PATIENT NAME: _________________________________ *Due to the nature of our specialty there may be patients that require additional time than was allowed for their appointment. This may lead to extended wait times. We appreciate your patience in allowing us to provide optimum care to all our patients.
Patient Medical History
History of problem for which you are seeing us
Duration of symptoms _____________________________________________________
How did problem start? No injury/event At work (date________) Home/leisure.
Briefly describe events: ____________________________________________________
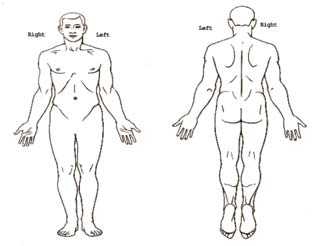
If you have pain or numbness: Mark “X” on the body part(s) with pain.
Mark “O” on body part(s) with numbness. Pain Scale Please circle appropriate number: 1 = no pain, 10 = severe pain.
Typically, pain level is: 1-----2-----3----4----5----6----7----8----9----10
At its worst, my pain is: 1-----2-----3----4----5----6----7----8----9----10
At its best, my pain level is: 1-----2-----3----4----5----6----7----8----9----10
Character of pain: Burning Stabbing Deep ache Frequency: Constant Intermittent Rare Improvement? (since onset) Worsened Improved Stayed the same Weakness: Yes No
Diagnostic History X-rays Yes No Date/Location _____________________ MRI Yes No Date/Location _____________________ CT scan Yes No Date/Location _____________________ Bone scan Yes No Date/Location _____________________ EMG Yes No Date/Location _____________________ Other Yes No Date/Location _____________________
Allergies _________________________________________________________________________ What is your reaction to this allergy? _________________________________________________ MedicationsExample:Received: Did it work? Anti-inflammatory Naprosyn, Ibuprofen Y – N Y – N Muscle relaxer Soma, Flexeril, Skelaxin Y – N Y – N Pain medication Tylenol w/codeine, Vicodin, Darvocet, Percocet Y – N Y – N Oral Steroid Medrol Dose Pak, Prednisone Y – N Y – N Nerve medication Lyrica, Neurontin Y – N Y – N TreatmentsReceived: Did it help? Consultations
Have you seen another spine care specialist for this problem? Yes No
If yes, Date_______________ Name of Physician:______________________
Recommendations/treatments: ___________________________________________
Legal advice
Do you have an attorney regarding this injury/problem? Yes No
If yes, please list the attorney’s name: _____________________________________
Past Medical History (circle all that you have experienced)
Other problems: __________________________________________________________________________
Surgeries Date
Work Status Number of years at current job: _______ Are you currently employed? Yes No If so: Regular duty Modified duty Working hrs / week __________ Where are you currently employed? ____________________________________________________________ What is your current occupation? ______________________________________________________________ What are your restrictions? _____________________________________________________________ Who wrote the restrictions? _____________________________________________________________ Review of Systems (In the past month, have you experienced any of the following? Please check each box.) (If you have any of these symptoms, please notify your family doctor.) HEENT Integumentary General Neurologic Abdominal: Gastrointestinal:
Pulmonary: Cardiovascular: Medications (Please list all the medications you are currently taking.) Medication Dose & times/day Medication Dose & times/day
Do you: Smoke: yes no _____Packs/day _____ # of YRS. Past smoker? yes no _____Packs/day _____ # of YRS.
Drink alcohol: yes no _____ # drinks/week.
Smoking and chewing tobacco is a leading risk factor in the development of degenerative disc disease. A disc is the shock absorber between the bones in your spine. When the disc starts to wear out it loses some of its ability to provide a "cushion" between bones. This allows for a greater risk of rupture. The discs already have a poor blood supply and when you smoke or use tobacco the blood vessels constrict (narrow) and the oxygen supply is lowered even more. Smokers also introduce carbon monoxide into the blood stream which can inhibit the discs' ability to absorb needed nutrients from the blood. This leads to dehydrated discs and eventually degenerative disc disease. If your spinal condition deteriorates enough to need a fusion surgery you will need to stop smoking or using tobacco. Nicotine is a bone toxin and can slow down new bone growth. The failure rate for many fusions can be 3 to 4 times higher for someone using tobacco. Many times you cannot have your surgery until you have been able to stop smoking or using tobacco. There are a number of different options available to assist in smoking or tobacco cessation. Please let us know when you are ready to quit using tobacco. If you are a current smoker, please initial and date here stating that you have read and understand the above smoking cessation recommendation:
Family History Relation State of health If deceased, age and cause of death
________________________________________________________________
Mother ________________________________________________________________ Brothers ________________________________________________________________ Sisters
________________________________________________________________
________________________________________________________________
________________________________________________________________
FARMAKOTERAPIA W PSYCHIATRII I NEUROLOGII, 2005, 3, 273278Zaburzenia czynnoci p³ciowych u pacjentówThe sexual dysfunction in multiple sclerosis patientsII Klinika Neurologiczna Instytutu Psychiatrii i Neurologii w WarszawieStreszczenieZaburzenia seksualne s¹ istotnym, jednak¿e doæ czêsto pomijanym problemem u pacjentów zestwardnieniem rozsianym (s.r.). Mog¹ one byæ istotn¹ prz
Etiology and Management of Chylothorax Following Pediatric Heart Surgery Michael Milonakis, M.D., Andrew C. Chatzis, M.D., Nikolaos M. Giannopoulos, M.D., Constantinos Contrafouris, M.D., Dimitrios Bobos, M.D., George V. Kirvassilis, M.D., and George E. Sarris, M.D. Department of Pediatric and Congenital Cardiac Surgery, Onassis Cardiac Surgery Center,Athens, Greece ABSTRACT Background: Chyl
 John Hammerstein, MD
John Hammerstein, MD