Anti-hyperglycemic and Anti-hypercholesterolemicEffects of Aloe vera Leaf Gel in Hyperlipidemic Type 2Diabetic Patients: A Randomized Double-Blind Placebo-Controlled Clinical Trial
Hasan Fallah Huseini1, Saeed Kianbakht1, Reza Hajiaghaee2, Fataneh Hashem Dabaghian3
1 Department of Pharmacology and Applied Medicine, Research Institute of Medicinal Plants, ACECR, Karaj, Iran2 Department of Pharmacognosy and Pharmacy, Research Institute of Medicinal Plants, ACECR, Karaj, Iran3 Research Institute for Islamic and Complementary Medicine, Tehran University of Medical Sciences, Tehran, Iran
drugs in treatment of 30 patients were evaluated
Diabetes mellitus type 2 with dyslipidemia is a
and compared with the placebo group (n = 30).
common disease. Previous studies suggest that
The aloe gel lowered the fasting blood glucose,
aloe (Aloe vera L.) leaf gel may positively affect
HbA1c, total cholesterol, and LDL levels signifi-
the blood glucose and lipid levels in dyslipidemic
type 2 diabetic patients. Thus, in this randomized
p = 0.004, respectively) without any significant ef-
fects on the other blood lipid levels and liver/kid-
with hyperlipidemic (hypercholesterolemic and/
ney function tests (p > 0.05) compared with the
or hypertriglyceridemic) type 2 diabetic patients
placebo at the endpoint. No adverse effects were
aged 40 to 60 years not using other anti-hyper-
reported. The results suggest that aloe gel may be
lipidemic agents and resistant to daily intake of
a safe anti-hyperglycemic and anti-hypercholes-
two 5 mg glyburide tablets and two 500 mg met-
terolemic agent for hyperlipidemic type 2 diabet-
formin tablets, the efficacy and safety of taking
aloe gel (one 300 mg capsule every 12 hours for 2
rently, there is renewed interest in the plant-
based medicines and functional foods modulating
Type 2 diabetes mellitus (T2DM) is common
physiological effects in the prevention and cure of
Downloaded by: Tel Aviv University. Copyrighted material.
worldwide [1]. Type 2 diabetic patients frequently
diabetes. The plant kingdom is a wide field to
have dyslipidemia [increased low-density lipo-
search for natural effective oral anti-hyperglyce-
mic agents that have slight or no side effects.
(VLDL) and triglycerides, and decreased high-
More than about 1200 plant species have been re-
density lipoprotein (HDL)]. The lipid changes are
corded to be used empirically for their alleged
attributed to increased free fatty acid flux second-
anti-hyperglycemic activity [12]. Aloe (Aloe vera
ary to insulin resistance. Dyslipidemia is one of
L., Liliaceae family) is a popular traditional reme-
the major risk factors for premature cardiovascu-
dy for numerous diseases such as diabetes melli-
lar morbidity and mortality in the T2DM patients
tus in several cultures [13, 14]. A variety of phar-
[2, 3]. Multiple anti-hyperglycemic and anti-hy-
macological effects have been demonstrated for
perlipidemic drugs with different mechanisms
aloe leaf preparations [13]. For example, aloe gel
are often needed for effective treatment of hyper-
lowered the blood triglycerides level in a mouse
lipidemic type 2 diabetic patients [4, 5]. Conven-
model of T2DM [15]. Further, aloe gel reduced
tional anti-hyperglycemic and anti-hyperlipi-
the blood cholesterol, triglycerides, LDL and VLDL
demic drugs have limited efficacies and impor-
levels, but increased the blood HDL level in strep-
Culture and Research (ACECR)Kavosh Boulevard, Supa
tant adverse effects. Thus, more efficacious and
tozocin-induced diabetic rats [16]. A controlled
safer anti-hyperglycemic and anti-hyperlipidemic
clinical trial (n = 60) indicated decreased blood to-
agents are needed [6, 7]. Plants have played a sig-
tal cholesterol, triglycerides, and LDL levels after
nificant role in maintaining human health and
12 weeks of two different doses of aloe gel in two
improving the quality of life for thousands of
groups of hyperlipidemic patients compared with
years [8]. Herbal supplements may be effective in
baseline. Since this trial was available as an ab-
Fax: + 98 26 14 76 40 [email protected]
prevention and treatment of diseases [9–11]. Cur-
stract only, neither intergroup comparisons nor
Huseini HF et al. Anti-hyperglycemic and Anti-hypercholesterolemic … Planta Med 2012; 78: 311–316
randomization nor blinding were mentioned [17]. Reports on the
for different concentrations of acemannan applied. 10 µL of each
effects of aloe in the animal models of diabetes have been incon-
of the sample solutions was spotted in triplicate on HPTLC plates.
sistent [18–22]. Two nonrandomized clinical trials (n = 76 and
Chromatograms were developed, scanned, and the peak areas re-
n = 40) are available from the same investigation group that re-
corded. The amount of acemannan in the sample was calculated
ported decreased fasting blood glucose and triglycerides levels,
by the calibration curve of acemannan.
but no change in the cholesterol level after 6 weeks of juice madefrom aloe gel in type 2 diabetic patients. The blood lipid levels
Preparation of the aloe gel powder and placebo capsules
were not the primary outcomes in the trials [21, 23]. Case reports
The aloe gel powder as the drug and toast powder as the placebo
of five type 2 diabetic individuals reported decreases in fasting
were separately filled into oral gelatin capsules with identical ap-
blood glucose and glycosylated hemoglobin (HbA1c) levels [18].
pearance by using a hand-operated capsule-filling machine (Sci-
No adverse effects were reported in these trials [17, 18, 21, 23].
entific Instruments and Technology Corporation). The aloe cap-
The trials had methodological drawbacks such as lack of random-
sules contained 300 mg of the aloe gel powder. Toast powder
ization, lack of double-blindness, small sample size, and lack of
was chosen as the placebo, because its appearance was relatively
power calculation [13, 14]. The preliminary data suggest a poten-
tial effect of aloe in glycemic control and hyperlipidemia; howev-er, further information is needed [13, 14].
In conclusion, further and better trials are needed to define the
Inclusion criteria: Iranian male and female type 2 diabetic outpa-
clinical efficacy and safety of aloe in the treatment of diabetes
tients aged 40 to 60 years; patients with fasting blood levels of
mellitus and hyperlipidemia more precisely. Thus, the efficacy
glucose between 150 mg/dL to 200 mg/dL and HbA1c between
and safety of aloe gel in the treatment of hyperlipidemic (hyper-
7 % to 9 % despite taking two 5 mg glyburide tablets and two
cholesterolemic and/or hypertriglyceridemic) type 2 diabetic pa-
500 mg metformin tablets every day; patients using two 5 mg
tients were evaluated and compared with placebo in the study
glyburide tablets and two 500 mg metformin tablets every day;
newly diagnosed patients with fasting blood LDL and/or triglyc-erides levels above 100 mg/dL and 150 mg/dL, respectively. Exclusion criteria: Patients taking other anti-hyperglycemic and
anti-hyperlipidemic agents; patients receiving insulin therapy;
patients with cardiac, renal, hepatic, hematological diseases, hy-
Aloe and preparation of the aloe leaf gel powder
pothyroidism, tachycardia, vertigo, and seizure; patients with a
The freshly harvested whole aloe leaves obtained from the Re-
history of gallstones or gall bladder surgery; patients using estro-
search Institute of Medicinal Plants (Karaj, Iran) were washed in
gen, steroid, beta-blocker, and thiazide; pregnant women; wom-
a suitable bactericide (chlorhexidine). 1 inch of the leaf base, 2 in-
en planning pregnancy; breast-feeding women.
ches of the tapering point, and sharp spines located along the leafmargins were removed by a knife. The skin was carefully sepa-
rated from the parenchyma. The filets were extensively washed
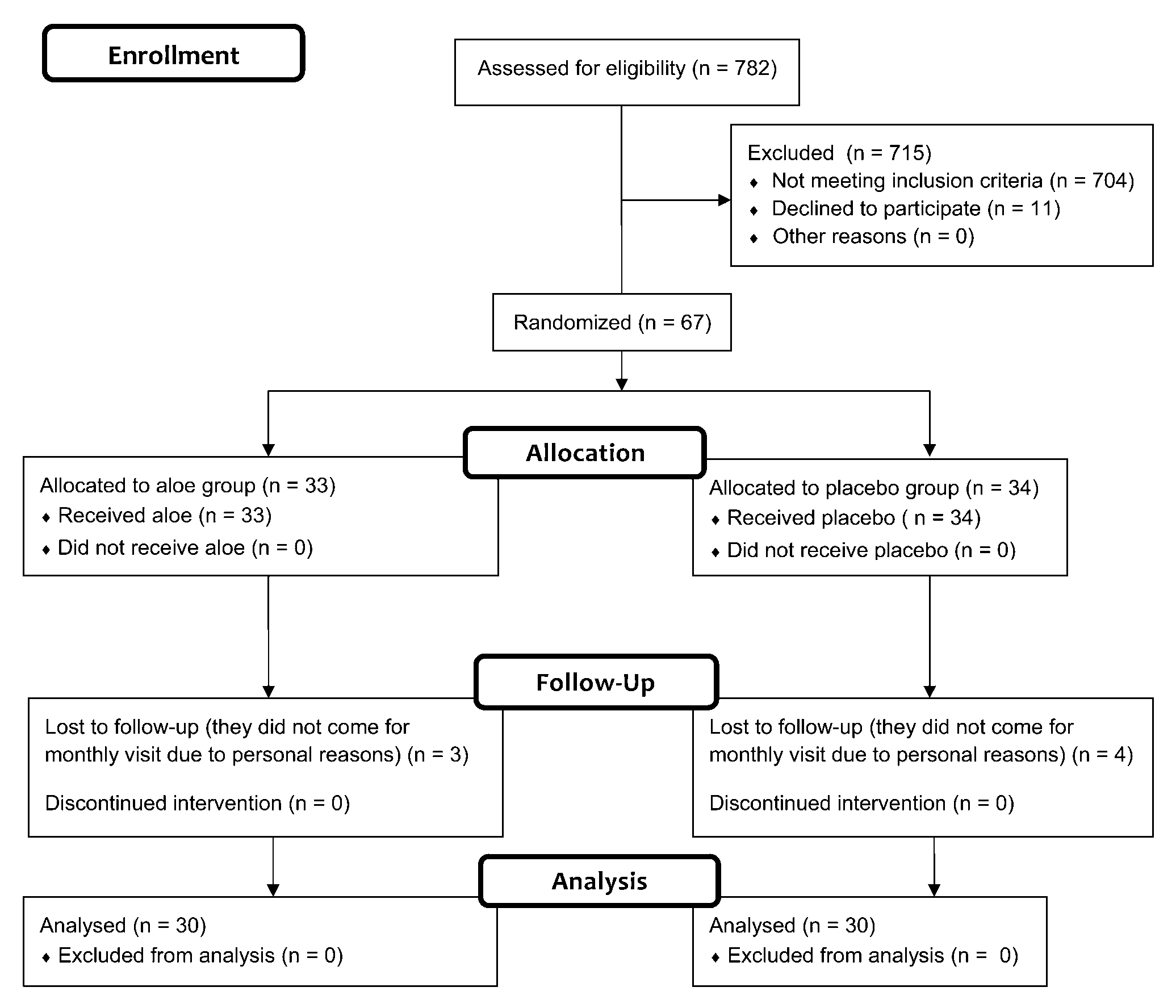
Sixty-seven Iranian male and female outpatients (thirty-three
with distilled water to remove the exudates from their surfaces,
patients in the aloe group and thirty-four patients in the placebo
then the filets were ground to a liquid, and the pulp was removed
group) were recruited according to the inclusion and exclusion
by filtering. The gel obtained was treated with activated carbon
criteria. Thirty patients in each group finished the trial which
to decolorize the gel and remove aloin and anthraquinones,
was the sample size calculated to estimate 25 mg/dL difference
which have laxative effects. The resultant gel was then freeze-
of total cholesterol between the groups, considering type I er-
dried so that a pure powder was produced [24].
ror = 0.05 and 80 % power. The CONSORT flowchart describing
Downloaded by: Tel Aviv University. Copyrighted material.
the progress of the patients through the trial is shown in
Determination of the acemannan content of the gel
l" Fig. 1. The demographic data of the subjects who finished the
The acemannan content of the gel powder was analyzed by
A group of thirty patients took the aloe capsules at the dose of
HPTLC according to the method described previously [25]. A
one 300 mg capsule every 12 hours by the oral route for 2
stock solution of acemannan (1000 mg/mL) was prepared in
months, and another concurrently parallel group of thirty pa-
water. Different concentrations of the stock solution (10, 20, 40,
tients took the placebo capsules orally every 12 hours for 2
and 80 mg/mL) were obtained by water dilution. 10 µL of each of
months. The dosage of the aloe gel was based on the results of a
them were spotted in triplicate on TLC plates so as to obtain con-
dose finding study. Block randomization was used for treatment
centrations of 100, 200, 400, and 800 ng per spot of acemannan,
allocation. The study was double-blind. Further, the patients
were recommended to restrict intake of carbohydrates and fatty
The data of peak areas versus acemannan masses were treated by
foods such as rice, confectionery, red meat, pies, cream pies, eggs,
the linear least square regression method. 1 mg of aloe powder
and fatty dairy products from two months before the beginning
dissolved in 10 mL of water was used for quantification of ace-
of the trial onward. All the subjects recorded the names and
mannan. 10 µL of each of the concentrations of standard solu-
amounts of the daily consumed foods for 3 days every week. To
tions were spotted in triplicate on HPTLC plates. Chromatograms
monitor the patientsʼ compliance with the allocated treatments,
were developed for 10 cm using n-butanol: n-propanol: glacial
the patients returned any capsules left and were asked questions
acetic acid: water (30: 15: 10: 5 v/v/v/v). After development, the
about taking the capsules on their monthly visit. The treatment,
plates were sprayed with anisaldehyde sulfuric acid reagent, and
diet, and physical activity of the patients completing the trial re-
the spots were detected by heating the plate at 105–110 °C for
mained unchanged throughout the study. At the beginning and
3 min. The sprayed plates were scanned at 600 nm. The calibra-
also the end of the study, the fasting (after fasting for 12 hours)
tion curve of acemannan was obtained by plotting peak areas
blood levels of glucose, HbA1c, creatinine, BUN (blood urea nitro-
Huseini HF et al. Anti-hyperglycemic and Anti-hypercholesterolemic … Planta Med 2012; 78: 311–316
The CONSORT flowchart describing the progress of the patients through the trial.
Downloaded by: Tel Aviv University. Copyrighted material.
gen), AST (aspartate aminotransferase), ALT (alanine aminotrans-
istered in the Iranian Registry of Clinical Trials with the number
ferase), AP (alkaline phosphatase), GGT (γ-glutamyl transpepti-
dase); total, direct, and indirect bilirubins; triglycerides, totalcholesterol, VLDL, LDL, and HDL in the aloe and placebo groupswere determined with standard enzymatic kits produced by the
Pars Azmoon company and an auto analyzer (Hitachi 902). The
glucose, HbA1c, and lipid levels were the primary outcome varia-
Linearity was shown for acemannan between 100 and 800 ng/
bles. The other blood parameter levels were the secondary out-
spot by 4 different concentrations of the acemannan standard.
come variables. The baseline homogeneity of the blood parame-
The equation y = 1.943 x + 7.103 (R2 = 0.999) with the applied ace-
ter means across the aloe and placebo groups was analyzed by
mannan mass x and the area y was obtained (l
the Mann-Whitney U test, and p values below 0.05 were consid-
of acemannan was determined in the gel powder.
ered as significant. At the end of the study, the data of the pa-
No adverse effects were reported. The groups were matched in
tients in the aloe and placebo groups were also compared by the
regard to demographic data (age, gender, duration of diabetes,
Mann-Whitney U test and p values below 0.05 were considered
" Table 1). The baseline blood levels of
as significant. All statistical analyses were per-protocol analyses.
all parameters were not significantly different between the two
All participants were requested to report any adverse effects.
Written informed consent was obtained from the patients. The
The aloe gel lowered the glucose, HbA1c, total cholesterol, and
medical ethics committee of the Ebne Sina Research Institute af-
LDL levels significantly (p = 0.036, p = 0.036, p = 0.006, and
filiated with the ACECR approved the protocol (approval number
p = 0.004, respectively) without any significant effects on the oth-
and date: 492/51/29 and 23 Nov. 2008). Further, the trial was reg-
er parameter levels (p > 0.05) compared with the placebo group
Huseini HF et al. Anti-hyperglycemic and Anti-hypercholesterolemic … Planta Med 2012; 78: 311–316
the subjects who finished the trial.
The fasting blood parameter levels before and after intervention and their changes during the study.
Downloaded by: Tel Aviv University. Copyrighted material.
a P < 0.05, significant (Mann-Whitney U test); SD, standard deviation; ↓ decrease; ↑ increase
" Table 2). The percentages of endpoint reduc-
tions of the glucose, HbA1c, total cholesterol, and LDL levels in
the aloe group compared with the baseline levels were 4.8 %,
The results suggest that aloe gel improves glycemic control and
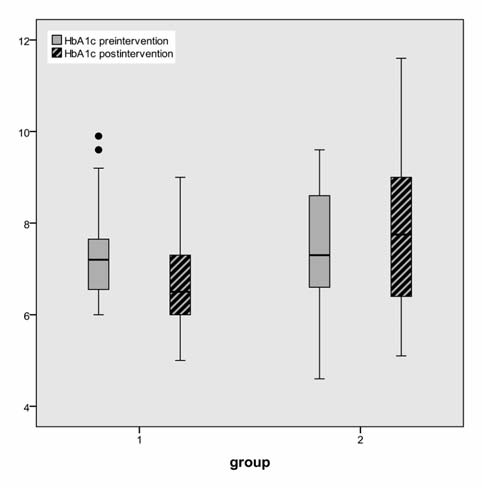
8.07 %, 8.35 %, and 4.48 %, respectively. The box plots of decreases
lowers the blood levels of total cholesterol and LDL, but does not
(before intervention – after intervention) in the glucose, HbA1c,
affect the other blood lipid levels and does not cause any hepatic,
total cholesterol, and LDL levels of the aloe and placebo groups
renal, or other adverse effects in the hyperlipidemic type 2 dia-
betic patients. The improved glycemic control agrees with theprevious trials [18, 21, 23]. However, the effects on the lipid pro-file have some discrepancies with the earlier trials [17, 21, 23].
Huseini HF et al. Anti-hyperglycemic and Anti-hypercholesterolemic … Planta Med 2012; 78: 311–316
Box plot of decreases (before intervention – after intervention) in
Box plot of decreases (before intervention – after intervention) in
the fasting blood glucose (FBG) levels (mg/dL) of the aloe (group 1) and
the blood glycosylated hemoglobin (HbA1c) levels (percent) of the aloe
(group 1) and placebo (group 2) groups.
Downloaded by: Tel Aviv University. Copyrighted material.
Box plot of decreases (before intervention – after intervention) in
Box plot of decreases (before intervention – after intervention) in
the blood total cholesterol levels (mg/dL) of the aloe (group 1) and placebo
the blood low-density lipoprotein (LDL) levels (mg/dL) of the aloe (group 1)
The total cholesterol and LDL lowering effects of the aloe gel in
vious studies reporting the triglycerides lowering effect of aloe
the present trial agree with the previous study reporting the total
gel [17, 21, 23]. The lack of the aloe gel effects on the triglyceride
cholesterol and LDL lowering effect of aloe gel [17] but disagree
and HDL levels in the present trial could be due to the small num-
with the earlier reports showing no effect of aloe gel on the cho-
lesterol level [21, 23]. Further, the lack of the aloe gel effect on the
The only bioactive that was identified and quantified in the aloe
triglycerides level in the current trial is inconsistent with the pre-
gel used in the present trial was a mucopolysaccharide named
Huseini HF et al. Anti-hyperglycemic and Anti-hypercholesterolemic … Planta Med 2012; 78: 311–316
acemannan. Further, the bioactives and mechanisms involved in
9 Fugh-Berman A. Herbs and dietary supplements in the prevention and
the anti-hyperglycemic and anti-hypercholesterolemic actions of
treatment of cardiovascular disease. Prev Cardiol 2000; 3: 24–32
10 Tapsell LC, Hemphill I, Cobiac L, Patch CS, Sullivan DR, Fenech M, Roo-
the aloe gel were not investigated in the study presented here.
denrys S, Keogh JB, Clifton PM, Williams PG, Fazio VA, Inge KE. Health
Very few studies have been conducted on the characterization of
benefits of herbs and spices: the past, the present, the future. Med
the bioactives and mechanisms mediating the anti-hyperglyce-
mic action of the aloe gel. Trace elements present in the gel and
11 Low Dog T. A reason to season: the therapeutic benefits of spices and
culinary herbs. Explore 2006; 2: 446–449
five phytosterols isolated from the gel were responsible for the
12 Tundis R, Loizzo MR, Menichini F. Natural products as alpha-amylase
anti-hyperglycemic effects of the gel in the streptozocin-induced
and alpha-glucosidase inhibitors and their hypoglycemic potential in
diabetic rats and a mouse model of T2DM, respectively [26, 27].
the treatment of diabetes: an update. Mini Rev Med Chem 2010; 10:
Also, aloe gel appeared to decrease insulin resistance in two
mouse models of T2DM [15, 28]. It is notable that the bioactives
13 Vogler BK. Aloe vera: a systematic review of its clinical effectiveness. Br
and mechanisms underlying the effects of aloe gel on the lipid
14 Yeh GY, Eisenberg DM, Kaptchuk TJ, Phillips RS. Systematic review of
profile have not been studied so far. Finally, considering the re-
herbs and dietary supplements for glycemic control in diabetes. Diabet
sults of the present and previous trials, further and larger clinical
trials concerning the efficacy and safety of aloe gel in the treat-
15 Kim K, Kim H, Kwon J, Lee S, Kong H, Im SA, Lee YH, Lee YR, Oh ST, Jo TH,
ment of patients with T2DM and/or hyperlipidemia as well as
Park YI, Lee CK, Kim K. Hypoglycemic and hypolipidemic effects of pro-cessed Aloe vera gel in a mouse model of non-insulin-dependent dia-
more studies addressing the bioactives and mechanisms involved
betes mellitus. Phytomedicine 2009; 16: 856–863
in the effects of aloe gel on the blood glucose and lipid levels
16 Rajasekaran S, Ravi K, Sivagnanam K, Subramanian S. Beneficial effects
of Aloe vera leaf gel extract on lipid profile status in rats with strepto-zocin diabetes. Clin Exp Pharmacol Physiol 2006; 33: 232–237
17 Nassiff HA, Fajardo F, Velez F. Effecto del aloe sobre la hiperlipidemia en
pacientes refractarios a la dieta. Rev Cuba Med Gen Integr 1993; 9: 43–
18 Ghannam N, Kingston M, Al-Meshaal IA, Tariq M, Parman NS, Wood-
We are grateful to the ACECR and its affiliated Research Institute
house N. The antidiabetic activity of aloes: preliminary clinical and ex-
of Medicinal Plants for sponsoring this study.
perimental observations. Horm Res 1986; 24: 288–294
19 Ajabnoor MA. Effect of aloes on blood glucose levels in normal and al-
loxan diabetic mice. J Ethnopharmacol 1990; 28: 215–220
20 Koo ML. Aloe vera: antiulcer and antidiabetic effects. Phytother Res
21 Yongchaiyudha S, Rungpitarangsi V, Bunyapraphatsara N, Chokechaijar-
The authors do not have any financial/commercial conflicts of in-
oenporn O. Antidiabetic activity of Aloe vera L. juice. I. Clinical trial innew cases of diabetes mellitus. Phytomedicine 1996; 3: 241–243
22 Oykar A, Can A, Akev N, Baktir G, Sutlupinar N. Effect of Aloe vera leaves
on blood glucose level in type I and type II diabetic rat models. Phy-
1 Campbell RK. Type 2 diabetes: where we are today: an overview of dis-
23 Bunyapraphatsara N, Yongchaiyudha S, Rungpitarangsi V, Chokechaijar-
ease burden, current treatments, and treatment strategies. J Am Pharm
oenporn O. Antidiabetic activity of Aloe vera L. juice. II. Clinical trial in
diabetes mellitus patients in combination with glibenclamide. Phyto-
2 Mudaliar S. New frontiers in the management of type 2 diabetes. Indi-
24 Ramachandra CT, Srinivasa Rao P. Processing of Aloe vera leaf gel: a re-
3 Tomkin GH. Targets for intervention in dyslipidemia in diabetes. Diabe-
view. Am J Agric Biol Sci 2008; 3: 502–510
25 Lobo R, Prabhu KS, Shirwaikar A, Ballal M, Balachandran C, Shirwaikar
4 Derosa G, Sibilla S. Optimizing combination treatment in the manage-
A. A HPTLC densitometric method for the determination of aloeverose
Downloaded by: Tel Aviv University. Copyrighted material.
ment of type 2 diabetes. Vasc Health Risk Manag 2007; 3: 665–671
in Aloe vera gel. Fitoterapia 2010; 81: 231–233
5 Spratt KA. Managing diabetic dyslipidemia: aggressive approach. J Am
26 Rajasekaran S, Sivagnanam K, Subramanian S. Mineral contents of Aloe
vera leaf gel and their role on streptozocin-induced diabetic rats. Biol
6 Davidson MH, Toth PP. Comparative effects of lipid-lowering therapies.
27 Tanaka M, Misawa E, Ito Y, Habara N, Nomaquchi K, Yamada M, Toida T,
7 Krentz AJ, Bailey CJ. Oral antidiabetic agents: current role in type 2 dia-
Hayasawa H, Takase M, Inagaki M, Hiquchi R. Identification of five phy-
betes mellitus. Drugs 2005; 65: 385–411
tosterols from Aloe vera gel as anti-diabetic compounds. Biol Pharm
8 Huang THW, Kota BP, Razmovski V, Roufogalis BD. Herbal or natural
medicines as modulators of peroxisome proliferator-activated recep-
28 Perez YY, Jimenez-Ferrer E, Zamilpa A, Hernandez-Valencia M, Alarcon-
tors and related nuclear receptors for therapy of metabolic syndrome.
Aquilar FJ, Tortoriello J, Roman-Ramos R. Effect of a polyphenol-rich ex-
Basic Clin Pharmacol Toxicol 2005; 96: 3–14
tract from Aloe vera gel on experimentally induced insulin resistancein mice. Am J Chin Med 2007; 35: 1037–1046
Huseini HF et al. Anti-hyperglycemic and Anti-hypercholesterolemic … Planta Med 2012; 78: 311–316
MUSIQUE MUNICIPALE DE PLAN-LES-OUATES ECOLE DE MUSIQUE BULLETIN D’INSCRIPTION Année scolaire 2011 / 2012 Je soussigné inscris mon enfant comme élève. ………………………. Prénom : ………………………. …………………………………………………… No :…………………………………………………………………………………�
 The CONSORT flowchart describing the progress of the patients through the trial.
The CONSORT flowchart describing the progress of the patients through the trial.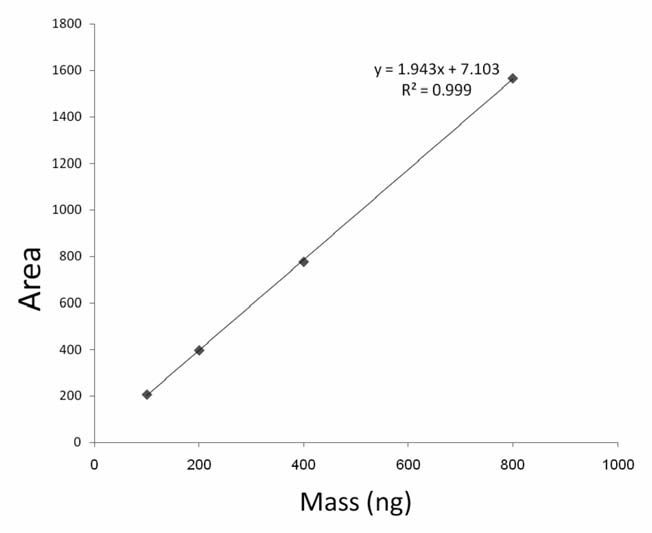 the subjects who finished the trial.
the subjects who finished the trial.

 Box plot of decreases (before intervention – after intervention) in
Box plot of decreases (before intervention – after intervention) in
the fasting blood glucose (FBG) levels (mg/dL) of the aloe (group 1) and
the blood glycosylated hemoglobin (HbA1c) levels (percent) of the aloe
(group 1) and placebo (group 2) groups.
Box plot of decreases (before intervention – after intervention) in
Box plot of decreases (before intervention – after intervention) in
the fasting blood glucose (FBG) levels (mg/dL) of the aloe (group 1) and
the blood glycosylated hemoglobin (HbA1c) levels (percent) of the aloe
(group 1) and placebo (group 2) groups.