The American Journal of Medicine (2006) 119, e3-e5
CLINICAL COMMUNICATION TO THE EDITOR Rituximab-induced Elimination of Acquired
frequent administration of C1-inhibitor concentrate, leading
Angioedema Due to C1-Inhibitor Deficiency
to very frequent attacks of severe These at-tacks may be life-threatening and obviously have a major
impact on morbidity and quality of life.
Here we describe 3 patients with such a therapy-resistant
Acquired deficiency of C1 inhibitor is a relatively rare
severe acquired deficiency of C1 inhibitor, who show a
but serious disorder, causing frequently occurring, severe
normalization of C1-inhibitor plasma levels and a complete
remission of angioedema attacks after treatment with anti-
ciency of C1 inhibitor may be caused by the formation of
auto-antibodies (type II ) but may also occur in the settingof lymphoproliferative disorders (type In the latter
CASE REPORT
case, at least 2 mechanisms have been proposed to explainthe decrease of C1 inhibitor. One involves anti-C1-inhibitor
Three patients with acquired angioedema had very frequent
specificity of the antibody produced by the malignant B-cell
(Ͼ1/10 days) angioedema attacks despite treatment with
clone; the other assumes consumption of C1 inhibitor by
danazol (150-300 mg/day), alone or in combination with
excessive activation of C1, the first complement factor, by
tranexamic acid (2-3 g daily). Severe angioedema attacks
immune complexes consisting of the idiotype of the anti-
(defined as an attack in the upper airway or a serious
body produced by the malignant clone and anti-idiotype
abdominal attack) were treated with intravenous adminis-
antibodies. The ongoing consumption of C1 inhibitor in the
tration of 1000 U of plasma-derived C1-inhibitor concen-
latter situation will cause a deficiency of this protease in-
trate (Sanquin, Amsterdam, the Netherlands). The 3 patients
It is becoming increasingly clear that many of the
had high requirements for C1-inhibitor concentrate admin-
patients with lymphoproliferative disorders have specific
istration (mean consumption 2500-9000 U/month). The di-
anti-C1 inhibitor antibodies, making the distinction between
agnostic criteria for acquired angioedema were based on the
type I and II forms of acquired C1-inhibitor deficiency less
clinical presentation with recurrent attacks of angioedema,
the absence of a family history of C1-inhibitor deficiency,
Patients with acquired C1-inhibitor deficiency can some-
onset of the angioedema attacks at age Ͼ25 years, a low
times be successfully managed by treatment of the under-
level of C1-inhibitor (Ͻ0.5 U/mL) and C4 (Ͻ100 mg/L) in
lying disorder, and patients in which no such underlying
plasma, low levels of C1q (Ͻ80 IU/mL), the presence of
disease is diagnosed or who do not require specific treat-
anti-C1-inhibitor antibodies (optionally), and a diagnosis of
ment for this disease are treated with androgenic steroids,
a lymphoproliferative disorder (optionally).
such as danazol (which stimulates hepatic production of
One of the patients (patient A, female, age 45 years) had
or with lysine analogues, such as epsilon
positive anti-C1-inhibitor IgG antibodies. One patient (pa-
caproic acid or tranexamic acid (which act by inhibition of
tient B, female, age 70 years) was recently diagnosed with
plasmin formation, that is important in the pathogenesis of
an indolent follicular B-cell lymphoma, stage IV, with lo-
In case of severe angioedema (for example,
calization in spleen, bone marrow and peripheral blood, for
located in the upper airways or severe abdominal attacks)
which no specific treatment was given so far, and in 1
patient (patient C, male, age 68 years) no underlying cause
for the C1-inhibitor deficiency was found. Patient A and
immunosuppressive agents in patients with autoimmune C1
patient C were diagnosed with acquired C1-inhibitor defi-
inhibitor deficiency is successful in some but not all
ciency for 12 and 7 years, respectively.
Although the majority of patients can be managed success-
In an attempt to reduce the frequency and severity of the
fully, some patients are resistant to treatment, even despite
angioedema attacks, patient A and C were treated withprednisolone (50 mg/day) in combination with cyclophos-phamide (150 mg/day). However, these treatment regimens
Requests for reprints should be addressed to Marcel Levi, MD, De-
had no effect at all on the clinical course or C1-inhibitor
partment of Internal Medicine, Academic Medical Centre F-4, Meiberg-
levels in plasma during 3-6 months follow-up. Hereupon
dreef 9, 1105 AZ Amsterdam, the Netherlands.
and after provision of informed consent by the patients, all
0002-9343/$ -see front matter 2006 Elsevier Inc. All rights reserved.
The American Journal of Medicine, Vol 119, No 8, August 2006
3 patients were treated with anti-CD20 monoclonal antibod-ies (Rituximab, Roche, the Netherlands, 375 mg/m2, onceevery week for a total of 4 doses). After 3-4 months fol-lowing this treatment, in all 3 patients the frequency ofangioedema attacks was drastically reduced, along with amarked reduction in C1-inhibitor concentrate requirement,and after 8-10 months, patients were completely free fromany angioedema attack The clinical improvementwas associated with increasing levels of C1-inhibitor inplasma to (near) normal levels at 10-12 months after treat-ment and a normalization of C4 levels in 2 of 3 patientsNo adverse effects of the treatment were noted inthe patients, except for some mild diffuse muscle and jointpain in 1 patient starting after the fourth administration ofanti-CD20 antibodies and persisting for 4-5 months. DISCUSSION We here show successful treatment of acquired angioedema with administration of anti-CD20 antibodies in 3 patients. Patients with very frequent attacks of severe angioedema requiring high doses of C1-inhibitor concentrate became asymptomatic 3-4 months after anti-CD20 treatment. Al- though we realize that this type of case series with success- ful outcome does not provide the ultimate proof of efficacy of this treatment for patients with acquired C1-inhibitor deficiency, we feel the results are rather compelling and suggest that further study is warranted. It is not very likely that spontaneous remission of acquired C1-inhibitor defi- ciency would have occurred in the 2 patients with a very long history of this disorder or in the untreated patient with acquired angioedema and the indolent B-cell lymphoma. Another limitation of this observation is that it is not yet clear whether the effect of CD20 antibody treatment is definitive or that relapse of the disease will occur. So far, patients have been followed for a mean period of 12 months without signs of recurrence of angioedema, but we realize that a longer follow-up period may be required. Neverthe- less, when a relapse occurs, repeat treatment with anti- CD20 antibodies is an option to be considered.
Rituximab is a chimeric antibody directed toward human
CD20, and its administration leads to a transient eliminationof CD20-positive B-cells by thus far not completely under-stood mechanisms, including antibody-dependent cellularcytotoxicity, complement activation, and induction of B-celThis CD20-directed treatment has beenshown to be highly effective in the (adjunctive) treatment oflymphoproliferative disorders, in particular B-cell lympho-
Effect of the administration of anti-CD20 antibodies
In addition, rituximab also has been shown to be
(indicated with arrows) in 3 patients with acquired C1-inhibitor
effective in therapy-resistant autoimmune such
deficiency (patient A: ‘ and black bars, patient B: and stripedbars, patient C: ● and white bars) on plasma levels of C1-inhibitor
and C4, frequency of serious angioedema attacks (upper airway
edema, facial edema, severe edema of extremities or genitals, and
report suggested that administration of Rituximab in a pa-
severe abdominal attacks) and the monthly requirement for C1-
tient with diffuse B-cell lymphoma also affected the occur-
rence of angioedema attacks in this In our expe-rience presented here, anti-CD20 treatment was effective inboth auto-antibody-associated C1-inhibitor deficiency and
Rituximab-induced Elimination of Acquired Angioedema
in the patients with C1-inhibitor deficiency in the frame-
3. Jackson J, Sim RB, Whelan A, Feighery C. An IgG autoantibody
work of a lymphoproliferative disorder. It is likely that in
which inactivates C1-inhibitor. Nature. 1986;323:722-724.
4. Cicardi M, Zingale LC, Pappalardo E, Folcioni A, Agostoni A. Au-
both situations the point of impact of anti-CD20 antibodies
toantibodies and lymphoproliferative diseases in acquired C1-inhibitor
must be the antibody producing B-cell clone. Importantly,
deficiencies. Medicine (Baltimore). 2003;82:274-281.
as mentioned before, the distinction between the 2 types of
5. Carugati A, Pappalardo E, Zingale LC, Cicardi M. C1-inhibitor defi-
acquired angioedema is rather unclear and many overlap
ciency and angioedema. Mol Immunol. 2001;38:161-173.
6. D’Incan M, Tridon A, Ponard D, et al. Acquired angioedema with C1
inhibitor deficiency: is the distinction between type I and type II still
In conclusion, we here demonstrate successful treatment
relevant? Dermatology. 1999;199:227-230.
of severe and conventional treatment-resistant acquired an-
7. Cicardi M, Beretta A, Colombo M, Gioffre D, Cugno M, Agostoni A.
gioedema due to deficiency of C1 inhibitor with the admin-
Relevance of lymphoproliferative disorders and of anti-C1 inhibitor
istration of anti-CD20 antibodies. Additional experience,
autoantibodies in acquired angio-oedema. Clin Exp Immunol. 1996;
and preferably, a controlled trial of anti-CD20 antibody
8. Chevailler A, Arlaud G, Ponard D, et al. C-1-inhibitor binding mono-
treatment in patients with acquired C1 inhibitor deficiency,
clonal immunoglobins in three patients with acquired angioneurotic
is required to confirm these observations, although we re-
edema. J Allergy Clin Immunol. 1996;97:998-1008.
alize that execution of a clinical trial may be difficult in
9. Agostoni A, Aygoren-Pursun E, Binkley KE, et al. Hereditary and
view of the limited number of patients.
acquired angioedema: problems and progress: proceedings of the thirdC1 esterase inhibitor deficiency workshop and beyond. J Allergy Clin
10. Smith MR. Rituximab (monoclonal anti-CD20 antibody): mechanisms
of action and resistance. Oncogene. 2003;22:7359-7368.
11. Silverman GJ, Weisman S. Rituximab therapy and autoimmune dis-
orders: prospects for anti-B cell therapy. Arthritis Rheum. 2003;48:
12. McLaughlin P, Grillo-Lopez AJ, Link BK, et al. Rituximab chimeric
anti-CD20 monoclonal antibody therapy for relapsed indolent lym-
phoma: half of patients respond to a four-dose treatment program. J Clin Oncol. 1998;16:2825-2833.
13. Coiffier B, Lepage E, Briere J, et al. CHOP chemotherapy plus ritux-
imab compared with CHOP alone in elderly patients with diffuse
large-B-cell lymphoma. N Engl J Med. 2002;346:235-242.
14. Edwards JC, Cambridge G. Prospects for B-cell-targeted therapy in
autoimmune disease. Rheumatology (Oxford). 2005;44:151-156.
15. Stasi R, Pagano A, Stipa E, Amadori S. Rituximab chimeric anti-CD20
monoclonal antibody treatment for adults with chronic idiopathicthrombocytopenic purpura. Blood. 2001;98:952-957.
16. Looney RJ, Anolik JH, Campbell D, et al. B cell depletion as a novel
treatment for systemic lupus erythematosus: a phase I/II dose-escala-tion trial of rituximab. Arthritis Rheum. 2004;50:2580-2589. References
17. Edwards JC, Szczepanski L, Szechinski J, et al. Efficacy of B-cell-
1. Agostoni A, Cicardi M. Hereditary and acquired C1-inhibitor defi-
targeted therapy with rituximab in patients with rheumatoid arthritis.
ciency: biological and clinical characteristics in 235 patients. MedicineN Engl J Med. 2004;350:2572-2581. (Baltimore). 1992;71:206-215.
18. Ziakas PD, Giannouli S, Psimenou E, Evangelia K, Tzioufas AG,
2. Markovic SN, Inwards DJ, Frigas EA, Phyliky RP. Acquired C1
Voulgarelis M. Acquired angioedema: a new target for rituximab?
esterase inhibitor deficiency. Ann Intern Med. 2000;132:144-150. Haematologica. 2004;89:ELT13.
PATIENT NAME: ____________________________________________________________________ WHAT IS THE MAIN REASON FOR YOUR CHILD’S VISIT TODAY______________________________ HOW LONG HAS THIS PROBLEM EXISTED________________________________________________ PLEASE MAKE A CHECK MARK BY YOUR CONCERNS EAR PROBLEMS NOSE PROBLEMS THROAT/MOUTH/NECK PROBLEMS ____HOARSENESS/VOICE
Benfotiamine Inhibits Intracellular Formation of Advanced Glycation End Products in vivo JIHONG LIN, ALEX ALT, JUTTA LIERSCH, REINHARD G. BRETZEL, MICHAEL BROWNLEE*, HANS-PETER HAMMES Third Medical Department, Justus-Liebig-University Giessen, Germany *Albert-Einstein College, New York, NY, USA ABSTRACT Glycolysis We have demonstrated previously that intrac
 The American Journal of Medicine (2006) 119, e3-e5
CLINICAL COMMUNICATION TO THE EDITOR
The American Journal of Medicine (2006) 119, e3-e5
CLINICAL COMMUNICATION TO THE EDITOR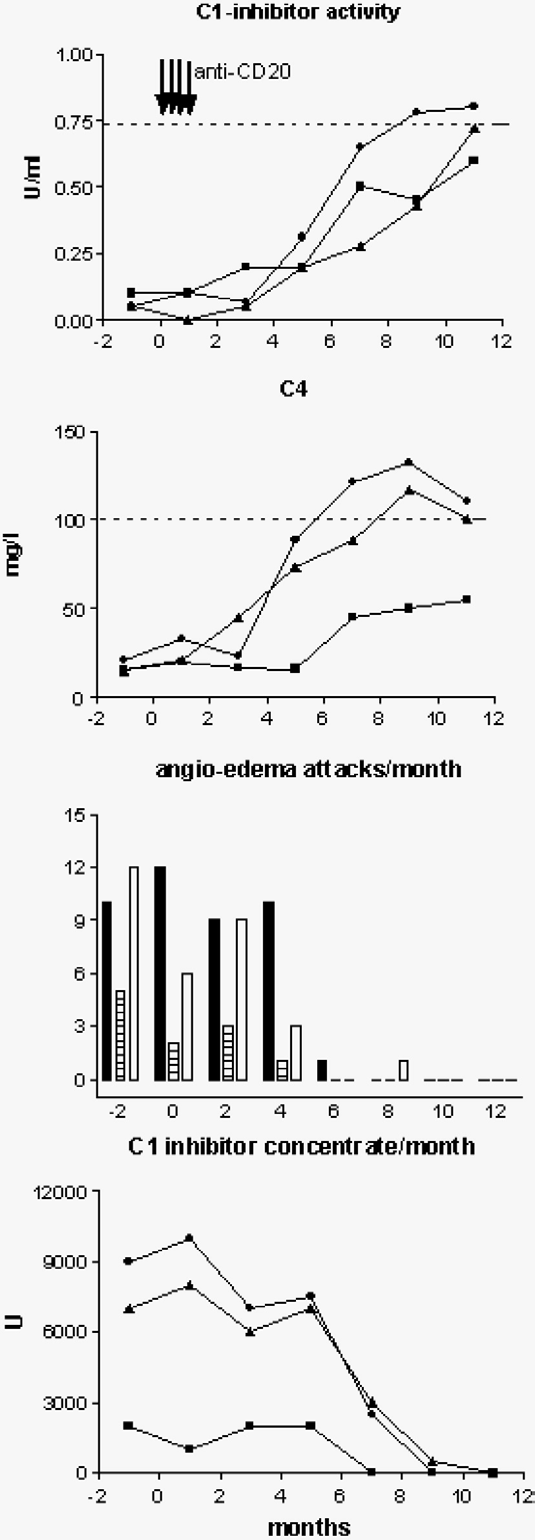 The American Journal of Medicine, Vol 119, No 8, August 2006
3 patients were treated with anti-CD20 monoclonal antibod-ies (Rituximab, Roche, the Netherlands, 375 mg/m2, onceevery week for a total of 4 doses). After 3-4 months fol-lowing this treatment, in all 3 patients the frequency ofangioedema attacks was drastically reduced, along with amarked reduction in C1-inhibitor concentrate requirement,and after 8-10 months, patients were completely free fromany angioedema attack The clinical improvementwas associated with increasing levels of C1-inhibitor inplasma to (near) normal levels at 10-12 months after treat-ment and a normalization of C4 levels in 2 of 3 patientsNo adverse effects of the treatment were noted inthe patients, except for some mild diffuse muscle and jointpain in 1 patient starting after the fourth administration ofanti-CD20 antibodies and persisting for 4-5 months.
The American Journal of Medicine, Vol 119, No 8, August 2006
3 patients were treated with anti-CD20 monoclonal antibod-ies (Rituximab, Roche, the Netherlands, 375 mg/m2, onceevery week for a total of 4 doses). After 3-4 months fol-lowing this treatment, in all 3 patients the frequency ofangioedema attacks was drastically reduced, along with amarked reduction in C1-inhibitor concentrate requirement,and after 8-10 months, patients were completely free fromany angioedema attack The clinical improvementwas associated with increasing levels of C1-inhibitor inplasma to (near) normal levels at 10-12 months after treat-ment and a normalization of C4 levels in 2 of 3 patientsNo adverse effects of the treatment were noted inthe patients, except for some mild diffuse muscle and jointpain in 1 patient starting after the fourth administration ofanti-CD20 antibodies and persisting for 4-5 months.