Clinical Review
Received: October 18, 2001Accepted: April 15, 2002
Therapy of Sneddon Syndrome
Agnes Flöel Tanya Imai Hubertus Lohmann Florian Bethke
Department of Neurology, University of Münster, Münster, Germany
Key Words Introduction
Sneddon syndrome W Epilepsy W Cognition WAnticoagulation W Antiplatelet therapy
Sneddon syndrome (SNS) is characterized by the asso-
ciation of ischemic cerebrovascular events with wide-spread livedo racemosa primarily on the trunk [1]. The
Abstract
presence of several other organ manifestations such as
We report the case of a young woman with progressive
cardiac and kidney lesions suggests that it is a systemic
cognitive decline and epilepsy. She showed ischemic
cerebrovascular disease and proximal livedo racemosa.
Livedo racemosa is a cutaneous sign consisting of strik-
Antiphospholipid antibody (aPL) could not be detected
ing violaceous, netlike-patterned erythemas of the skin,
and there were no microemboli on continuous transcra-
with irregular, broken circular segments. It is localized on
nial Doppler ultrasonography monitoring. Histology of
both trunk and extremities and persists on warming [3]. It
cerebral vessels showed intimal hyperplasia in small lep-
results from persistent and irregular focal impairment of
tomeningeal venous vessels and micronecrosis of grey
the blood flow in cutaneous vessels, e.g. due to partial or
and white matter. We subsequently made the diagnosis
complete occlusion or to increased viscosity, and can be
of aPL-negative Sneddon Syndrome (SNS). Anticoagula-
found in atherosclerosis, vasculitis, or SNS.
tion with warfarin could not be initiated because of a
The onset of cerebrovascular events in Sneddon syn-
drug-resistant epilepsy with the risk of falls and subse-
drome usually occurs before the age of 45 years. Hemipar-
quent bleeding; immunosuppression with steroids and
esis, hemisensory symptoms, dysphasia, and visual symp-
azathioprine was ineffective, as was initial antiplatelet
toms are common. As medium-sized arteries are mainly
therapy with clopidogrel alone. However, when we in-
affected, strokes are rarely fatal, and good recovery is
tensified antiplatelet therapy by combining clopidogrel
observed initially. However, recurrent events frequently
and ASS, a slowing of disease progression, as assessed
lead to functional disability and vascular dementia. Ap-
by neuropsychological testing and magnetic resonance
proximately half of the patients report of headache. Cra-
imaging, was noted on a follow-up after 6 months. Ther-
nial magnetic resonance imaging (MRI) detects cortical,
apeutic options in SNS in both aPL-positive and aPL-neg-
subcortical or cortico-subcortical abnormalities sugges-
ative patients with SNS are discussed.
tive of arterial ischemic infarcts which are frequently mul-
tiple [2, 4]. Usually, periventricular white matter changes
Department of Neurology, University of Münster
Tel. +49 251 834 9969, Fax +49 251 834 8181, E-Mail [email protected]
are observed [5]. Diffuse cortico-subcortical atrophy is
family history of skin lesions, cognitive dysfunction and stroke-like
observed in late stages of the disease. Heart valve abnor-
On physical examination, the patient (84 kg, 174 cm) was in a
malities are detected in half of the patients [4]. Both aortic
reduced general state of health. Her blood pressure was 140/96 mm
and mitral valve lesions may occur [4]. Mild to moderate
Hg. The neuropsychological assessment revealed a significant decline
systemic hypertension has been found in approximately
since her first neuropsychological evaluation 2 years ago (table 1, 1st
60% of patients with SNS. Venous thrombosis occurs in
examination). Her main problems had then been reduced mental
15% of patients [4]. Decreased creatinine clearance and
speed, reduced mental flexibility and impaired word production(‘verbal fluency’). Other functions, including long-term memory,
even chronic renal failure has been reported [6].
immediate and delayed recall, language, visuospatial abilities, praxis
The prevalence of antiphospholipid antibodies (aPL)
and judgement had either been average or above average. Now, she
in SNS has been reported to range from 0 to 85% depend-
showed a predominantly dysexecutive syndrome [9], i.e. mental flex-
ing upon the series [4, 6]. Patients with SNS and aPL are
ibility was moderately impaired. Verbal and spatial working memory
more likely to develop epilepsy (30% in aPL-positive vs.
and selective attention were severely impaired. Mild behavioralchanges were also noted. Other higher cognitive functions (language,
10% in aPL-negative cases [2]). Optimal management of
visuospatial abilities, praxis, judgement) were unimpaired (table 1,
patients with SNS remains an unsolved problem. Pro-
spective randomized controlled trials are not available
Her motor examination showed weakness and dysdiadochokine-
[7]. Therapeutic management is based either on treating
sia of the left arm. Her tendon reflexes were brisk but symmetrical,
detectable anomalies of the coagulation system such as
coordination and sensation were normal. She had livedo racemosaon the back of the upper arms and on the back of the legs (fig. 1).
aPLs (inference from treatment of single patients with
These skin signs were discrete and had not been noted before. Skin
aPLs), or is based on pathophysiological assumptions.
biopsy revealed small vessels in the subcutis with a reorganizing
Positive effects of anticoagulation, antiplatelet therapy
small thrombus, and other small vessels showed an endothelial thick-
and immunosuppression, alone or in combination, have
ening. There were no signs of an inflammatory process, especially no
been observed, but they were often minimal at best. Slow-
signs of vasculitis (fig. 2). MRI of the brain showed bihemisphericconfluent signal increases on T
ing down or even reversing the cognitive decline has rare-
in cortical regions and parieto-occipital subcortical white matter
ly been possible [7]. Concomitant diseases which carry an
increased risk of bleeding, such as epilepsy with an
On MR spectroscopy, she had neuronal degeneration (N-acetyl-
increased risk of falls, uncontrolled hypertension, poor
L-aspartate reduction), but no lactate increase. Therefore, a mito-
compliance, liver disease, peptic ulcer and previous cere-
chondrial encephalopathy with lactic acidosis and stroke-like epi-sodes was highly unlikely. EMG was normal. Muscle biopsy showed
bral hemorrhage have to be considered in each patient
an unspecific mild type-II atrophy. Doppler ultrasonography of the
intra- and extracranial arteries was normal. There were no clinically
In the present study, we report on a young woman with
silent circulating microemboli on 1-hour continuous transcranial
aPL-negative SNS and drug-resistant epilepsy. Her clini-
Doppler monitoring of both middle cerebral arteries. Transthoracic
cal course under different treatment regimens is de-
echocardiography showed a tricuspid aortic valve with insufficiencygrade 1, and a minimal tricuspid valve insufficiency. An MRI-guided
scribed, followed by a general discussion of treatment
stereotactic brain biopsy yielded only inconspicuous brain tissue.
However, a subsequent CT scan of the head revealed that the biopsyhad been taken slightly off the lesion. Therefore, a second MRI-guided stereotactic brain biopsy was performed, which showed mul-tiple, predominantly older and mostly incomplete micronecroses of
Case Report
grey and white matter and a white matter degeneration. Thesechanges were due to intimal hyperplasia in small leptomeningeal
A 29-year-old woman (D.N.) presented to the department of neu-
veins, most likely secondary to disseminated thromboses with recan-
rology with a 5-year history of focal epilepsy with secondary generali-
alization (fig. 4). Extensive laboratory studies uncovered no evidence
zation, which had proven pharmacoresistent despite various antiepi-
of vasculitis, hypercoagulable state, or toxic metabolic disturbances.
leptic drug regimes, including carbamazepine, valproic acid, lamotri-
The following tests were all normal: full blood count, coagulation
gine, phenytoin, gabapentin and topiramate. Additionally, there was
tests including detection of antithrombin III, protein C, and protein
a progressive 3-year decline in cognitive function. She had poor con-
S deficiency, homocysteine blood levels (N ^12 Ìmol/l), fasting
centration, easy fatigue and increasing difficulty in word retrieval.
serum glucose, complement (CH50, C3, C4), cryoglobulins, cryofi-
This had led to her quitting a secretary trainee program in August
brinogen, rheumatoid factor, antineutrophil cytoplasmatic anti-
1998, and she had had no employment since then. Lately, she had
bodies and serum immunelectrophoresis. Lupus anticoagulant and
had difficulties coping with everyday household work and her 8-
anticardiolipid antibodies (IgM and IgG) 1 and 2, and beta 2 glyco-
protein I were found normal on five occasions in a 1.5-year period.
Her medical history was significant for elevated arterial blood
The patient was diagnosed as having aPL-negative SNS. Antico-
pressure since the age of 18, a chronic tension headache and atopic
agulation, antiplatelet and/or immunosuppressive therapy were con-
dermatitis. No stroke-like episodes were reported. There was no
sidered. Since no coagulopathy had been detected and the patient
Fig. 1. Photograph of the right upper arm of patient D.N. Her livedo racemosa presents as a violaceous, broken rash. Fig. 2. Skin biopsy of patient D.N. (hematoxylin-eosin, original mag- nification: !32). Histology reveals small vessels in the subcutis with endothelial thickening (arrow). Table 1. Neuropsychological evaluations of patient D.N. over the course of 38 months
WMS-R = Wechsler Memory Scale – Revised; RAVLT = Auditory Verbal Learning Test; WAIS-R = Wechsler Adult Intelligence Scale – Revised; TMT = Trail
Making Task; COWA = Controlled Oral Word Association. 1
Percentile: e.g., the 75th percentile is a score that is equal to or better than 75% of all subjects who were tested.
Flöel/Imai/Lohmann/Bethke/Sunderkötter/Droste
Fig. 3. Axial, T2-weighted cranial MRI of patient D.N. In the frontal and parieto-occi- pital cortical regions and subcortical white matter, bihemispheric confluent signal in- creases on T2-weighted images can be seen. Fig. 4. Small leptomeningeal blood vessels showing marked endothelial hyperplasia (ar- row) (hematoxylin-eosin, original magnifica- tion: !64).
had a high risk of falls with subsequent intracranial hemorrhage
of carcinomas) was stopped. Antiplatelet therapy was intensified by
because of her drug-resistant epilepsy, we decided against warfarin
adding aspirin (50 mg per day) to clopidogrel.
anticoagulation. An antiplatelet agent (clopidogrel, 75 mg per day)
Six months later, the patient was seen in our outpatient clinic. She
was given. More aggressive therapies like immunosuppression were
did not complain of any further cognitive decline. Neuropsychologi-
discussed with the patient and her family. Primarily because of the
cal examination did not reveal any significant changes compared
rapid cognitive decline over the last 2 years, a therapeutic immuno-
with the testing 6 months ago (small improvement in attentional
suppressive trial (steroids plus azathioprine) was started ex juvanti-
tasks, deterioration in verbal learning and memory tasks) (table 1,
Additionally, her antiepileptic medication was changed; most
importantly, medication that caused drowsiness (carbamazepine,phenytoine) was reduced. Subsequently, under valproic acid medica-
Discussion
tion only, she improved significantly on working memory and learn-ing tasks, but still showed a dysexecutive syndrome (table 1, 3rdexamination).
SNS is clinically defined as the combination of livedo
She returned to hospital 6 months later because of dizziness, nau-
racemosa and cerebrovascular events [1, 11]. Because no
sea and diplopia that began after an increase in her antiepileptic
specific test for SNS exists, clinical differentiation from
medication (valproic acid) 10 days before admission, and which dis-
other phenomenologically similar disorders may be diffi-
appeared after reduction of valproic acid.
She also reported a further decline in memory and concentration
cult and has raised controversy [2, 11–15]. Various neuro-
over the past 6 months. On neurological examination, she showed
logical problems have been associated with SNS and
slurred speech and weakness of the left arm, which persisted after
aPLs, including cerebrovascular events, chorea, seizures,
reduction of her antiepileptic medication. On neuropsychological
myelopathy, atypical migraine-like events, acute encepha-
assessment, she had a dysexecutive syndrome with decline in mental
lopathy, and dementia [3, 4, 12, 16, 17].
flexibility, working memory and selective attention (table 1, 4thexamination). An MRI of the head revealed a progression of frontal,
The first manifestation of disease in our patient was
occipital, temporo-occipital and cerebellar lesions. Additionally, a
drug-resistant epilepsy, followed by progressive cognitive
fresh lesion with blood degradation products in the right striatum
decline. Skin lesions were discrete, no coagulopathy was
was noted, consistent with an infarction in the previous 2–3 months.
detected. The patient did not present with acute cerebro-
In summary, no slowing in disease progression was observed since
vascular events. However, her cranial MRI suggested that
the initiation of antiplatelet and immunosuppressive therapy 6months ago. Therefore, the potentially dangerous immunosuppres-
a number of microinfarctions had taken place in the pre-
sive therapy with azathioprine (increased risk of infection, induction
ceding years. Neither the signal pattern nor the distribu-
tion of white matter lesions were specific for SNS. Similar
A recent review [2] suggests that aPL-positive and aPL-
findings may be seen in other cerebrovascular disorders
negative SNS patients show distinct clinical and biologi-
affecting small arteries [3]. The diagnosis of SNS was ulti-
cal features. In aPL-positive patients, seizures and clini-
mately confirmed on brain (and skin) biopsy.
cally audible mitral regurgitation are more frequently
Stereotactic brain biopsy is invasive and carries a small
observed, the fishnet of the livedo is larger, and thrombo-
but definite risk of morbidity and even mortality. Nev-
cytopenia is present in about one third of patients [4]. In
ertheless, we opted for a brain biopsy, first to exclude any
comparison, thrombocytopenia has never been reported
treatable disease, and second to confirm the diagnosis of
in aPL-negative patients [2, 4, 14].
SNS. The options for treatment of SNS, anticoagulation,
Treatment of patients with SNS is still controversial.
antiplatetelet and/or immunosuppressive medication are
Categorization of SNS patients into two subsets (aPL-pos-
all long-term treatments, and carry a substantial risk
itive and aPL-negative), as described above, might in-
themselves. Therefore, in patients without aPLs, the deci-
sion about potentially harmful therapies should be based
APL-positive SNS patients might be treated like pri-
on a definite diagnosis. Skin biopsy, which is much less
mary antiphospholipid syndrome. In primary antiphos-
invasive, has been reported to yield no abnormalities on
pholipid syndrome, patients with the highest titers of
histological examination in the majority of patients in a
aPLs seem to have the greatest risk of recurrent thrombot-
study of 44 patients [4]. Not all studies agree on the validi-
ic events [12, 19]. A wide variety of treatments including
ty of brain biopsy in diagnosing SNS. A recent study by
antiplatelet agents, anticoagulants, corticosteroids, im-
Zipper et al. [18] reported inconclusive results for brain
munosuppressants has been tried, but no prospective ran-
biopsy. However, brain biopsy might not have been car-
domized controlled trials are available to guide manage-
ried out by an experienced examiner, and therefore the
ment. A retrospective analysis of patients with primary
biopsy might have missed the relevant area. Even a slight
antiphospholipid syndrome suggested that long-term anti-
deviation from the lesion area might lead to inconspic-
coagulation is advisable, with the INR maintained at 3 or
higher [2, 22, 24]. Therefore, in aPL-positive SNS pa-
The pathogenic mechanisms in SNS and primary anti-
tients, high-dose warfarin (INR 6 3) is currently mostly
phospholipid syndrome are incompletely understood [12,
19]. A defective vascular endothelium, alone or in combi-
Optimal management of aPL-negative SNS remains an
nation with a slight or nondetectable coagulation deficit,
unsolved problem [2]. In a study on aPL-negative patients
might traumatize the endothelium [4, 12, 20, 21]. The
with SNS, the number of cerebral events was lower with
presence of aPLs, most notably anticardiolipid antibodies
antiplatelet therapy; antiplatelet therapy was as effective
and lupus anticoagulant, may be detected in about half of
as high-dose warfarin [4]. Frances et al. [4] suggested that
the SNS patients, with a range from 0 to 85% depending
antiplatelet therapy might slow cognitive decline in aPL-
on the series [4, 6]. Their presence suggests that SNS
negative SNS patients, based on the observation that the
results from a thrombotic process [4, 12]. A number of
only patient in their study who developed frank dementia
authors have found noninflammatory endothelial prolif-
(of the vascular type) was the one who did not receive
eration and fibro-mucinous changes with subsequent oc-
clusion of small vessels [20]. Monitoring the middle cere-
Wohlrab et al. [28] suggested the use of a triple therapy,
bral artery using transcranial Doppler ultrasonography
i.e. in addition to antiplatelet therapy, angiotensin-con-
(TCD) showed clinically silent microembolisms in 38% of
verting enzyme inhibitors (ACE inhibitors) and prosta-
patients with SNS, all aPL-positive [22].
glandin E1 are to be given. ACE inhibitors are posited to
In aPL-negative cases, a primary inflammatory process
reduce angiotensin II-mediated proliferation and migra-
has been suggested [3, 4, 21], though a number of studies
tion of subendothelial vascular myocytes. Prostaglandin
did not show inflammatory changes on skin and brain
E1 might improve microcirculation by altering the rheo-
biopsies [11, 14], and the inefficacy of immunosuppres-
logical properties of the blood. The authors reported 5
sive therapies argues against a primary inflammatory vas-
patients treated with the triple combination who did not
show further clinical deterioration over the course of 3–5
Varying findings on microscopy might be due to differ-
ent underlying disease processes in patients clinically
In both aPL-positive and aPL-negative cases, limited
diagnosed with SNS [2]. It might also be due to sampling
effectiveness [3, 11, 14, 25] or frank inefficacy [13] of var-
in different stages of the disease [23].
ious immunotherapies, including steroids and azathio-
Flöel/Imai/Lohmann/Bethke/Sunderkötter/Droste
prine, has been repeatedly described. The use of cortico-
signals on continuous TCD monitoring does not argue
steroids and immunosuppressives without antithrombot-
ic agents seems to be deleterious as noted in 6 previously
In summary, patients diagnosed with SNS are to be
reported patients [4, 26]. A temporary improvement with
screened for antiphospholipid antibodies, arterial hyper-
high-dose corticosteroids and aspirin has been reported
tension (24-hour blood-pressure monitoring and ophthal-
moscopy), renal dysfunction (creatine clearance) and
The symptom most difficult to treat in both aPL-posi-
heart valve abnormalities (echocardiography).
tive and aPL-negative patients is cognitive decline [5, 29].
Therapeutically, aPL-positive patients should be start-
Mental deterioration is not only one of the most common
ed on high-dose warfarin (INR 63). If warfarin is con-
symptoms in SNS, but also one of the most important as
traindicated because of a concomitant disease, antiplate-
far as quality of life is concerned. It ranges from moderate
let therapy, ideally in the combination of two different
cognitive impairment [3, 5, 16] to frank dementia [3, 5].
agents (ASS and clopidogrel), is the most appropriate
Dementia in SNS occurs on a multi-infarct basis [16, 28].
Rare cases of more gradual cognitive decline without spe-
In aPL-negative patients, antiplatelet therapy, again in
cific acute cerebrovascular episodes have also been re-
combination, should be administered.
ported [29, 30]. On imaging, these cases show widespread
In both aPL-positive and aPL-negative patients, if dis-
changes in the form of cerebral infarction.
ease is rapidly progressive despite therapy, ACE inhibi-
Apart from aPLs, clinically silent microembolism has
tors and prostaglandin E1 might be given. Ultimately,
been posited to provide subclinical evidence of active dis-
immunosuppressive agents like steroids and azathioprine
ease in SNS patients, and might therefore guide thera-
can be tried, but always in combination with antithrom-
peutic approaches [22]. However, in our patient, no
microemboli were detected; still, the disease was clearlyprogressive, both clinically (further deterioration in men-tal flexibility, working memory and selective attention)
Acknowledgments
and on cranial MRI (progression of size of white matter
This work was supported by the Nachwuchsgruppen-Förderung
lesions, fresh lesion in the right striatum). This finding
of the Ministry of Science, Nordrhein-Westfalen (516-400 01000).
argues against a mechanism of arterio-arterial or cardio-
We thank Dr. C. Rickerts, Institute of Neuropathology, University of
genic microembolism as the pathomechanism in our pa-
Münster, Germany, for providing histological pictures of patient
tient. Intravascular, in situ thrombosis seems more likely
here [22]. Taken together, the absence of microembolic
References
1 Sneddon IB: Cerebrovascular lesions and live-
6 Kalashnikova LA, Nasonov EL, Borisenko VV,
11 Bruyn RP, van der Veen JP, Donker AJ, Valk
do reticularis. Br J Dermatol 1965;77:180–
J, Wolters EC: Sneddon’s syndrome. Case re-
Kushekbaeva AF: Sneddon’s syndrome: Car-
port and literature review. J Neurol Sci 1987;
2 Frances C, Piette JC: The mystery of Sneddon
diac pathology and antiphospholipid anti-
syndrome: Relationship with antiphospholipid
bodies. Clin Exp Rheumatol 1991;9:357–361.
12 Levine SR, Brey RL, Sawaya KL, Salowich-
syndrome and systemic lupus erythematosus. J
7 Wright RA, Kokmen E: Gradually progressive
Palm L, Kokkinos J, Kostrzema B, Perry M,
dementia without discrete cerebrovascular
3 Stockhammer G, Felber SR, Zelger B, Sepp N,
events in a patient with Sneddon’s syndrome.
thrombo-occlusive events in the antiphospho-
Birbamer GG, Fritsch PO, Aichner FT: Sned-
lipid syndrome. Ann Neurol 1995;38:119–
don’s syndrome: Diagnosis by skin biopsy and
8 Lip GY, Lowe GD: Warfarin and aspirin as
MRI in 17 patients. Stroke 1993;24:685–690.
thromboprophylaxis in atrial fibrillation. Br J
13 Rautenberg W, Hennerici M, Aulich A, Holzle
4 Frances C, Papo T, Wechsler B, Laporte JL,
Biousse V, Piette JC: Sneddon syndrome with
9 Bogousslavsky J, Kaste M, Skyhoj Olsen T,
and Sneddon’s syndrome. Lancet 1988;ii:629–
or without antiphospholipid antibodies. A
comparative study in 46 patients. Medicine
stroke prevention. European Stroke Initiative
14 Kalashnikova LA, Nasonov EL, Kushekbaeva
(EUSI). Cerebrovasc Dis 2000;10:12–21.
AE, Gracheva LA: Anticardiolipin antibodies
5 Tourbah A, Piette JC, Iba-Zizen MT, Lyon-
10 Baddeley A: The central executive: A concept
in Sneddon’s syndrome. Neurology 1990;40:
and some misconceptions. J Int Neuropsychol
course of cerebral lesions in Sneddon syn-
21 Sepp N, Zelger B, Schuler G, Romani N,
26 Geschwind DH, FitzPatrick M, Mischel PS,
Fritsch P: Sneddon’s syndrome – an inflamma-
FJ, Bermejo-Pareja F: Sneddon’s syndrome
tory disorder of small arteries followed by
with negative antiphospholipid antibodies.
smooth muscle proliferation. Immunohisto-
chemical and ultrastructural evidence. Am J
16 Weissenborn K, Ruckert N, Ehrenheim C,
27 Baleva M, Chauchev A, Dikova C, Stamenov
Schellong S, Goetz C, Lubach D: Neuropsycho-
22 Sitzer M, Sohngen D, Siebler M, Specker C,
B, Nikoevski N, Tzankov N, Nikovov K: Sned-
logical deficits in patients with Sneddon’s syn-
Rademacher J, Janda I, Aulich A, Steinmetz H:
don’s syndrome: Echocardiographic, neurolog-
ical, and immunologic findings. Stroke 1995;
17 Schellong SM, Weissenborn K, Niedermeyer J,
Sneddon’s syndrome. Arch Neurol 1995;52:
Wollenhaupt J, Sosada M, Ehrenheim C, Lu-
28 Wohlrab J, Fischer M, Marsch C: Aktuelle
bach D: Classification of Sneddon’s syndrome.
23 Zelger B, Sepp N, Stockhammer G, Dosch E,
Hilty E, Ofner D, Aichner F, Fritsch PO: Sned-
18 Zipper SG, Lambert S, Seemann WR, Baer U,
don’s syndrome. A long-term follow-up of 21
29 Devuyst G, Sindic C, Laterre EC, Brucher JM:
Schlisske K: Sneddon syndrome: Vasculitis or
patients. Arch Dermatol 1993;129:437–447.
Neuropathological findings of a Sneddon’s syn-
thrombotic disorder? Med Klin 2000;95:158–
24 Krnic-Barrie S, O’Connor CR, Looney SW,
drome presenting with dementia not preceded
Pierangeli SS, Harris EN: A retrospective re-
by clinical cerebrovascular events. Stroke 1996;
19 Feldmann E, Levine SR: Cerebrovascular dis-
view of 61 patients with antiphospholipid syn-
ease with antiphospholipid antibodies: Im-
drome. Analysis of factors influencing recur-
30 Gorman DG, Cummings JL: Neurobehavioral
mune mechanisms, significance, and thera-
rent thrombosis. Arch Intern Med 1997;157:
presentations of the antiphospholipid antibody
syndrome. J Neuropsychiatry Clin Neurosci
25 Rosove MH, Brewer PM: Antiphospholipid
20 Daoud MS, Wilmoth GJ, Su WP, Pittelkow
thrombosis: Clinical course after the first
thrombotic event in 70 patients. Ann Intern
Flöel/Imai/Lohmann/Bethke/Sunderkötter/Droste
McDonald's USA Ingredients Listing for Popular Menu Items Provided below is a listing of components in our popular menu items by category, followed by the ingredient statements for those components. Allergens containedwithin these components are indicated in capital type at the end of each respective ingredient statement. We encourage customers to check these statementsregularly as ingredie

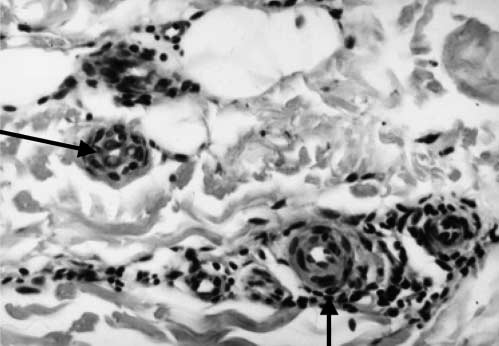 Fig. 1. Photograph of the right upper arm of patient D.N. Her livedo
Fig. 1. Photograph of the right upper arm of patient D.N. Her livedo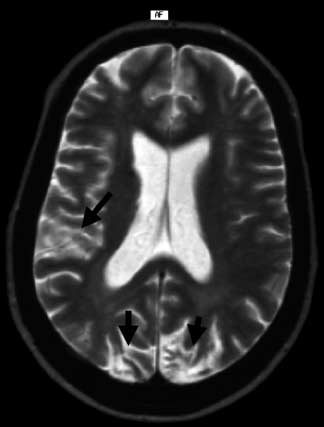
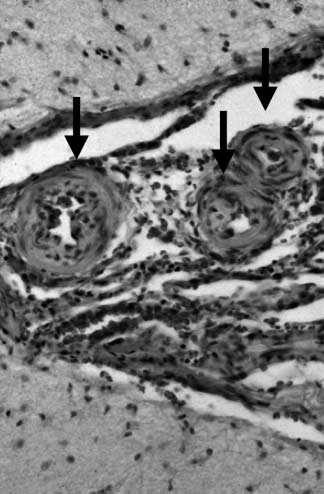 Fig. 3. Axial, T2-weighted cranial MRI of
Fig. 3. Axial, T2-weighted cranial MRI of