In Vitro Comparison of Particle Size Distribution/Respirable Dose for LiteAire Spacer versus Misty Max – 10 Nebulizer Using Albuterol. Sunil Dhuper MD, Sanjay Arora MD, Aziz Ahmed MD, Alpana Chandra MD ,Cynthia Chong MD, Chang Shim MD, Hillel W. Cohen DrPH, Scott Foss, Sonia Choksi MD North Central Bronx Hospital, 3424 Kossuth Avenue, Bronx, New York 10467 An Affiliate of The Albert Einstein College of Medicine Introduction
Despite tremendous variability in the number of MDI actuations (2-12) used in studies comparing beta agonist delivery via MDI/spacer and one unit dose ampule with a nebulizer, there is increasing literature support based on clinical trials for the use of 6 MDI actuations. As delivery systems influence the inhaled dose, it would be prudent to determine the in vitro dose outputs using the two systems prior to conducting a clinical efficacy comparison study between MDI/Spacer and nebulizer. In a prior in-vitro study, we have demonstrated no significant difference in the β-agonist total dose output between 6 actuations of MDI with LiteAire Spacer versus 1 unit dose ampule with a nebulizer. However, as particle size distribution was investigated with the two delivery systems, respirable dose output equivalency between the two systems remains undetermined. Therefore, the objective of this study is to compare the emitted dose particle size distribution and effective respirable dose between 6 actuations of albuterol MDI with LiteAire Spacer versus 1 unit dose ampule of a nebulizer.
Discussion
This study demonstrates that using the breath simulation technique there is no significant difference in the total dose output using 6 actuation of albuterol MDI spacer versus 1 unit dose
To determine the total dose output, a test device was attached to a USP
of nebulizer albuterol. Even though the difference in the respirable fraction between the two
throat model feeding into a filter connected to a Michigan Instrument Dual
modes of delivery using ACI was significant, there was no difference in the total dose output
Test Lung System. The lung was driven by a Puritan Bennet 7200 Ventilator
in the effective respirable dose calculated using the breath simulation studies. We also
set at 14 breaths/minute, tidal volume (TV) of 600 ml and inspiratory to
determined that the total dose deposition using ACI with the two modes of delivery was not
expiratory (I:E) ratio of 1:4. With LiteAire, an albuterol MDI (CFC Inhalation
significantly different and well in line with the method using the breath simulated techniques.
Aerosol – IVAX Pharmaceuticals, Inc.) was actuated at the beginning of
The total dose output was found to be 175.9±27.0 µg for 6
We used Oxygen at a flow rate of 8 LPM for nebulizing albuterol, a standard practice for
inhalation for 6 respiratory cycles (n=6 actuations) and with the nebulizer
actuations of albuterol delivered to a LiteAire Spacer via MDI
acute asthma in the emergency department. We determined that the impact of using oxygen
(Misty Max 10), one 3-ml vial (0.833mg/ml) of albuterol solution was delivered
versus 219.8±13.6 µg for a Misty Max 10 with T-piece. The
instead of room air on the cut off diameter in the ACI is negligible. The cut off diameters for the
over five minutes. O2 to the Nebulizer was set at a pressure of 50-Psi and a
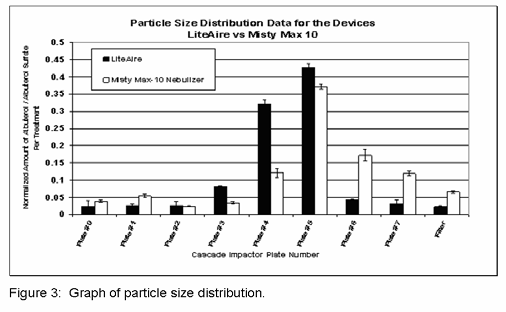
percent respirable fraction (defined as the total mass on plates # 3-
ACI are dependant on the viscosities of gas used with the impactor. The viscosity of air is
flow of 8 LPM. Each filter was washed with 0.05mM KCl with 1 % acetic acid
7 indicating a size range of 4.7-0.4 μm) was found to be
0.018centiPoise while that of 100% oxygen is 0.020centiPoise. The concentration of oxygen
buffer to collect the deposited drug. Dosage was determined using a UV
90.26±1.51% for LiteAire and 81.68±0.66% for the Misty Max 10
and the respective viscosity when delivered at 8 LPM, with ACI operating at 28.3LPM flow was
spectrophotometer, at a wavelength of 276 nm. Both devices were tested 3
(p<0.001). The particle size distributions are shown in Figure 3.
43% and 0.019centiPoise, respectively. Hence, the difference in viscosities of the two gases
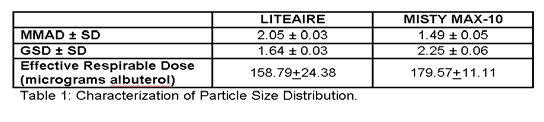
Table 1 summarizes the ACI results. The MMAD was 2.05±0.03 for
used for the two modes of delivery (MDI /Spacer vs. Nebulizer) would be 0.001centiPoise. The
Particle size was determined using an Andersen 8-Stage Cascade Impactor
the LiteAire versus 1.49 ± 0.05 for the Misty Max 10 (p<0.0001) and
impact of this difference on the cutoff diameters of ACI and therefore the respiratory particle
(ACI) with USP throat. The ACI was operated at 28.3 LPM. A filter for
the GSD was 1.64±0.03 for the LiteAire versus 2.25±0.06 for the
collection of particle was placed after the last plate of the ACI instead of a
Misty Max 10 (p<0.001). The effective respirable dose (total dose
The optimal time for nebulization has been reported in the literature. In a study by Malone
terminal filter inside the impactor. A TSI flow meter was connected between
output from the breath simulation studies * respirable fraction in
et al, it was determined that aerosolization past the sputtering point did not increase albuterol
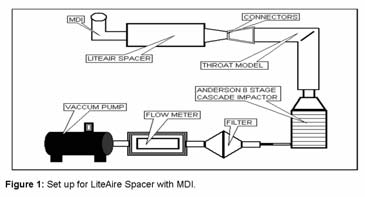
the ACI and vacuum pump. For the spacer unit (Figure 1), the vacuum pump
micrograms) was 158.79+24.38 micrograms with the LiteAire vs.
delivery. The study observed an abrupt decline in aerosol output that always corresponded to
was turned on for at least 60 seconds. Six doses of medication were
179.57+11.11 micrograms for the Misty Max 10 ( p=0.27)
the nebulizer sputtering with no change in the albuterol output between 30 to 60 seconds after
dispensed at the rate of one actuation of albuterol MDI every
the sputtering time for three different volumes (1.5 ml, 2.5 ml, and 3.5 ml albuterol solutions).
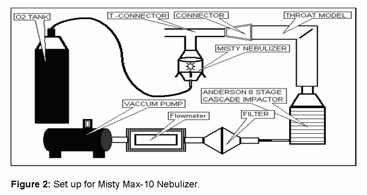
ten seconds. For the T-nebulizer, setup using the Misty Max 10 (Figure 2),
We chose 5 minutes nebulization time in our study as this was one minute past the sputtering
the vacuum pump was turned on for at least 60 seconds and one 3-ml vial
(0.833mg/ml) albuterol solution was delivered over five minute period using O2 at 8 L/min to the nebulizer. Each plate and the filter were washed separately with 10ml of 0.05 mM KCl with 1% acetic acid solution to obtain 9
Conclusion
samples. The 9 samples underwent analysis to quantify the dose of albuterolusing a UV spectrophotometer (λ=276 nm). The above experiment was
When conducting a clinical efficacy study comparing MDI/Spacer and one unit dose of
repeated for a total of three times (N=3), for both devices.
albuterol delivered via nebulization, we recommend using 6 albuterol MDI actuations with spacer as the in vitro dose outputs with the two modes are comparable.
GETTING READY FOR NASAL SURGERY What to expect - You can expect to have visible bruising and swelling for several weeks. You can expect to have drainage for a few days. 6 WEEKS BEFORE SURGERY Your surgeon may request abstinence from smoking and all tobacco products 6 weeks before and 6 weeks afterward. Failure to abstain from tobacco may result in your surgery being postponed or canceled
Alma Mater Studiorum University of Bologna, August 22-26 2006 LANGUAGE USE IN AUTOBIOGRAPHICAL MEMORY FOR MUSICAL EXPERIENCES Dr. Mark Lammers Dr. Mark Kruger ABSTRACT opment of the self, social bonding, and motivation (Bluck, Memories for musical experiences among adults associated 2003; Pillemer, 2003). Because music is a pervasive part of with a symphony orches
 In Vitro Comparison of Particle Size Distribution/Respirable Dose for LiteAire Spacer versus Misty Max –
In Vitro Comparison of Particle Size Distribution/Respirable Dose for LiteAire Spacer versus Misty Max –