Seminars in Neonatology (2003) 8, 223–232 Surgical treatment of infants with necrotizing enterocolitis Agostino Pierro*, Nigel Hall Department of Paediatric Surgery, The Institute of Child Health and Great Ormond Street Hospital forChildren NHS Trust, University College London, London, UKSummary With the improvements in neonatal intensive care, necrotizing enterocolitis KEYWORDS ;
(NEC) has become the most common gastrointestinal emergency amongst infants in
neonatal intensive care units. The incidence of NEC varies between 1 and 8% of
neonatal intensive care unit admissions and the disease has a mortality rate between
20 and 40%. There are a number of surgical options available to the paediatric surgeon
depending on the clinical condition of the infant and the extent of the disease.
However owing to a paucity of prospective data in this field and a lack of randomizedcontrolled trials there is little consensus as to which is the most appropriate. Primaryperitoneal drainage has become very popular in North America and Europe for thetreatment of perforated NEC in very low-birthweight infants. It is a useful manoeuvrein the resuscitation of critically ill infants and in some of these infants, furtheroperation may be avoided completely by inserting a peritoneal drain. Others howeverremain too unwell to undergo laparotomy and may die. Two randomized controlledtrials are currently underway to determine the real benefit of peritoneal drainage. Laparotomy in very small neonates has become safer with improvements in anaesthe-sia and intensive care management. Resection and primary anastomosis has beenproposed as a valid treatment modality in neonates with both focal and multifocaldisease. The advantage of resection and primary anastomosis over stoma formation isstill controversial. Different surgical techniques such as diverting jejunostomy or ‘clipand drop’ have been described to deal with extensive disease and avoid massive smallbowel resection. Prospective studies and randomized controlled trials are needed todefine the best operative treatment for neonates with severe NEC. 2003 Published by Elsevier Ltd. Introduction
nized risk factors such as congenital heart disease. The majority of cases respond to intensive medical
Necrotizing enterocolitis (NEC) is the most common
treatment, which involves treatment of sepsis with
surgical emergency in the neonatal period. With
parenteral broad-spectrum antibiotics, correction
advances in neonatal intensive care, the incidence
of hypovolaemia and acidosis, ventilatory sup-
is increasing and the disease affects up to 0.5% of
port of respiratory failure and other supportive
all live births and 3–5% of low-birthweight live
measures. The intestine is decompressed by means
births. Whilst primarily a disease of pre-term
of a nasogastric tube and rested for a period of at
infants, it is also observed in term infants, particu-
least 7–10 days during which time nutritional intake
larly those with co-existing morbidities and recog-
is maintained by means of total parenteral nutrition(TPN). Despite excellent medical attention, a
* Corresponding author: Department of Paediatric Surgery,
number of infants develop more severe NEC requir-
ing surgical intervention. This group of infants rep-
WC1N 1EH, UK. Tel.: +44-20-7905-2175/2641; fax: +44-20-
resents a major challenge for paediatric surgeons.
7404-6181E-mail address: [email protected] (A. Pierro).
Despite increasing experience of this disease, there
1084-2756/03/$ - see front matter 2003 Published by Elsevier Ltd. doi:10.1016/S1084-2756(03)00025-3
remains little consensus as to the most appropriate
Indications for surgery in infants with NEC
timing and nature of surgery. In addition to surgeryin the acute phase, a number of infants develop
late complications of NEC, either following medi-
PneumoperitoneumClinical deterioration despite maximal medical treatment
cal or previous surgical treatment, and these
Abdominal mass with persistent intestinal obstruction or
complications require surgical intervention. Paucity of evidence
Increased abdominal tenderness, distension and/or
Whilst there are a number of surgical techniques in
use for the management of NEC, there is little
agreement amongst paediatric surgeons as to the
approach most beneficial to the child. This stems
primarily from the lack of quality prospective dataor randomized controlled trials concerning this con-dition. Although the disease is not rare, the share ofcases seen in each individual centre is sufficientlysmall to preclude large-scale studies on a local
perforation associated with persistent signs of
basis. The majority of published data comparing
treatment modalities are retrospective reviews of
Various authors have suggested other indications
relatively small series of patients. There is inevi-
for surgery, some of which remain controversial.
table bias within these studies and the numbers
Occasionally, a laparotomy is performed because of
involved are too small to draw reliable conclusions.
increased abdominal tenderness and distension
In order for one surgical method to be proven
and/or discolouration of the abdominal wall. The
superior to another, large-scale, multicentre,
differential diagnosis in these cases include midgut
prospective, randomized controlled trials are
volvulus, Hirschsprung's enterocolitis and, rarely,
required. To date, these have been particularly
intussusception.6 Similarly, a fixed dilated intesti-
sparse in the field of paediatric surgery. This article
nal loop defined by persistent location and con-
focuses on the operative management of infants
figuration for more than 24 h has been a proposed
with severe NEC and on the recent advances in this
indication for surgery. However, approximately
half of the patients with this finding recover with-out undergoing an operation.5,7 The presence of gas
Indications for surgery
in the portal vein on abdominal radiograph has beenproposed as an indication for surgery, although this
Severity of NEC is classified according to the Bell
is not accepted universally it does appear to carry a
criteria which have been modified by Walsh and
relatively poor prognosis.8 Rowe et al.5,9 suggested
Kliegman.1 Whilst this system may aid some thera-
that more than 90% of infants with portal vein gas
peutic decisions and provide limited prognostic
will develop intestinal necrosis, and approximately
information, it does not take into account the
half will have panintestinal involvement. These
extent of disease on an anatomical basis which
authors suggest operative intervention on appear-
ance of portal vein gas on plain abdominal radio-
There is great controversy surrounding the indi-
graphs. Finally, according to Kosloske et al.,3 a
cations for surgery in infants with NEC. Table 1
positive paracentesis (defined as aspiration of more
summarizes the indications reported in the litera-
than 0.5 ml of brown or yellow-brown fluid with
ture. The indications for operation in a recent study
visible bacteria on Gram stain) is suggestive of
of neonates with NEC included pneumoperitoneum
gangrenous bowel thereby indicating surgical inter-
in 45% of the neonates, clinical deterioration in 37%
and intestinal obstruction in 18%.2 The most widely
have been reported on the presence of sealed
accepted indication for surgery is the presence of
pneumoperitoneum. Unfortunately, pneumoperi-
toneum is not always demonstrable in neonates
infants with severe NEC11 and its prevalence is
with intestinal perforations.3–5 Other absolute
indications for surgery in acute NEC include con-
arotomy.12 The value of thrombocytopenia in
tinued deterioration of an infant that is refrac-
defining the extent of the disease and the need for
tory to maximal medical treatment, and an
an operation is controversial. The trend of the
abdominal mass or abscess secondary to intestinal
platelet count during the course of the disease is
Surgical treatment of infants with necrotizing enterocolitis
considered particularly important. A sudden, pro-
found drop in the platelet count appears to predictthe presence of gangrenous bowel13 and may indi-
cate the need for operative intervention.14 Platelet
consumption in combination with one or more other
factors, such as abdominal mass or radiographic
evidence of fixed abnormal bowel loops, is con-
Proximal jejunostomy‘Clip and drop’ technique
sidered an important criterion to determine the
need for surgery.15 Persistent thrombocytopenia16or decreasing platelet count17 is considered import-ant in diagnosing clinical deterioration and theneed for surgery. A study of risk factors and severityindices in NEC showed that infants that were
number of options exist, including resection with
operated had significantly lower platelet counts
enterostomy, resection with primary anastomosis,
pre-operatively than the ones managed conserva-
proximal jejunostomy, ‘clip and drop’ technique
tively.18 Ververidis et al.2 showed that the greater
the extent of the disease, the lower the platelet
The patient's weight and clinical status as well as
count. The nadir platelet count was significantly
the extent of the disease influence the choice of
lower in infants who died than in survivors. None of
surgical intervention. At laparotomy, the extent of
the patients with platelet count >100×109/l died. In
the disease can be classified as focal when it is
predicting intestinal gangrene, severe thrombo-
limited to a single intestinal segment; multifocal if
cytopaenia has a sensitivity of 69%, specificity of
it includes two or more intestinal segments with
60% and positive predictive value of 89%, whilst a
more than 50% of the small intestine viable and
rapid fall in platelet count has a sensitivity of 32%,
panintestinal when the majority of small and large
specificity of 89% and positive predictive value of
bowels are involved with less than 25% viable bowel
92%. Therefore, the presence of thrombocyto-
paenia cannot reasonably predict the extent of thedisease or indicate the need for laparotomy; how-
Primary peritoneal drainage
ever, a very low platelet count or a rapid fall in
The management of intestinal perforation related
platelet count is a negative prognostic sign.
to NEC in extremely low-birthweight infants(ELBW), defined as <1000 g, remains controversial. Surgical treatment
In 1975, Marshall and Ein presented at the meetingof the Canadian Association of Paediatric Surgeons,
Up to 50% of neonates with NEC develop advanced
Winnipeg, Manitoba, Canada, the use of percu-
disease that requires operative treatment.19 Butter
taneous peritoneal drainage before laparotomy, as
et al.20 reported an increase in operative rate from
a method of stabilizing and improving the systemic
46% between 1990 and 1994 to 69% between 1995
status of premature infants with intestinal perfora-
and 1999. According to this study, the increase was
tion secondary to NEC. Initially, it was hoped that
due to an increase in the percentage of stage III
the drainage of air and stools from a child too
patients and an increase in referrals of post-NEC
unstable for a laparotomy would relieve symptoms
strictures. To some it may be surprising that small,
of abdominal compartment syndrome and infec-
unstable, critically ill infants are able to tolerate
tion, and subsequently improve tolerance of a
major surgical interventions. In a recent study
laparotomy. Two years later, Ein et al.24 from the
investigating safety of the operative procedure
Hospital for Sick Children in Toronto reported the
itself, investigators found that even very low-
use of peritoneal drainage without laparotomy
(PPD) in the management of newborn infants with
complicated NEC. Since then, there have been
There is no general consensus concerning the
several reports, which have suggested that PPD may
ideal surgical management of NEC. Current surgical
serve as a definitive therapy rather than an
options include primary peritoneal drainage (PPD)
intermediary for laparotomy. In 1990, the same
authors25 presented their 13-year experience with
The principal surgical objectives of laparotomy
PPD in 37 patients with bowel perforation second-
in acute NEC are to control sepsis, remove gan-
ary to NEC. Sixty-five percent of these patients
grenous bowel and to preserve as much bowel
weighed less than 1000 g and 88% less than 1500 g.
length as possible.5,22,23 Within these objectives, a
These patients were all septic, acidotic and too
unstable to undergo a primary laparotomy. Of the
same treatment modality (PPD/laparotomy). The
37 reported patients, one-third completely recov-
authors concluded that, using the current available
ered with PPD and did not require any further
data, it is not possible to determine whether PPD is
operative intervention. In the remaining two-thirds
associated with improved survival, and that only a
(26 patients), nine (24%) died rapidly before
randomized controlled trial could identify the best
laparotomy (within 24 h) for continued clinical
In light of relatively poor quality evidence from
deterioration, and seven (22%) underwent a
retrospectively collected data, it is not surprising
delayed laparotomy for bowel occlusion or fistula
that there is little consensus amongst paediatric
formation. The authors concluded that laparotomy
surgeons. In an attempt to resolve this issue, there
with resection and bowel anastomosis or stoma
are currently two multicentre, prospective, ran-
could be the preferred treatment for NEC and per-
domized controlled trials in progress comparing
foration, but they recommended PPD for ELBW
peritoneal drainage with primary laparotomy in
infants less than 1000 g (Pierro: NET trial) or 1500 g
In 1988, Cheu et al.26 reported their experience
with PPD in 51 of 92 infants with perforated NEC.
Two recent studies seem to indicate that PPD is
They concluded that PPD was useful in resuscitating
more advantageous in neonates with isolated per-
ELBW infants with intestinal perforation secondary
forations of the gastrointestinal tract not related to
to NEC, but considered PPD a stabilizing procedure
NEC.34,35 These perforations are usually isolated,
and not an alternative to laparotomy. Other
idiopathic or related to indomethacin treatment for
authors have advocated the use of PPD as primary
patent ductus arteriosus. The infants affected have
treatment for NEC and perforation for all children
neither pneumatosis intestinalis nor portal vein
weighing less than 1500 g and for unstable babies
more than 1500 g.27 In this study, 79% of patientssurvived after PPD and 17 out of 23 survivorsrequired no further operative intervention. In ad-
Resection of affected bowel and
dition, the Toronto group28 reported a survival rate
enterostomy formation
of 69% in neonates less than 1000 g treated withperitoneal drainage compared with a survival rate
The resection of affected bowel and exteriorization
of only 22% in neonates who underwent laparotomy
of remaining segments was once thought to be the
only safe surgical approach to the infant with gan-
We recently conducted a systematic review of
grenous bowel. This technique remains widely used
the topic and failed to discover any randomized
but has been superseded by more novel approaches
trial on the usage of PPD in the management of
in some centres. Resection of necrotic bowel in
NEC. In spite of the lack of conclusive evidence,
neonates with NEC has the theoretical advantage of
peritoneal drainage has become a popular method
reducing bacterial translocation and correcting the
of treatment of ELBW infants with complicated
septic state of the patients. The conventional view
NEC, whilst other surgeons still prefer to perform a
is that it is safer to exteriorize the bowel ends as
laparotomy, resection of the diseased bowel, with
the presence of peritonitis, inflammation of the
either a primary anastomosis or stoma creation and
bowel wall and the reduced intestinal blood supply
peritoneal toilet for this disease.29–32 Resection of
in patients with NEC are unfavourable factors for
the necrotic bowel is considered by some authors to
the healing of the anastomosis.36 In addition, the
be the key factor in improving the condition of the
stoma allows adequate healing and rests the distal
neonate.32 Moss et al.33 recently performed a
bowel prior to subsequent re-anastomosis.23
meta-analysis on this topic reviewing the results of
There are, however, several disadvantages to
10 published studies. The combined probability of
this approach. It is often difficult to re-establish
survival was similar for PPD (55%) and laparotomy
adequate enteral feeding sufficient for adequate
(67%). A marked bias in treatment assignment was
weight gain. High output stomas, in particular,
found, with a greater proportion of smaller babies
carry a risk of dehydration and electrolyte imbal-
undergoing PPD compared with laparotomy (931 vs.
ance, and the importance of early closure to avoid
chronic salt and water loss has been highlighted.
of birthweight on survival did not show a signifi-
Enterostomies have been associated with signifi-
cant difference in survival between PPD and
cant morbidity whilst present, including stenosis,
laparotomy. In addition, there were significant
prolapse and excoriation of the surrounding skin.
variations in outcomes between institutions for the
Stoma closure involves a second anaesthesia and is
Surgical treatment of infants with necrotizing enterocolitis
usually performed once the infant is thriving and
et al.23 found that resection and primary anastomo-
fully recovered from the acute stage of the illness.
sis was associated with a higher survival rate than
Metabolic or physical problems, however, may de-
enterostomy. In addition, resection and primary
mand earlier surgery. In one series, the incidence
anastomosis was not associated with higher inci-
of complications in infants with enterostomies for
dence of intestinal strictures and longer duration of
NEC was 68%.37 This high rate has prompted the
PN compared with resection and enterostomy.
search for alternative strategies which may avoid
the need for repetitive surgery and complications
associated with stomas, whilst ensuring that the
domized controlled trials. It is possible that the
underlying surgical principles of treating NEC by
more critical patients with multifocal disease were
allocated to enterostomy in preference over resec-tion with anastomosis, as indicated by the rela-tively high incidence of post-NEC strictures after
Resection and primary anastomosis
enterostomy. It is notable, however, that in thestudy by Fasoli et al.,23 resection and primary
Resection and primary anastomosis was once con-sidered a hazardous option because of the risk of
anastomosis was associated with acceptable mor-
anastomotic leakage due to poor healing of intra-
bidity and mortality even in patients with NEC
peritoneal anastomoses in the presence of peri-
spread to multiple intestinal segments. The results
tonitis, inflammation of the bowel wall and com-
of intestinal resections and multiple primary anas-
promised intestinal blood supply. In recent years, a
tomoses for preservation of bowel length have not
number of centres have published retrospective
been reported in the literature. Hall and Pierro
reviews of infants treated with intestinal resection
(unpublished data) have treated seven neonates
and primary anastomosis. Kieswetter et al.38
(weight 800–1800 g) with resection and multiple
showed that in patients with localized NEC, an 89%
intestinal anastomoses: four neonates, who had
survival rate can be achieved with resection and
two intestinal anastomoses, had no complications,
primary anastomosis. Harberg et al.39 reported
two, who had three and four intestinal anastomo-
minimal morbidity and low mortality (11%) with
ses, had anastomotic leaks and one neonate who
resection and primary anastomosis in patients with
had three anastomoses developed an anastomotic
localized or multiple areas of the disease regardless
stricture. The results of this small series are
of the degree of peritoneal contamination. Sparnon
encouraging, however, more than two intestinal
and Kiely32 reported an uncomplicated and rapid
anastomoses may carry an increased risk of
recovery in seven of 10 neonates with primary
anastomosis. Griffiths et al.40 reported 76% survival
Most paediatric surgeons would agree that every
after resection and primary anastomosis com-
effort should be made to preserve the ileocaecal
pared with 39% in patients who underwent resec-
valve in neonates with NEC. Ladd et al.,47 in a
tion and enterostomy. A similar favourable experi-
retrospective review of infants with NEC, found
ence with resection and primary anastomosis has
no difference in duration of TPN, post-operative
been reported by Pokorny et al.15 and Parigi
stay and growth between infants with or without a
et al.41. In contrast, Cooper et al.42 showed that the
ileocaecal valve. Similarly, in a more recent study,
survival rate of neonates that underwent primary
there were no significant differences in duration
anastomosis was lower (64%) than that of neonates
of TPN, incidence of NEC recurrence and hospital
that had an enterostomy (79%). Ade-Ajayi et al.43
stay between 40 neonates with NEC who had the
reported 89% survival after resection and primary
ileocaecal valve resected and 43 who did not.23
anastomosis for advanced NEC. Recurrence of
However, the incidence of post-NEC strictures was
NEC and strictures occurred in 22 and 17% of the
significantly lower in neonates who had the valve
neonates, respectively. Fasoli et al.23 reported that
resected compared with neonates who retained
in neonates with localized NEC, resection and pri-
the ileocaecal valve, possibly indicating that not
mary anastomosis had similar results to resection
resecting bowel of questionable viability in order to
spare the ileocaecal valve could be less advan-
Whilst resection and primary anastomosis was
tageous than resecting the valve itself. Survival
initially described in selected patients with focal
rate was not affected by the removal of the valve.
disease and good general condition, it is also now
These results seem to indicate that neonates adapt
gaining acceptance as a valid treatment option for
well to the loss of the ileocaecal valve. The critical
severe NEC and even for multifocal disease.22 In a
issues in performing an intestinal resection are
study of 46 neonates with multifocal disease, Fasoli
the length of the retained small bowel and the
gestational age of the neonate. It is well known that
Clip and drop technique
pre-term neonates have potential for bowelgrowth48 and the earlier findings23,47 appear to
This method complies with surgical principles and
indicate that their bowel adaptive capacity to the
also avoids stoma formation. For the infant with
loss of the ileocaecal valve is remarkable.
extensive bowel necrosis, Vaughan et al.50 advo-cated the resection of all segments of grossly non-viable
Operations for panintestinal disease
aspiration of peritoneal contamination, clippingthe ends of remaining bowel and returning them to
The techniques described thus far are of particular
the abdomen. This is followed by a second-look
use for the infant with one or more short segments
laparotomy with delayed anastomosis 48–72 h
of NEC. Multiple resections and primary anasto-
later. In their small series, all three infants with
moses may be appropriate for some infants with
NEC survived,50 and in a subsequent report of four
more widespread disease, provided careful atten-
infants in whom this technique was employed, one
tion is paid to the viability of resection margins.
died and the remaining three required stoma
Infants with NEC affecting a large proportion of the
formation at the second look.8 This technique has
gastrointestinal tract pose a particularly difficult
the advantages of preserving bowel length and
problem, and treatment of this group remains par-
ticularly controversial. The surgical principles inthese children are difficult if not impossible to
Patch, drain and wait
fulfil. Due to the length of bowel involved, it isoften not possible to fully remove all gangrenous
The basic principle of this technique, reported by
intestine whilst salvaging adequate length for sus-
Moore,51 is to resect no bowel and do no entero-
tainable life. It is for these reasons that in the
infant with panintestinal NEC who is unstable and
laparotomy, insertion of bilateral Penrose drains
critically ill, some surgeons would forego further
from the undersurface of the diaphragm into the
treatment. However, when there is doubt, a
pelvis with exit sites in both lower quadrants. Wait-
number of techniques have recently been reported
ing is important and post-drainage laparotomy
with the aim of allowing time for stabilization of
should not be performed before 14 days. The
the infants' general condition and the possibility of
bilateral Penrose drains capture faecal fistulas
some healing of the gastrointestinal tract to occur.
and function as de-facto enterostomies. Moore's
Due to the severity of the disease, the mortality
15-year personal experience indicates no mortality
with this approach during the first 60 post-operative days, no major morbidity and no second
Proximal jejunostomy
operations required in 70% of patients, possibly dueto spontaneous ‘auto-anastomosis’. The author51
Initially proposed by Martin and Neblett,30 surgical
advocates this technique for infants with extensive
creation of a high jejunostomy in the presence of
gut necrosis (NEC totalis). There are no reports
panintestinal disease has been reported in one
from other centres employing the same technique.
series of 10 infants.49 This technique allowsdecompression and defunctioning of the diseased
Authors' preferred surgical strategy
intestine but does not remove gangrenous segmentsand may permit continued bacterial translocation.
The authors' preferred approach to the operative
A second-look laparotomy and intestinal recon-
management of infants with NEC is illustrated in
structive surgery are performed after 6–8 weeks
and the aim is once again to preserve as much
In infants with focal disease involving a small
bowel length as possible. In this series, eight infants
length of small or large bowel, a resection and
survived to undergo a second procedure; in these,
primary anastomosis is usually performed, with the
resection of necrotic segments and anastomosis
exception of patients unstable during the operation
was performed to restore intestinal continuity.
who are managed with a stoma at the level of the
There was, however, a significant incidence of TPN-
related complications and only a 50% long-term
In infants with multifocal disease (>50% of the
TPN-free survival rate. This procedure is useful in
bowel assumed to be viable), various surgical
neonates with NEC affecting the majority of the
options are available. Resection and one or more
intestine, but the high morbidity and mortality rate
intestinal anastomoses (preferably not more than
two) are performed when it is possible to ascertain
Surgical treatment of infants with necrotizing enterocolitis
Authors preferred operative management of advanced NEC.
the viability of the bowel distal to NEC without
orogastric tube is inserted to decompress the
causing significant bleeding. Stoma (with or with-
out intestinal resection), proximal enterostomy or
anaerobic coverage are given intravenously for at
clip and drop technique are performed when: (a) it
least 7 days. Ventilatory and circulatory support are
is not possible to ascertain the status of the bowel
distal to the NEC; (b) the distal bowel is of dubious
Advances in neonatal intensive care have been sub-
viability; (c) attempts to dissect the distal bowel
stantial in recent years, and this article is not
cause significant bleeding and (d) the patient is
unstable peri-operatively. In these circumstances,
The metabolic insult of the necrotic bowel and
a stoma with or without intestinal resection(s) is
sepsis contributes to stress the neonate's homeo-
the preferred surgical option. However, if this
static mechanisms. Sepsis is an intriguing pathologi-
would lead to massive intestinal resection, the clip
cal condition associated with many complex
and drop technique described earlier will be
metabolic and physiological alterations.52 Studies
adopted in an attempt to salvage as much intestinal
in adults have shown that the metabolic response to
length as possible. If the mobilization of the bowel
sepsis is characterized by hypermetabolism as
loops affected by NEC causes significant bleeding, a
documented by an increase in resting energy
high diverting jejunostomy is preferred.
expenditure by up to 49%.53 In addition, increased
In patients with panintestinal disease (>75% of
tissue catabolism,53 gluconeogenesis and hepatic
small and large bowel involved), two options are
release of glucose54 have been described. The
considered: (a) proximal diverting jejunostomy
existing knowledge on the metabolic response to
when the intestinal resection would cause signifi-
sepsis in infants is limited. A recent metabolic study
cant bleeding or loss of the majority of the small
in septic neonates with NEC by Powis et al.55 failed
bowel and (b) clip and drop technique in the at-
to show any increase in whole body protein turn-
tempt to salvage some of the affected bowel and
over, synthesis and catabolism. This data suggests
avoid a short bowel syndrome. In neonates with
that the calorific requirement of infants with NEC is
total intestinal gangrene, closure of the abdomen
not increased. The metabolic rate and hormonal
and treatment withdrawal are considered.
response to stress and sepsis in infants may bedifferent from that of adults, and therefore, it is
Pre- and post-operative management
not possible to adapt recommendations made foradults to the neonatal population. It is possible that
Infants with NEC are amongst the most critically ill
neonates divert the products of protein synthesis
and most difficult patients to care for in paediatric
and breakdown from growth into tissue repair. This
surgery. Commonly, they are small premature
may explain the lack of growth commonly observed
neonates who require intensive care support and a
in infants with critical illness or sepsis. Further
team approach combining the expertise of paedi-
studies are needed in this field to delineate the
atric surgeons, neonatologists, intensivists, car-
metabolic response of newborn infants to NEC and
diologists and microbiologists. A nasogastric or
severe sepsis by exploring the relationship between
nutrition and immunity. The standard practise in
from 26 to 48 days. The usual management of
most paediatric surgical centres is to avoid enteral
post-NEC strictures is intestinal resection and pri-
feeding during the acute stage of the disease, and
NEC include intestinal malabsorption, short bowel
In addition to requiring nutritional support,
syndrome, hepatic cholestasis and recurrence of
neonates with NEC may present with clotting
NEC. Malabsorption can derive from various causes
abnormalities and require repeated transfusions of
including enzyme depletion, intestinal dysmotility,
platelets and clotting factors. The Thomsen–
hypersecretion of gastric acid and bacterial over-
Freidenreich (T) cryptantigen is a naturally occur-
growth.5 Short bowel syndrome is the most serious
ring antigen found on the surface of all human
long-term gastrointestinal complication of NEC
erythrocytes, and is normally concealed by a
with an incidence of up to 23% in NEC survivors.68
layer of N-acetylneuraminic acid. This antigen
Hepatic cholestasis is a common complication of
infants with NEC requiring long-term PN. The
acetylneuraminic acid layer is cleaved from the
factors contributing to the development of this
cell surface by neuraminidase, thus exposing
complication are likely to be multifactorial, and are
the underlying antigen. T cryptantigen activation
not yet fully determined. Neonates, especially
has been reported in some cases of neonatal
those born pre-term, with low-birthweight are par-
NEC.56–61 Activation of the T cryptantigen renders
ticularly at risk. Infection, intestinal bacterial over-
erythrocytes susceptible to haemolysis following
growth, and lack of enteral stimulation contribute
the transfusion of blood products containing anti-T
significantly to the development of the disease.5,69
antibodies. In a recent study of 104 neonates with
Introduction of minimal bolus enteral feeding in the
advanced NEC,62 the incidence of T cryptantigen
recovery phase of the disease is important because
activation was 22% and was significantly higher in
it stimulates gallbladder contractility,5,70,71 pro-
infants with stage III disease (30%) compared with
motes bile flow and aids in bowel adaptation.5 The
those with stage II disease (4%). Screening of
recurrence rate of NEC varies between 4 and
neonates with advanced NEC for T cryptantigen
6%.72,73 The presence of an intestinal stricture may
activation is advised to identify those at risk of
further promote the recurrence of NEC.
The neurodevelopmental implications of NEC
The only direct implication of T cryptantigen
have not been fully investigated. Approximately
activation for the management of NEC is that a
50% of the neonates with NEC are neurodevelop-
selective transfusion policy has been recommended
mentally normal.5,74 The neurological sequelae in
in order to reduce the risk of haemolysis. This has
children with NEC seems to be correlated with
been identified in a number of infants when NEC is
complicated by T cryptantigen activation and car-
medical diseases rather than with NEC itself.
ries a poor prognosis.63–65 In one series of 128
The mortality rate of neonates with NEC depends
infants with NEC, the mortality rate was 40% follow-
on the severity of the disease, associated anomalies
ing post-transfusion haemolysis compared with 6%
and gestational age. Over the past three decades,
when post-transfusion haemolysis did not occur.63
the survival rate of neonates with NEC has improved
When infants with T cryptantigen activation require
progressively. This has been most apparent in very
blood products, the use of packed red cells, washed
low-birthweight infants.5 In a study of 83 neonates
platelets and low titre anti-T FFP is advis-
who required a laparotomy for advanced NEC (Bell's
able.62,66,67 Should haemolysis occur, exchange
stage II and III), the overall mortality rate was 30%.
transfusion may abolish the haemolytic process and
Causes of death included multisystem organ failure
(nϭ10), sepsis (nϭ14) and congenital cardiacabnormality
occurred within 30 days from the diagnosis of NEC. Outcome of surgical intervention
The mortality rate was higher (67%) in patients withpanintestinal involvement of the disease compared
Approximately half of the neonates with NEC who
with patients with focal (12%) or multifocal NEC
clinical resolution of the disease. The most commoncomplication in this group of infants is post-NECintestinal stricture. Butter et al.20 reported an
Conclusions
incidence of post-NEC strictures of 48% in neonatestreated medically. The time, from the onset of NEC
The fact that so many infants with NEC survive is
until the diagnosis of intestinal stricture, ranged
testimonial to the advances in medical and surgical
Surgical treatment of infants with necrotizing enterocolitis
9. Rowe MI, Reblock KK, Kurkchubasche AG et al. Necrotiz-
ing enterocolitis in the extremely low birth weight infant. J Pediatr Surg 1994;29:987–90.
10. Ricketts RR. The role of paracentesis in the management of
infants with necrotizing enterocolitis. Am J Surg 1986; 52:61–5.
11. Hutter JJ Jr, Hathaway WE, Wayne ER. Hematologic ab-
normalities in severe neonatal necrotizing enterocolitis. J Pediatr 1976;88:1026–31.
12. O'Neill JAJ. Neonatal necrotizing enterocolitis. Surg ClinNorth Am 1981;61:1013.
13. O'Neill JAJ, Stalman TM, Meng HC. Nectrotizing entero-
colitis in the newborn. Ann Surg 1975;182:280–6.
14. Foglia RP. Necrotizing enterocolitis. Curr Probl Surg 1995;
32:757–823.
15. Pokorny WJ, Garcia-Prats JA, Barry YN. Necrotizing entero-
Mortality rate according to extent of the disease in 83
colitis: incidence, operative care, and outcome. J Pediatr
neonates with NEC who required laparotomy (adapted from
Surg 1986;21:1149–54.
16. Grosfeld JL, Chew H, Schlater M. Changing trends in necro-
tizing enterocolitis. Ann Surg 1991;214:300–7.
17. Ross MN, Waine ER, Janic JS et al. A standard for comparison
for acute surgical necrotizing enterocolitis. J Pediatr Surg 1989;24:938–1002.
care. Surgical intervention plays a vital role in the
18. Schrober PH, Nassiri J. Risk factors and severity indices in
treatment of a proportion of infants with NEC, and
necrotizing enterocolitis. Acta Paediatr 1994;396(Suppl):
is undoubtedly essential for their survival. How-
ever, the selective patients who would benefit
19. Kosloske AM. Surgery of necrotizing enterocolitis. World J
most from surgery and the precise nature of that
Surg 1985;9:277–84.
surgery remain largely unclear. Despite the intro-
20. Butter A, Flageole H, Laberge JM. The changing face of
surgical indications for necrotizing enterocolitis. J Pediatr
duction of new surgical techniques in recent years
Surg 2002;37:496–9.
and a general improvement in morbidity and mor-
21. Anveden-Hertzberg L, Gauderer MW. Surgery is safe in very
tality rates, there remains little consensus amongst
low birthweight infants with necrotizing enterocolitis. Acta
paediatric surgeons as to the most appropriate
Paediatr 2000;89:242–5.
way to treat many of these children. Prospective,
22. Pierro A. Necrotizing enterocolitis: pathogenesis and
multicentre, randomized controlled trials are
treatment. Br J Hosp Med 1997;58:126–8.
23. Fasoli L, Turi RA, Spitz L et al. Necrotizing enterocolitis:
required to enable us to answer these questions
extent of disease and surgical treatment. J Pediatr Surg
1999;34:1096–9.
24. Ein SH, Marshall DG, Girvan D. Peritoneal drainage under
References
enterocolitis. J Pediatr Surg 1977;12:963–7.
1. Walsh MC, Kliegman RM. Necrotizing enterocolitis: treat-
25. Ein SH, Shandling B, Wesson D et al. A 13-year experience
ment based on staging criteria. Pediatr Clin North Am 1986;
with peritoneal drainage under local anesthesia for necro-
33:179–201.
tizing enterocolitis perforation. J Pediatr Surg 1990;
2. Ververidis M, Kiely EM, Spitz L et al. The clinical significance
25:1034–6.
26. Cheu HW, Sukarochana K, Lloyd DA. Peritoneal drainage for
enterocolitis. J Pediatr Surg 2001;36:799–803.
necrotizing enterocolitis. J Pediatr Surg 1988;23:557–61.
3. Kosloske AM. Indications for operation in necrotizing
27. Morgan LJ, Shochat SJ, Hartman GE. Peritoneal drainage as
enterocolitis revisited. J Pediatr Surg 1994;29:663–6.
primary management of perforated NEC in the very low
4. Puntis J, McNeish AS, Allan RN. Long term prognosis of
birth weight infant. J Pediatr Surg 1994;29:30–4.
Crohn's disease with onset in childhood and adolescence.
28. Azarow KS, Ein SH, Shandling B et al. Laparotomy or drain
Gut 1984;25:329–36.
for perforated necrotizing enterocolitis: who gets what and
5. Albanese CT, Rowe MI. Necrotizing enterocolitis. In: O'Neill
why? Pediatr Surg Int 1997;12:137–9.
JAJ, Rowe MI, Grosfeld JL, Fonkalsrud EW, Coran AG,
29. Kosloske AM, Papile LA, Burstein J. Indications for operation
editors. Pediatric surgery. St Louis, MO: Mosby 1998;vol. 2:
in acute necrotizing enterocolitis of the neonate. Surgery
1980;87:502–8.
6. Stringer MD, Spitz L. Surgical management of neonatal
30. Martin LW, Neblett WW. Early operation with intestinal
necrotising enterocolitis. Arch Dis Child 1993;69:269–701.
diversion for necrotizing enterocolitis. J Pediatr Surg 1981;
7. Caty MG, Azizkhan RG. Nectrotizing enterocolitis. In:
16:252–5.
Ashcraft KW, Murphy JP, Sharp RJ, Sigalet DL, Snyder CL,
31. Musemeche CA, Kosloske AM, Ricketts RR. Enterostomy in
editors. Pediatric surgery. Philadelphia, PA: W.B. Saunders
necrotizing enterocolitis: an analysis of techniques and
timing of closure. J Pediatr Surg 1987;22:479–83.
8. Molik KA, West KW, Rescorla FJ et al. Portal venous air: the
32. Sparnon AL, Kiely EM. Resection and primary anastomosis
poor prognosis persists. J Pediatr Surg 2001;36:1143–5.
for necrotizing enterocolitis. Pediatr Surg Int 1987;2:101–4.
33. Moss RL, Dimmitt RA, Henry MC et al. A meta-analysis
cial nutrition in support in clinical practice. London: Edward
of peritoneal drainage versus laparotomy for perforated
necrotizing enterocolitis. J Pediatr Surg 2001;36:1210–3.
55. Powis MR, Smith K, Rennie M et al. Characteristics of protein
34. Rovin JD, Rodgers BM, Burns RC et al. The role of peritoneal
and energy metabolism in neonates with necrotizing
drainage for intestinal perforation in infants with and with-
enterocolitis—a pilot study. J Pediatr Surg 1999;34:5–10.
out necrotizing enterocolitis. J Pediatr Surg 1999;34:143–7.
56. Kirsten GF, Smith J, Pieper C et al. The necessity for
35. Cass DL, Brandt ML, Patel DL et al. Peritoneal drainage as
T-cryptantigen activation screening in babies with necrotis-
definitive treatment for neonates with isolated intestinal
ing enterocolitis. S Afr Med J 1996;86:546–8.
perforation. J Pediatr Surg 2000;35:1531–6.
57. Klein RL, Novak RW, Novak PE. T-cryptantigen exposure in
36. Tam PKH. Necrotizing enterocolitis—surgical management.
neonatal necrotizing enterocolitis. J Pediatr Surg 1986;
Semin Neonatol 1997;2:297–305. 21:1155–8.
37. O'Connor A, Sawin RS. High morbidity of enterostomy and its
58. Mupanemunda RH, Kenyon CF, Inwood MJ et al. Bacterial-
closure in premature infants with necrotizing enterocolitis.
induced activation of erythrocyte T-antigen complicating
Arch Surg 1998;133:875–80.
necrotising enterocolitis: a case report. Eur J Pediatr 1993;
38. Kiesewetter WB, Taghizadeh F, Bower RJ. Necrotizing
152:325–6.
enterocolitis: is there a place for resection and primary
59. Seges RA, Kenny A, Bird GW et al. Pediatric surgical patients
anastomosis? J Pediatr Surg 1979;14:360–2.
with severe anaerobic infection: report of 16 T-antigen
39. Harberg FJ, McGill CW, Saleem MM et al. Resection with
positive cases and possible hazards of blood transfusion.
primary anastomosis for necrotizing enterocolitis. J PediatrJ Pediatr Surg 1981;16:905–10. Surg 1983;18:743–6.
60. Squire R, Kiely E, Drake D et al. Intravascular haemolysis in
40. Griffiths DM, Forbes DA, Pemberton PJ et al. Primary
association with necrotising enterocolitis. J Pediatr Surg
1992;27:808–10.
experience. J Pediatr Surg 1989;24:515–8.
61. Williams RA, Brown EF, Hurst D et al. Transfusion of infants
41. Parigi GB, Bragheri R, Minniti S et al. Surgical treatment
with activation of erythrocyte T antigen. J Pediatr 1989;
of necrotizing enterocolitis: when? how? Acta Paediatr115:949–53.
1994;396(Suppl):58–61.
62. Hall N, Ong EG, Ade-Ajayi N et al. T cryptantigen activa-
42. Cooper A, Ross A III, O'Neill JA et al. Resolution of intract-
tion is associated with advanced necrotizing enterocolitis.
able cholestasis associated with total parenteral nutrition
J Pediatr Surg 2002;37:791–3.
following biliary irrigation. J Pediatr Surg 1985;20:772–4.
63. Novak RW, Abbott AE Jr, Klein RL. T-cryptantigen determi-
43. Ade-Ajayi N, Kiely E, Drake D et al. Resection and primary
nation affects mortality in necrotizing enterocolitis. Surg
anastomosis in necrotizing enterocolitis. J R Soc Med 1996;
Gynecol Obstet 1993;176:368–70. 89:385–8.
64. Anand KJ, Hickey PR. Halothane–morphine compared with
44. Parigi GB, Bragheri R, Minniti S et al. Surgical treatment
high-dose sufentanil for anesthesia and postoperative anal-
of necrotizing enterocolitis: when? how? Acta Paediatr
gesia in neonatal cardiac surgery see comments. N Engl J
1994;396(Suppl):58–61. Med 1992;326:1–9.
45. Cooper A, Ross AJ III, O'Neill JA Jr et al. Resection
65. Cruickshank AM, Fraser WD, Burns HJ et al. Response of
with primary anastomosis for necrotizing enterocolitis: a
serum interleukin-6 in patients undergoing elective surgery
contrasting view. J Pediatr Surg 1988;23:64–8.
of varying severity. Clin Sci (Colch) 1990;79:161–5.
46. Ade-Ajayi N, Kiely E, Drake D et al. Resection and primary
66. Facchinetti F, Bagnoli F, Bracci R et al. Plasma opioids in the
anastomosis in necrotizing enterocolitis. J R Soc Med 1996;
first hours of life. Pediatr Res 1982;16:95–8. 89:385–8.
67. Chwals WJ. The newborn as a surgical patient. Metabolic
47. Ladd AP, Rescorla FJ, West KW et al. Long-term follow-up
considerations. In: Rowe MI, Grosfeld JL, Fonkalsrud EW,
after bowel resection for necrotizing enterocolitis: factors
Coran AG, editors. Pediatric surgery. St Louis, MO: Mosby
affecting outcome. J Pediatr Surg 1998;33:967–72.
48. Touloukian RJ, Smith GJ. Normal intestinal length in
68. Ricketts RR. Surgical treatment of necrotizing enterocolitis
preterm infants. J Pediatr Surg 1983;18:720–3.
and the short bowel syndrome. Clin Perinatol 1994;
49. Sugarman ID, Kiely EM. Is there a role for high jejunostomy
21:365–87.
in the management of severe necrotising enterocolitis?
69. Pierro A. Cholestatic jaundice in newborn infants receiving
Pediatr Surg Int 2001;17:122–4.
parenteral nutrition. Semin Neonatol 1996;1:1–4.
50. Vaughan WG, Grosfeld JL, West K et al. Avoidance of stomas
70. Jawaheer G, Pierro A, Lloyd DA et al. Gall bladder contrac-
and delayed anastomosis for bowel necrosis: the ‘clip and
tility in neonates: effects of parenteral and enteral feeding
drop-back’ technique. J Pediatr Surg 1996;31:542–5.
published erratum appears in Arch Dis Child Fetal Neonatal
51. Moore TC. Successful use of the ‘patch, drain, and wait’
Ed 1995; 73:F198. Arch Dis Child Fetal Neonatal Ed 1995;
laparotomy approach to perforated necrotizing entero-
72:F200–2.
colitis: is hypoxia-triggered ‘good angiogenesis’ involved?
71. Jawaheer G, Shaw NJ, Pierro A. Continuous enteral feeding
Pediatr Surg Int 2000;16:356–63.
impairs gallbladder emptying in infants. J Pediatr 2001;
52. Vlessis AA, Goldman RK, Trunkey DD. New concepts in the
138:822–5.
pathophysiology of oxygen metabolism during sepsis see
72. Ricketts RR, Jerles ML. Neonatal necrotizing enterocolitis:
comments. Br J Surg 1995;82:870–6.
experience with 100 consecutive surgical patients. World J
53. Plank LD, Connolly AB, Hill GL. Sequential changes in the
Surg 1990;14:600–5.
metabolic response in severely septic patients during the
73. Stringer MD, Brereton RJ, Drake DP et al. Recurrent necro-
first 23 days after the onset of peritonitis see comments.
tizing enterocolitis. J Pediatr Surg 1993;28:979–81. Ann Surg 1998;228:146–58.
74. Stevenson DK, Kerner JA, Malachowski N et al. Late mor-
54. Takala J, Pitkanen O. Nutrition support in trauma and
sepsis. In: Payne-James J, Grimble G, Silk D, editors. Artifi-
Pediatrics 1980;66:925–7.
THIS CIRCULAR IS IMPORTANT AND REQUIRES YOUR IMMEDIATE ATTENTIONHong Kong Exchanges and Clearing Limited and The Stock Exchange of Hong Kong Limited take noresponsibility for the contents of this circular, make no representation as to its accuracy or completeness andexpressly disclaim any liability whatsoever for any loss howsoever arising from or in reliance upon the wholeor any part of the co
Les damos la Bienvenida al XXI Congreso de nuestra querida Sociedad. Para nosotros es un privilegio hacerlo en la provincia de Mendoza, que nos recibirá con suinigualable belleza, calidez de sus habitantes. La Comisión Directiva que tengo el orgullo de presidir, junto al Comité Organizador local, hadesplegado todo su esfuerzo para que este Congreso sea no sólo un éxito en su programa-ción
 Seminars in Neonatology (2003) 8, 223–232
Seminars in Neonatology (2003) 8, 223–232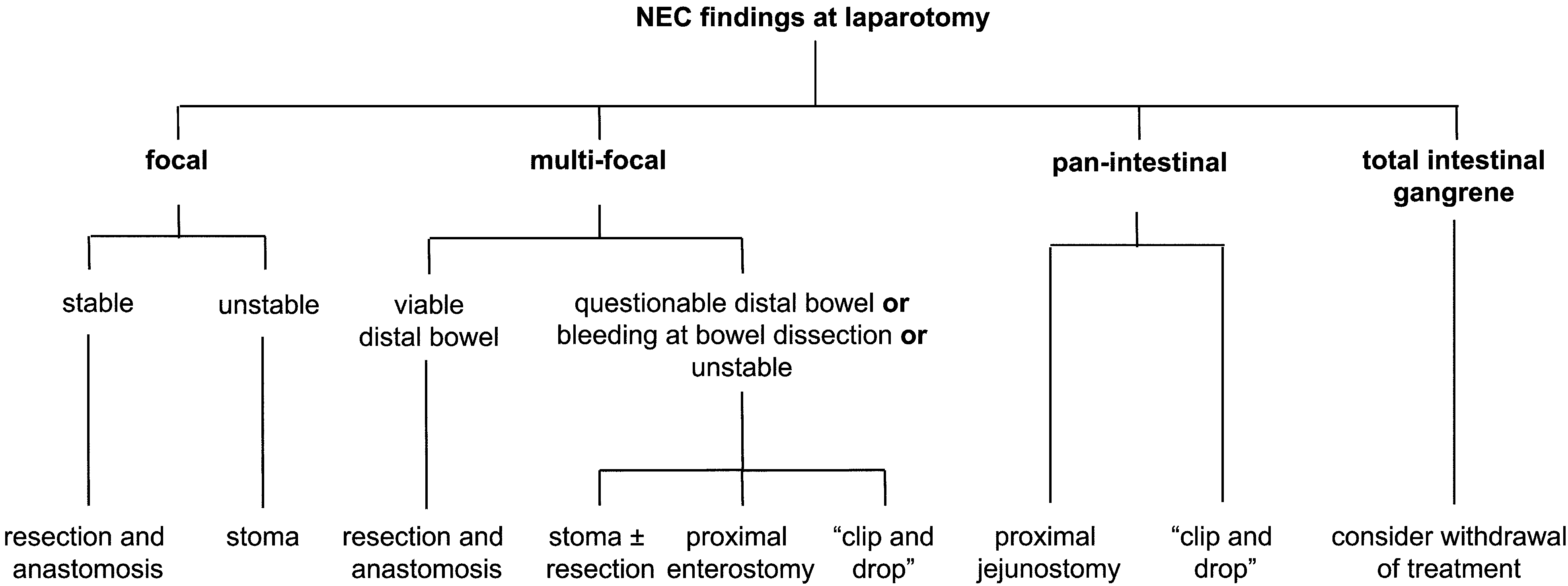 Surgical treatment of infants with necrotizing enterocolitis
Authors preferred operative management of advanced NEC.
Surgical treatment of infants with necrotizing enterocolitis
Authors preferred operative management of advanced NEC.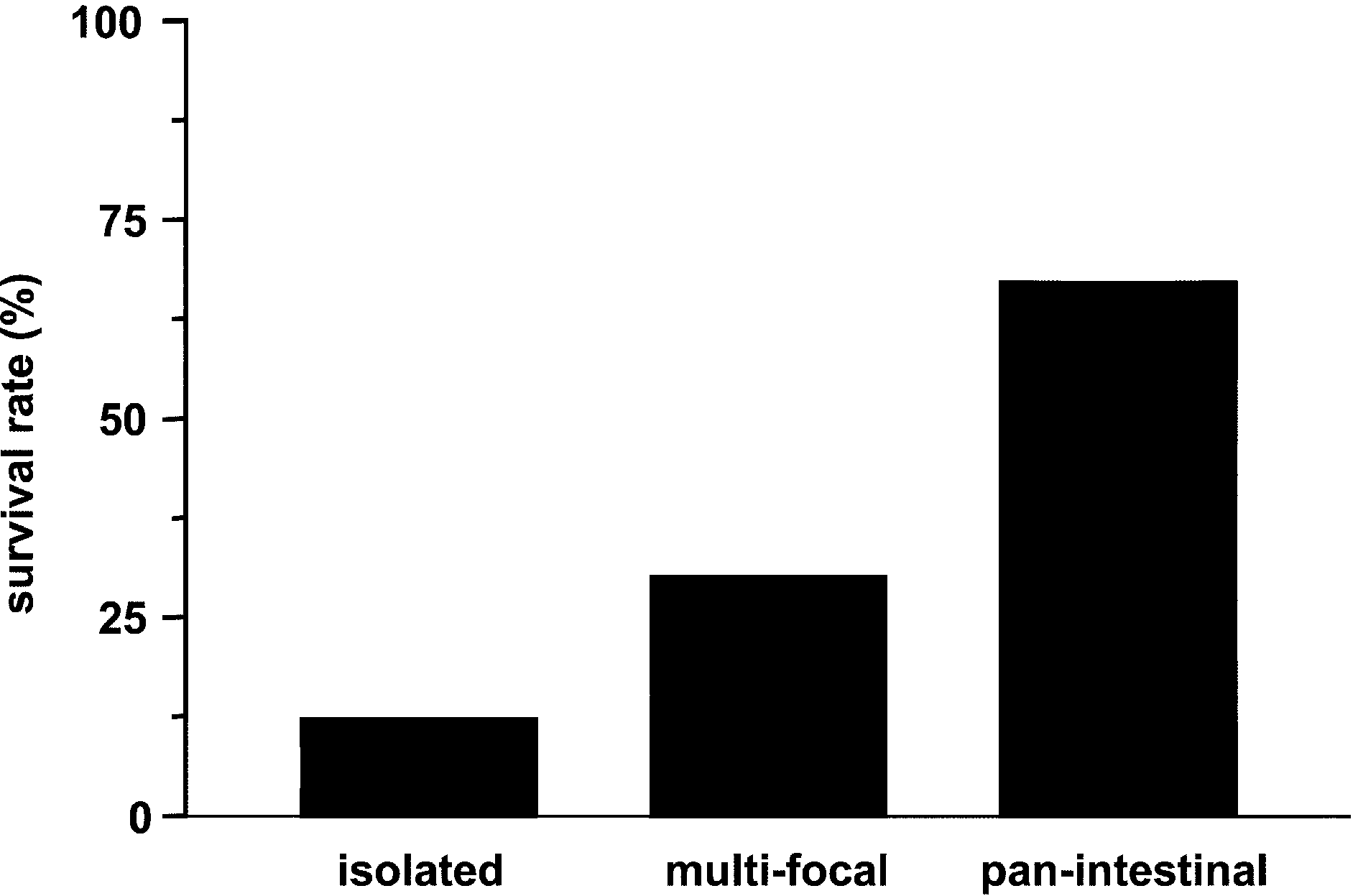 Surgical treatment of infants with necrotizing enterocolitis
9. Rowe MI, Reblock KK, Kurkchubasche AG et al. Necrotiz-
ing enterocolitis in the extremely low birth weight infant.
Surgical treatment of infants with necrotizing enterocolitis
9. Rowe MI, Reblock KK, Kurkchubasche AG et al. Necrotiz-
ing enterocolitis in the extremely low birth weight infant.