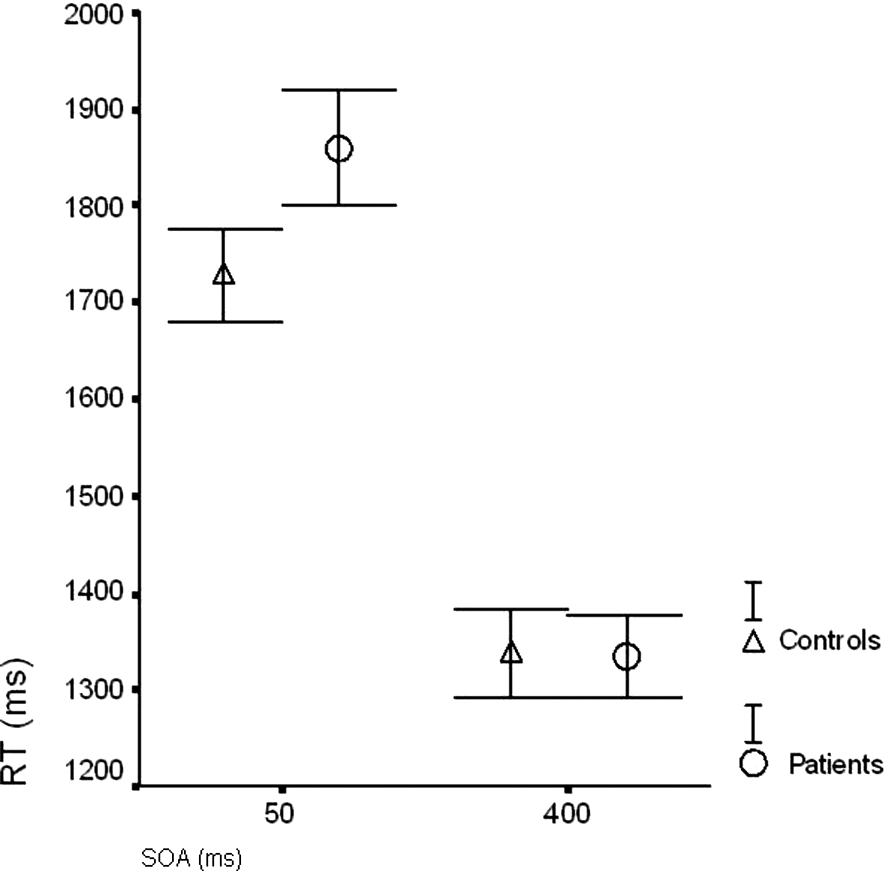 (SD = 588), and for long SOA, normal letters
independent process. The other interaction is that
yielded 874 ms (SD = 453) and mirrored 879 ms
of Reflection × SOA, F(1, 26) = 9.29, p < .001. Fig-
(SD = 436). Thus, the interaction is based on the
ure 2 shows that for short SOA, normal letters are
restriction of the effect of reflection to short SOA.
(SD = 588), and for long SOA, normal letters
independent process. The other interaction is that
yielded 874 ms (SD = 453) and mirrored 879 ms
of Reflection × SOA, F(1, 26) = 9.29, p < .001. Fig-
(SD = 436). Thus, the interaction is based on the
ure 2 shows that for short SOA, normal letters are
restriction of the effect of reflection to short SOA.