Randomized controlled study of 3 different types of hemoclipsfor hemostasis of bleeding canine acute gastric ulcers
Dennis M. Jensen, MD, Gustavo A. Machicado, MD, Ken Hirabayashi, BA
Background: Mechanical closure of bleeding vessels is clinically appealing, and several types of hemoclips arenow marketed for endoscopic hemostasis of nonvariceal lesions. No comparative data have been reported onease of clip placement, hemostasis efficacy, or clip retention rates on bleeding ulcers.
Objective: To compare 3 different types of hemoclips for hemostasis of bleeding ulcers.
Design: Randomized controlled study.
Subjects: Seven adult dogs with prehepatic portal hypertension were heparinized, and acute gastric ulcers weremade with jumbo biopsy forceps. Animals had oral proton pump inhibitors daily and weekly endoscopies toquantitate clip retention and ulcer healing.
Interventions: Bleeding ulcers were randomized in pairs (2 for each treatment/dog) to endoscopic hemocliptreatment or control.
Main Outcome Measurements: Initial times and success of deployment, hemostasis efficacy, clip retentionrates, and ulcer healing during endoscopic follow-ups.
Results: There was no difference in initial hemostasis rates of hemoclips, and no major complications occurred. Ulcer healing times were faster (Resolution Clip [RC] or TriClip [TC]) or similar (QuickClip2 [QC]) to con-trols. Clip retention at 1 week was significantly less with TC and, at 3 to 7 weeks, was significantly higherwith RC.
Conclusions: (1) For the 3 hemoclip devices, initial hemostasis rates were 100%, but all devices required similarlearning time to place clips successfully. (2) Short-term retention rates of TC were significantly less than QC orRC. (3) Long-term clip retention was significantly higher with RC. (4) All 3 hemoclips were safe, and none inter-fered with ulcer healing. (Gastrointest Endosc 2006;64:768-73.)
A fundamental procedure of general surgery is mechan-
throughout the GI tract, which is now accessible to
ical ligation of bleeding arteries. Successfully performing
various types of endoscopes, and this type of mechanical
this endoscopically could be a major advantage for
hemostasis is very clinically appealing.
endoscopic hemostasis of bleeding nonvariceal lesions,
There are several clinical nonrandomized and random-
such as ulcers that have exposed arteries or arterioles as
ized reports of hemoclips for hemostasis in the upper-GI
the source of hemorrhage.If the hemoclips remain on
tract, with variable results. Hemoclip devices have under-
the vessel through the usual period of ulcer recurrent
gone redesign and improvements to facilitate their
bleeding, until complete ulcer healing (eg, re-epithelializa-
deployment and clinical use. Several companies now mar-
tion), and if no complications occur, permanent hemosta-
ket hemoclips for clinical applications. However, no data
sis of bleeding ulcers or other lesions could be achieved
have been reported that compare various clinically
with hemoclips Bleeding nonvariceal lesions occur
marketed hemoclips in terms of ease of clip placement,hemostasis efficacy, clip retention rates, or other com-parative outcomes.
Our purposes in this study were to (1) compare the
Copyright ª 2006 by the American Society for Gastrointestinal Endoscopy
initial time and success for deployment of 3 different types
0016-5107/$32.00doi:10.1016/j.gie.2006.06.031
of hemoclips, (2) compare the efficacy and the safety for
768 GASTROINTESTINAL ENDOSCOPY Volume 64, No. 5 : 2006
Study of 3 hemoclips for hemostasis of acute ulcers
hemostasis of bleeding acute gastric ulcers, and (3) quan-titate hemoclip retention rates and ulcer healing during
Although several types of hemoclips are available forendoscopic hemostasis of nonvariceal lesions, no
Before starting this comparative study, the 2 endoscop-
comparative data have been reported on ease of
ists (D.M.J. and G.A.M.) learned, in a separate pilot study,
placement, efficacy, or retention rates.
how to successfully deploy each type of hemoclip. This
was first done on a laboratory bench top on tissue modelsand then endoscopically in dogs. Approximately 8 hemo-
In a randomized controlled trial of 3 types of hemoclips
clips of each type were used; 5 to 6 hemoclips (of each
in 7 dogs, hemostasis rates were 100%, all devices
kind) were successfully placed endoscopically in other
required similar learning time for successful placement,
dogs, before this study was initiated.
and none interfered with ulcer healing.
Short-term retention rates of the TC were significantly
For this randomized, prospective study, 7 adult dogs,
lower than with the QC or the RC, but long-term
each weighing approximately 22.7 to 27.2 kg (50-60 lb),
retention was significantly higher with the RC hemoclip.
with prehepatic portal hypertension, were used. After pre-medication, intubation, and isoflurane anesthesia, intrave-nous heparin was administered (1000 units/4.5 kg body
40 mg before meals [AstraZeneca Pharmaceuticals LP, Wil-
weight) for anticoagulation, as previously descAn
mington, Del]). All animals had clinical evaluations (twice
endoscopic examination of the stomach was performed
weekly) to check for potential complications and under-
by using a Pentax therapeutic videoendoscope (Pentax,
went weekly endoscopies to evaluate end points, clip re-
Orangeburg, NY), with a large channel (3.7-mm diameter)
tention, and ulcer healing. Long-term treatment end
and separate water-jet irrigation. Acute gastric ulcers were
points included (1) clip retention rates on weekly fol-
created in the antrum and the body of the stomach with
low-up endoscopies, (2) complete ulcer healing (eg, re-
a large (3.2- to 8-mm diameter open jaws) jumbo biopsy
epithelialization), and (3) clinical evidence of recurrent
forceps (Boston Scientific Corp, Marlborough, Mass), as
bleeding (and stigmata of ulcer bleeding) or complications
previously described.In brief, the ulcers were created
of endoscopy or treatments (perforation, vomiting, inter-
in pairs (3-4 cm apart), starting in the antrum, were ran-
domized, and were treated. Proximally, within 4 to 5 cm,
For statistical comparisons at the end of the study, the
the next pair of ulcers was made, randomized, and treated
time-to-event outcomes (eg, time to successfully place 2
with a different treatment. In all, 4 pairs of ulcers (8 ulcers/
hemoclips, time to ulcer healing, duration of hemoclip re-
animal) in a linear array distal to proximal resulted. These
tention) were compared by log-rank tests. Proportions
were mapped as distance from the pylorus and the inci-
(eg, failures of hemoclip placement, success of initial he-
sors, which facilitated identification on the weekly fol-
mostasis, and hemoclip retention at 1-5 weeks) were com-
pared by c2 tests. A P value of less than .05 was considered
These resultant acute bleeding ulcers were randomized
in pairs (2 for each treatment/dog or 8 ulcers total/animal)by using sealed envelopes with treatment designations,created by random numbers tables for 7 dogs. The ran-
domization was to 1 of 3 endoscopic hemoclip treatments:QuickClip2 (QC) (standard size 8 mm open; Olympus
From the pilot study, the investigators observed that
America Inc, Central Valley, Pa); TriClip (TC) (3 prongs in
there was a short learning curve for each type of hemoclip.
a tripod configuration, 8 mm open between prongs;
Although familiarity with hemoclips was helpful, it did not
Cook Endoscopy, Winston-Salem, NC); or Resolution Clip
equate with hands-on experience or successful endoscopic
(RC) (size, 12 mm open; Microvasive); or control (no en-
deployment of different types of hemoclips. Because of the
doscopic treatment). For the ulcers randomized to hemo-
different characteristics of hemoclips, as summarized in
clips, we required 2 hemoclips per ulcer to be successfully
especially in the deployment mechanisms, the GI
placed and complete hemostasis to occur. The acute treat-
endoscopist and his assistant had to learn how to success-
ment end points quantitated were (1) acute hemostasis,
fully deploy each type of clip. Approximately 8 hemoclips
complete control of acute ulcer bleeding; (2) time to suc-
of each type were used for practice and deployment (5-6
cessfully place 2 hemoclips on the bleeding ulcer; (3) fail-
clips endoscopically) before successful endoscopic place-
ure of initial clip placement; and (4) ability to appose the
ment was assured by our team of investigators.
There were some differences observed in the pilot
The animals were subsequently treated with oral pro-
study for hemoclips or their deployment, which probably
ton pump inhibitors (PPI) once daily (esomeprazole
influenced results in this study ). A major
Volume 64, No. 5 : 2006 GASTROINTESTINAL ENDOSCOPY 769
Study of 3 hemoclips for hemostasis of acute ulcers
There were no major complications (such as perfora-
TABLE 1. Comparison of Olympus, Cook Endoscopy,
tions, recurrent bleeding, vomiting, or weight loss). All
and Microvasive endoscopic hemoclips (results
the hemoclips passed spontaneously. They did not inter-
fere with ulcer healing or any animal’s eating frequencyor pattern of eating.
Endoscopically deployable hemoclips were initially de-
veloped in Japan by Kuramata et aland Hayashi et al,
more than 30 years ago. The early Olympus hemoclips
could not be rotated, so that access to some bleeding ulcerswas not possible, and deployment was often difficult, espe-
cially in emergency Over the last 3 decades, Olym-
pus hemoclips have undergone significant technologic
improvements, including development of many sizes andshapes of clips, which were reloadable.Now, QCs are
marketed in the United States as preloaded and single-use clips that can be rotated to improve deploymentupon GI lesions.Also now, other endoscopy devicecompanies have designed and marketed other types of
advantage of the RC hemoclip appeared to be the grasp-
and-release mechanism, which allowed grasping, releas-
The results of our pilot study emphasized that each of
ing, and repositioning of the hemoclip before actual clip
the hemoclipping devices is unique in size, shape, deploy-
deployment. The TC and the QC did not have this feature,
ment characteristics, ability to grasp and release bleeding
and, once grasped or closed, these clips could not be
lesions, and ability to partially rotate the hemoclips before
opened and repositioned; they were lost or misplaced
placement (see Because of these differences,
on the sides of acute ulcers. The TC 3-prong clip was
practice before clinical emergency use of hemoclips (of
more difficult to place tangentially than the RC or the
different types) is necessary, in our opinion. There was
QC, and, because of its narrow-wire prongs, often the
a short but definite learning curve for successful deploy-
TC device sliced through the edges of acute ulcers. Among
ment of each type of endoscopic hemoclipping device.
the 3 hemoclip types, rotation capability was best with the
In our studies, this was accomplished before initiation of
QC on the bench top but not by endoscopy (see below).
the comparative study, with laboratory bench top hemo-
The RC was larger (when open) than the TC or the QC,
clipping of tissue, followed by successful endoscopic de-
and the RC hemoclip grasped more tissue.
ployment. Such training should be strongly considered
The mean time required to place 2 hemoclips on the
for the GI endoscopist, as well as for the GI technicians
bleeding ulcers was similar for all 3 hemoclips ).
who will be assisting the endoscopist, if neither is familiar
Failure rates (of deployment onto the bleeding ulcer)
with the types of hemoclips to be used.
were similar with the QC (12.9%), the TC (6.9%), and
Clinical studies, whether case series or comparative
the RC (9.1%). In contrast, acute hemostasis rates were
studies, are only reported with Olympus hemoclips. For
100% for all hemoclipped ulcers, compared with 0% for
example, Lai et reported successful hemostasis in
control (not endoscopically treated) ulcers (P ! .05).
95% of 40 patients who presented with ulcer bleeding. Re-
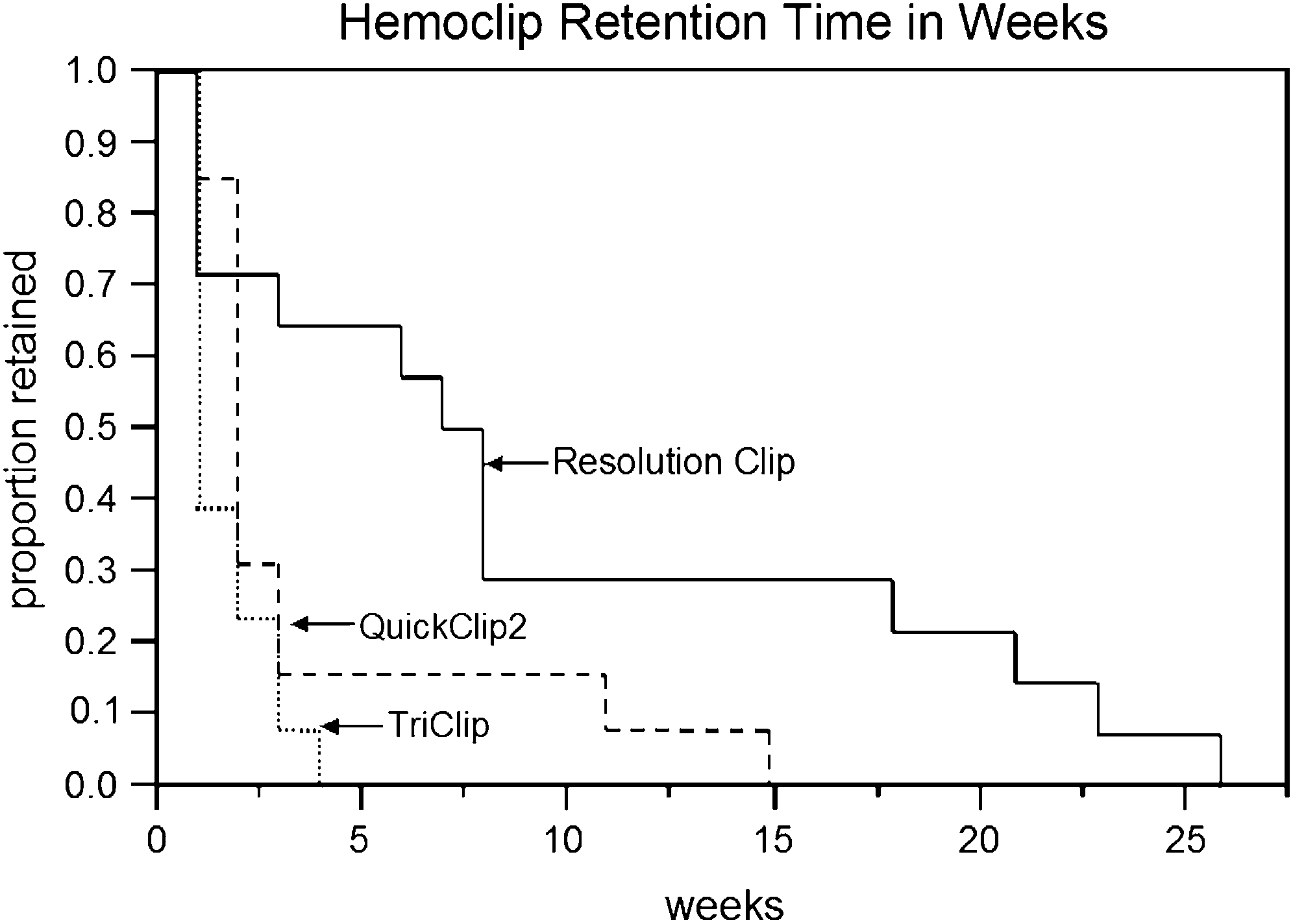
Long-term clip retention was significantly higher with
current bleeding rates were slightly higher in spurting
the RC compared with the other 2 types of hemoclips.
ulcers (15%) than with oozing ulcers (4%). They were
The median clip retention times for 1 or more clips to still
not able to place the clips in 2 patients (5%) because of
be on the ulcer and the interquartile ranges [IQR] were
technical difficulties. In contrast, Villanueva et alre-
for TC, 1 week (IQR, 1-2); for QC, 2 weeks (IQR, 2-3);
ported that Olympus hemoclips could not be placed in
and for RC, 8 weeks (IQR, 1-18). The product-limit curves
about 19% of patients with bleeding chronic peptic ulcers.
The majority of these patients had chronic ulcers with fi-
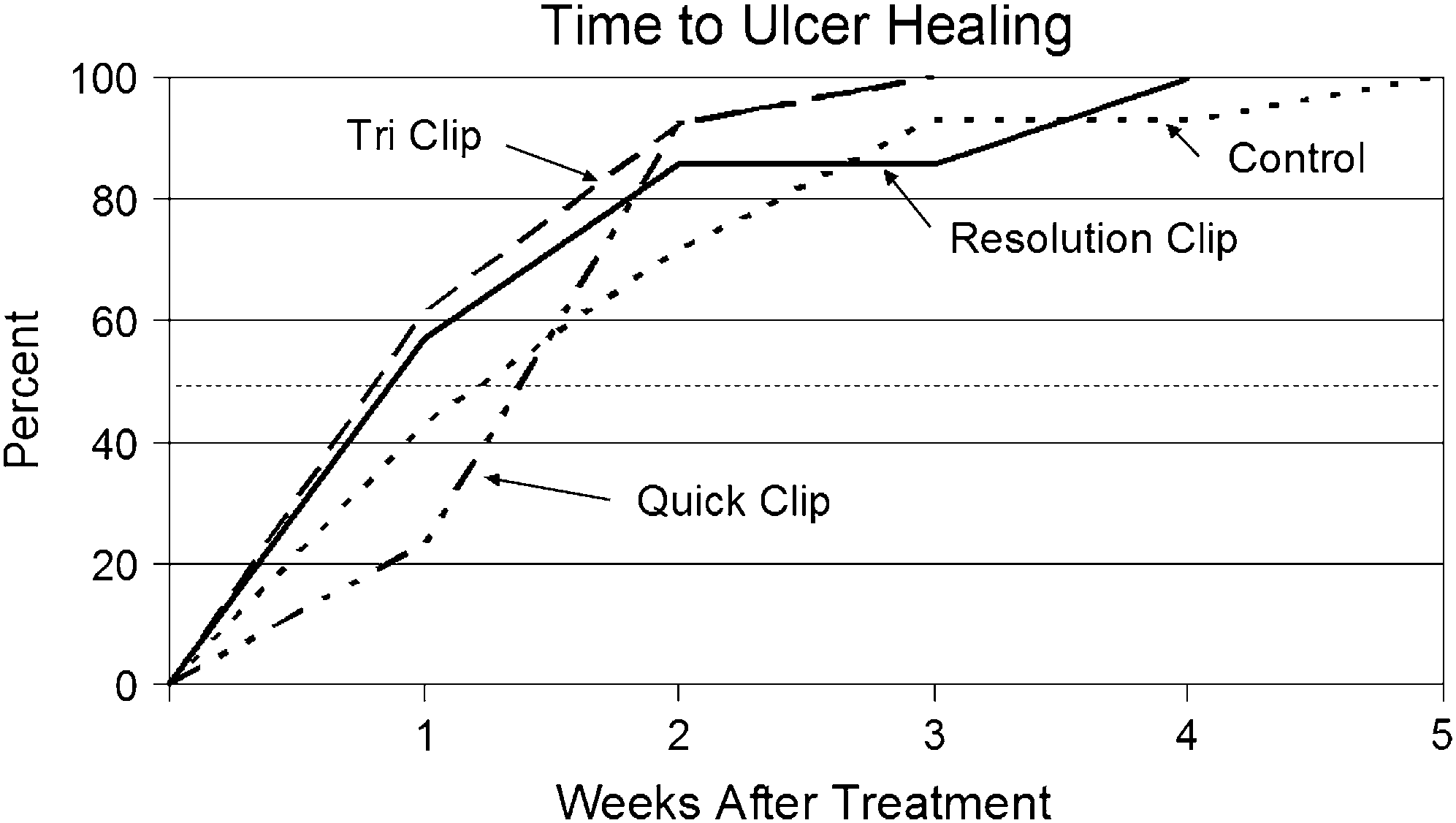
By log-rank tests, there were no significant differences
brotic bases, and the Olympus hemoclip would not ad-
in time to ulcer healing of hemoclip-treated ulcers or con-
here to the ulcer base or the stigmata.
trols. Specifically, the median times to healing and IQR
Investigators who compared ethanol injectioor
ranges of the TC and the RC ulcers were 1 week (IQR,
epinephrine injectionwith Olympus hemoclip for hemo-
1-2), for QC ulcers were 2 weeks (IQR, 2-2), and controls
stasis of upper-GI nonvariceal lesions (predominantly
peptic ulcers) have reported significantly higher recurrent
770 GASTROINTESTINAL ENDOSCOPY Volume 64, No. 5 : 2006
Study of 3 hemoclips for hemostasis of acute ulcers
TABLE 2. Results acutely and during follow-up weekly endoscopies
Hemoclip retention/no. successfully placed (%)
Mean time for Successful hemostasis/ Acute hemoclipping failure/
*P ! .05 vs other treatments.
Figure 2. The time to ulcer healing. Shown are the proportion of ulcershealed on weekly follow-up endoscopies, grouped according to initial he-moclip treatments or control. For each, 13 to 14 ulcers were randomized,and animals took daily esomeprazole (40 mg/d) until all ulcers healed.
Figure 1. Product-limit curves for proportion of hemoclips retained, de-
The dotted horizontal line indicates median time to ulcer healing, which
fined as 1 or more clips retained per ulcer. Two hemoclips had been suc-
was not significantly different for the treatment groups or control.
cessfully placed on each ulcer (N Z 13-14 per treatment group) duringhemostasis. All hemoclips were eventually lost in all ulcers, and therewas no censoring of data. The overall log rank test had P ! .0014. Pair-wise comparisons were RC vs QC, P Z .046, RC vs TC, P Z .004, and
was uniformly successful. In our experience, these dispa-
rate results probably relate to practice with and standard-ization of endoscopic techniques before initiation ofclinical randomized studies.Also, this may relate to
bleeding rates in the injection groups compared with the
a learning curve problem, as we experienced in our pilot
hemoclip group. In another randomized controlled trial
study with this hemoclip study. Saltzman et alrecently
that compared hemoclip with injection of distilled water,
reported that Olympus hemoclipping (with or without
investigators also reported significantly higher recurrent
concomitant epinephrine injection) yielded similar hemo-
bleeding rates in the injection arm of the studyThe
stasis rates and outcomes as epinephrine injection and
high hemostasis rates and the lack of complications with
multipolar coagulation. Gevers et reported that Olym-
hemoclipping are positive aspects of this technology.
pus hemoclipping with or without epinephrine injection
In more recent clinical trials, there have been compar-
was superior to injection of polidocanol alone.
isons of hemoclipping with other techniques for nonvari-
All previous clinical reports have used Olympus hemo-
ceal hemostasis, both thermal or combination treatments.
clips for endoscopic hemostasis.No clinical studies have
Comparisons of Olympus hemoclipping with heat probe
been reported with other types of hemoclips, such as Res-
have yielded conflicting results.Cippoletta et alre-
olution hemoclips, or Cook Endoscopy hemoclips. The
ported superior results with hemoclipping, which were re-
latter have different characteristics of size, strength, de-
lated to very low hemostasis rates for active bleeding with
ployment, and partial rotation, as shown in . All
heat probe and high rates with hemoclipping. In contrast,
these factors may effect acute hemostasis, retention, and
had significantly better results with heat probe, be-
possibly efficacy and safety with different hemoclips for
cause hemoclips failed or could not be deployed in about
nonvariceal hemostasis. To date, no comparative study
15% of the bleeding chronic ulcers, whereas heat probe
of hemoclips for hemostasis has been reported.
Volume 64, No. 5 : 2006 GASTROINTESTINAL ENDOSCOPY 771
Study of 3 hemoclips for hemostasis of acute ulcers
Our current study compared 3 different hemoclips,
enterologists today. Second, the endoscopic treatment in
which are currently available to the endoscopist for clini-
the stomach is very similar to hemostasis of bleeding hu-
cal hemostasis: the QC, the TC, and the RC. We compared
man gastric ulcers. The endoscopic techniques of finding
application difficulty, hemostatic efficacy, effect on ulcer
the ulcer, washing the ulcer base to expose bleeding sites,
healing, and retention time at the applied site.
and deploying the hemoclips, and of successful acute he-
Partial rotation of the hemoclip, once passed down the
mostasis of acute ulcers are equivalent to clinical acute ul-
endoscope, was subjectively somewhat easier and better
cer hemostasis. Third, the ability to place hemoclips on
controlled with the RC than with the QC, which tended
bleeding sites and hemoclip retention rates on acute gas-
to flip with shaft rotation. Acute failure of deployment oc-
tric lesions closely approximate hemostasis of acute ul-
curred approximately 10% of the time and was similar for
cers. Fourth, healing rates on high-dose oral PPIs are
all 3 hemoclips when used for hemostasis of moderate ul-
similar to human acute ulcers. Last, injury patterns and
cer bleeding in this model. All 3 hemoclips had similar he-
early recurrent bleeding in dogs with prehepatic portal hy-
mostasis rates for these acute ulcers. No major tissue
pertension parallel those seen in patients.
damage occurred with hemoclips, although the TC some-
This type of comparative study would not be easy to
times sliced through the edges of the acute ulcers.
perform or might not be possible in a clinical, controlled
There was no interference with ulcer healing. Ulcers
randomized study of ulcer hemostasis. Yet the observa-
with hemoclips retained appeared to heal somewhat
tions are very relevant to clinical choices, commonly
quicker (eg, RC or TC) or as fast (eg, QC) as control ulcer-
made by GI endoscopists treating patients with nonvari-
ations. RCs were retained the longest, and this may pro-
ceal GI hemorrhage. The differences in the hemoclip tech-
mote permanent hemostasis more often than TCs,
nologies cannot be overemphasized nor the need to
which generally all fell off before the 1 week follow-up en-
become facile with their deployment before endoscopic
doscopy. No complications, ill effects, or nutritional conse-
use, especially with emergencies. The results of this com-
quences occurred either because of the passage of the
parative study should interest endoscopists, GI techni-
The potential limitations of this study include the fol-
lowing. First, the study was performed under controlled
laboratory conditions by highly experienced endoscopists
All devices required similar experience and time to
who had practiced each hemoclip technique before start-
learn how to place clips successfully.
ing this study. Clinical results by those endoscopists or
Initial hemostasis rates for acute ulcers were similar for
their assistants who are not facile with hemoclip deploy-
ment for acute nonvariceal upper-GI hemostasis may be
The TC short-term retention rates were significantly
quite different. Second, the lesions were acute, small, gas-
tric ulcers rather than chronic, large, deep (often fibrotic)
The long-term clip retention rate was significantly higher
peptic ulcers. The endoscopic techniques, placement suc-
with RC than the other 2 hemoclip types.
cess, retention rates, and performance of different types of
All 3 hemoclips were safe and did not interfere with
hemoclips with chronic peptic ulcers undoubtedly will be
different than acute, small ulcers.Third, bleeding gastriculcers were purposely placed en face in this study to facil-itate comparisons of endoscopic hemoclipping with differ-
ent devices. Clinically, hemoclip placement or deploymentmay be technically significantly more difficult, especially
The authors thank Jeffrey Gornbein for biostatistical
with tangentially oriented, duodenal, or high gastric le-
support and Michelle Meadows for the word processing.
sions, especially in retroflexion. Last, the bleeding ratesof these lesions (even with the heparin and portal hyper-tension) is modest, and no ulcers had spurting arterial
bleeding and required pre-injection with dilute epineph-rine to slow bleeding, continued target jet washing, or
This research was partially funded by research grants
clot removal to facilitate endoscopic visualization. These
from Boston Scientific Corp, Olympus America Corp, and
prehemoclip, endoscopic techniques will often be neces-
sary in clinical endoscopic hemostasis of spurting ulcersor other nonvariceal upper-GI lesions or those types of le-sions with adherent clots.
There are several major strengths and advantages of
1. Jensen DM. Where next with endoscopic ulcer hemostasis? Am J Gas-
this animal model and study. First, all ulcers were oozing
or moderately bleeding, which mimic the vast majority
2. Jutabha R, Jensen DM, Machicado GA, et al. Randomized controlled
of nonvariceal GI (upper or colon) lesions seen by gastro-
studies of injection: gold probes compared to monotherapies for
772 GASTROINTESTINAL ENDOSCOPY Volume 64, No. 5 : 2006
Study of 3 hemoclips for hemostasis of acute ulcers
hemostasis of bleeding canine gastric ulcers. Gastrointest Endosc
15. Cippoletta L, Bianco MA, Marmo R, et al. Endoclips versus heater
probe in preventing early recurrent bleeding from peptic ulcer: a pro-
3. Kuramata H, Eto S, Horiguchi K, et al. Evaluation of gastrofiberscope
spective and randomized trial. Gastrointest Endosc 2001;53:147-51.
for treatment (TGF proto-type by Olympus Co). Stomach Intestine
16. Jensen DM, Kovacs TOG, Jutabha R, et al. Randomized, controlled trial
of medical therapy compared to endoscopic therapy for prevention of
4. Hayashi T, Yonezawa M, Kawabara T. The study on staunch clip for the
recurrent ulcer hemorrhage in patients with non-bleeding adherent
treatment by endoscopy. Gastrointest Endosc 1975;17:92-101.
clots. Gastroenterology 2002;123:407-13.
5. Raju GS, Gajula L. Endoclips for GI endoscopy: technical review. Gas-
17. Jutabha R, Jensen DM, Martin P, et al. Randomized study comparing
banding and propranolol to prevent initial variceal hemorrhage in cir-
6. Hachisu T. Evaluation of endoscopic hemostasis using an improved
rhotics with high-risk esophageal varices. Gastroenterology 2005;128:
clipping apparatus. Surg Endosc 1988;2:13-7.
7. Binmoeller KF, Thonke F, Soehendra M. Endoscopic hemoclips treat-
18. Saltzman J, Strate LL, Di Sena V, et al. Prospective trial of endoscopic
ment for gastrointestinal bleeding. Endoscopy 1993;25:167-70.
clip versus combination therapy in upper GI bleeding (PROTECCT-UGI
8. Hachisu T, Yamada H, Satoh SI, et al. Endoscopic clipping with a new
Bleeding). Am J Gastroenterol 2005;100:1503-8.
rotatable clip-device and a long clip. Dig Endosc 1996;8:127-33.
19. Gevers AM, DeGoede E, Simoens M, et al. A randomized trial compar-
9. Lai YC, Yang SS, Wu CH, et al. Endoscopic hemoclip treatment for
ing injection therapy with hemoclip and with injection combined with
bleeding peptic ulcer. World J Gastroenterol 2000;6:53-6.
hemoclip for bleeding ulcers. Gastrointest Endosc 2002;55:466-9.
10. Villanueva C, Balanzo J, Sabat M, et al. Injection therapy alone or with
20. Jensen DM, Machicado GA, Hirabayashi K. Hemoclipping (CLIP) of
endoscopic hemoclip for bleeding peptic ulcer. Preliminary results of
chronic ulcers: a randomized prospective study of initial success,
a randomized trial [abstract]. Gastrointest Endosc 1996;43:361.
clip retention rates, and ulcer healing [abstract]. Gastrointest Endosc
11. Nishiaki M, Tada M, Yanai H, et al. Endoscopic hemostasis for bleeding
peptic ulcer using a hemostatic clip or pure ethanol injection. Hepato-gastroenterology 2000;47:1042-4.
12. Nagayama K, Tazawa J, Sakai Y, et al. Efficacy of endoscopic clipping
for bleeding gastroduodenal ulcer: comparison with topical ethanolinjection. Am J Gastroenterol 1999;94:2897-901.
Received February 15, 2006. Accepted June 5, 2006.
13. Chou Y-C, Hsu P-I, Lai K-H, et al. A prospective, randomized trial of
Current affiliations: CURE Hemostasis Research Group, CURE Digestive
endoscopic hemoclip placement and distilled water injection for
Diseases Research Center, David Geffen School of Medicine at UCLA, the
treatment of high-risk bleeding ulcers. Gastrointest Endosc 2003;57:
VA Greater Los Angeles Healthcare System, Los Angeles, California, USA.
14. Lin HJ, Hsieh YH, Tseng GY, et al. A prospective, randomized trial of
Reprint requests: Dennis M. Jensen, MD, CURE Digestive Diseases
endoscopic hemoclip versus heater probe thermocoagulation for
Research Center, Bldg 115, Rm 318, VA Greater Los Angeles Healthcare
peptic ulcer bleeding. Am J Gastroenterol 2002;97:2250-4.
System, 11301 Wilshire Blvd, Los Angeles, CA 90073-1003.
Volume 64, No. 5 : 2006 GASTROINTESTINAL ENDOSCOPY 773
Borrowing Rules The English and American Studies Library The English and American Studies Library is one of a number of libraries at the Faculty of Arts at the Charles University in Prague. It is subordinate to the Coordinating Methodological Centre, and closely collaborates with the Department ofAnglophone Literatures and Cultures and the Department of the English Language and ELT Methodol
O NASCIMENTO DO CIDADÃO DIFERENTE: PROGNÓSTICO OU JULGAMENTO Universidade de Santo Amaro - INTRODUÇÃO E OBJETIVOS O nascimento de bebês em condições que exigem a intervenção de profissionais da saúde são bastante comuns. No entanto, quando a condição, como no caso das anomalias congênitas, indica o desenvolvimento de deficiência, impedimento ou desvantage
 Study of 3 hemoclips for hemostasis of acute ulcers
TABLE 2. Results acutely and during follow-up weekly endoscopies
Hemoclip retention/no. successfully placed (%)
Mean time for Successful hemostasis/ Acute hemoclipping failure/
*P ! .05 vs other treatments.
Study of 3 hemoclips for hemostasis of acute ulcers
TABLE 2. Results acutely and during follow-up weekly endoscopies
Hemoclip retention/no. successfully placed (%)
Mean time for Successful hemostasis/ Acute hemoclipping failure/
*P ! .05 vs other treatments.