The Effects of Balance Training and High-Intensity Resistance Training on Persons With Idiopathic Parkinson’s Disease Mark A. Hirsch, PhD, Tonya Toole, PhD, Charles G. Maitland, MD, Robert A. Rider, PhD
ABSTRACT. Hirsch MA, Toole T, Maitland CG, Rider RA.
mine pathway.1 Clinical signs of bradykinesia, rhythmic
The effects of balance training and high-intensity resistance
tremor, rigidity, and postural instability follow dopamine de-
training on persons with idiopathic Parkinson’s disease. Arch
pletion.2 Optimal management of Parkinson’s disease (PD)
involves both pharmacologic treatment and encouragement ofphysical activity,3 yet few well-controlled prospective studies
Objective: To assess immediate and near-term effects of 2
have documented the benefits of physical activity in PD.4-6
exercise training programs for persons with idiopathic Parkin-
Recent work with animal models of PD, stroke, and spinal cord
injury indicates that rehabilitative training can stimulate a
Design: Randomized control trial.
number of plasticity-related events in the brain and the spinal
Setting: Public health facility and medical center.
cord, including neuronal outgrowth, neurotrophic factor ex-
Participants: Fifteen persons with IPD.
pression, synaptogenesis, and even neurogenesis.7-16 These
Intervention:
use-dependent events, in turn, enhance the range of self-regu-
training) and balance group (balance training only) underwent
lated movements that may contribute to a greater plasticity and
10 weeks of high-intensity resistance training (knee extensors
improved behavioral outcome. Moreover, during slow degen-
and flexors, ankle plantarflexion) and/or balance training under
eration of nigrostriatal dopaminergic neurons, coapplication of
altered visual and somatosensory sensory conditions, 3 times a
intense sensorimotor training appears to be neuroprotective.17
week on nonconsecutive days. Groups were assessed before,
Our study evaluates the effect of a series of physiotherapeu-
immediately after training, and 4 weeks later.
tic exercises selected on the basis of their efficacy in improving
Main Outcome Measures: Balance was assessed by com-
balance in frail older adults.18-22 Strategies for enhancing bal-
puterized dynamic posturography, which determined the sub-
ance among older adults with PD are needed, because in the
ject’s response to reduced or altered visual and somatosensory
absence of regular physical activity, balance and muscle
orientation cues (Sensory Orientation Test [SOT]). Muscle
strength deteriorate in persons with PD.6 Many persons with
strength was assessed by measuring the amount of weight a
PD report impaired balance and falls.23-30 Koller et al27 found
participant could lift, by using a standardized weight-and-
that balance impairment in older adults with longer duration
pulley system, during a 4-repetition-maximum test of knee
PD usually does not respond to levodopa; 38% of persons with
extension, knee flexion, and ankle plantarflexion.
PD experienced falls; 13% fall more than once per week; some
Results: Both types of training improved SOT performance.
report falling repeatedly throughout the day; and persons with
This effect was larger in the combined group. Both groups
PD are 5 times more likely than healthy older adults to suffer
could balance longer before falling, and this effect persisted for
falls-related injuries, such as hip fractures.30
at least 4 weeks. Muscle strength increased marginally in the
Recently Olanow and Koller2 and Glendinning and Enoka31
balance group and substantially in the combined group, and
identified risk factors for falls in PD including postural insta-
this effect persisted for at least 4 weeks.
bility and muscle weakness. Studies have documented im-
Conclusion: Muscle strength and balance can be improved
paired knee and ankle muscle strength in PD32-36 and dyssyn-
in persons with IPD by high-intensity resistance training and
movement initiation.37,38 Specifically, persons with PD show
Key Words: Balance; Exercise; Parkinson disease; Rehabil-
reduced peak torque production in knee extension, knee flex-
ion, and ankle dorsiflexion in comparison with healthy age-
2003 by the American Congress of Rehabilitation Medi-
matched adults—muscle weakness is not related to rigidity or
cine and the American Academy of Physical Medicine and
tremor, and the unaffected leg in persons with PD is weaker
than either leg in subjects without PD.35,36 Isometric forceproduction, release of isometric force, and rate of force gener-
IDIOPATHIC PARKINSON’S DISEASE (IPD) features im- ation are also abnormal in some patients with PD,37-40 suggest-
pairment of resting muscle tone and voluntary movement,
ing impairment in force production may be associated with a
because of loss of striatal dopamine in the nigrostriatal dopa-
reduced ability to generate rapid contractions.
We previously showed a strong relationship between lower-
body muscle strength and impaired balance in IPD.41 Eighty-eight percent of the variability on a standardized test of balance
From the Department of Physical Medicine and Rehabilitation, Johns Hopkins
(EquiTest®a) may be attributable to (1) peak torque of knee
University Medical Center, Baltimore, MD (Hirsch); Departments of Nutrition, Foodand Exercise Sciences (Toole) and Physical Education (Rider), Florida State Univer-
flexion relative to that of knee extension, (2) peak torque of the
sity, Tallahassee, FL; and Neuroscience Center and Balance Disorders Clinic, Talla-
inversion of the ankle, and (3) use of an ankle strategy to
control balance.41 During an “ankle strategy,” the individual
No commercial party having a direct financial interest in the results of the research
uses the ankle as a fulcrum to control sway, allowing the
supporting this article has or will confer a benefit upon the authors(s) or upon anyorganization with which the author(s) is/are associated.
shoulders and hips to stay aligned with the ankles. Individuals
Reprint requests to Tonya Toole, PhD, Dept of Nutrition, Food, & Exercise
with weak ankle muscle strength were likely to fall on this
Sciences, Florida State University, 436 Sandels Bldg, Tallahassee, FL 32306-1493,
balance test and subjects swayed excessively when the ratio of
hamstring strength to quadriceps strength was less than two
0003-9993/03/8408-7700$30.00/0doi:10.1016/S0003-9993(03)00046-7
thirds.41 Lower-extremity weakness in persons with PD may
Arch Phys Med Rehabil Vol 84, August 2003 STRENGTH AND BALANCE IN PARKINSON’S DISEASE, Hirsch Table 1: Pretreatment Subject Characteristics
were volunteers who had been diagnosed with IPD by theirneurologist and who had not participated in any organized
balance or muscle strengthening activities before being pre-tested. All participants were ambulatory, were not acutely ill,
were able to follow simple commands, and were not suffering
from unstable cardiovascular disease or other uncontrolled
chronic conditions that would interfere with the safety and
conduct of the training and testing protocol. A total of 15
patients qualified for the study. Because Tallahassee is a rela-
Ϸ200,000 people), it is very difficult to recruit
larger numbers of patients who qualify and who also will invest
the time for testing and intervention. The protocol was ap-
proved by the Human Subjects Committee of Florida State
University and reviewed by the participants’ primary care
physicians, who also gave their written consent. All partici-
pants gave informed consent for the procedures used.
During the study, participants were taking Parkinson’s medica-
tions, that is, levodopa and carbidopa (Sinemet) (nϭ11), selegiline(Eldepryl) (nϭ12), pergolide (Permax) (nϭ1 ), bromocriptine
NOTE. Values are mean Ϯ standard error of the mean.
Abbreviations: Age at initial diagnosis, age at participants initial
ϭ3), and amantadine (nϭ2). Participants followed
diagnosis with PD; Disease duration, time lapse from initial diagno-
their normal schedule of medications throughout the course of the
sis to beginning of study; EquiTest falls, average number of falls on
study and we tested them 2 hours after they had ingested their
pretest EquiTest conditions 4 – 6; Latency to fall, number of seconds
morning dose and within the same relative temporal period of their
elapsed before an EquiTest fall occurred; % EquiTest trials resultingin falls, total number of trials (conditions 4 – 6, as defined in table 2)
drug cycle (between 9:00 AM and 12:00 PM). Parkinson’s medica-
divided by number of trials resulting in falls; Summary EquiTest
tions were not changed during the study.
score, averaged score from the 3 trials of EquiTest conditions 4 – 6;
All participants were first pretested for balance and then
Strength score, averaged score from the 3 muscle strength tests;Strength to body weight ratio, strength divided by body weight;
pretested for muscle strength on separate days. After assess-
Hamstring to quadriceps ratio, hamstring strength score divided by
ment, participants were randomly assigned to 1 of 2 training
groups. To prevent an unequal distribution of nonfallers and toensure that each group contained a similar number of subjectswho fell during the EquiTest, 4 subjects who had not fallen on
impair the ability to mount postural responses of an appropriate
any trial of the EquiTest were paired (2 men, 2 women) and
randomly assigned to the 2 groups. Then subjects who did fall
Other authors2,6,29,31 have suggested that balance impairment
during the EquiTest were randomly assigned to the 2 groups.
in PD and normal age-related physical changes, such as de-
Both groups received identical balance training exercises, but
clines in muscle strength which occur in adults19,22 (healthy and
the combined group also engaged in resistance training. All
pathologic populations) who do not exercise to strengthen
physiologic measurements were obtained at baseline (pretreat-
muscle, may respond favorably to muscle-strengthening and
ment) and repeated within 5 days of completion of training
balance rehabilitation. Physical interventions related to enhanc-
(posttreatment). Additionally, measurements were repeated 4
ing balance and muscle strength and potentially reducing falls
weeks after training ceased (follow-up treatment). Participants
are relatively inexpensive interventions that help prevent dys-
did not train during this 4-week period. Exercise sessions for
function and dependence in the elderly and would appear to be
both groups were conducted at different times of the day.
a logical avenue for addressing balance impairment in personswith PD. Testing and Intervention
The aim of this study was to determine how a specific group
rehabilitation program would influence muscle strength and
Muscle strength testing.
balance in patients with IPD. We hypothesized that the bene-
tensors, knee flexors, and ankle plantarflexors was measured at
ficial effects would include enhanced balance scores and mus-
baseline, after 10 weeks of training, and 4 weeks after training
cle strength on 2 standardized tests. If so, this work would
had ceased by using standardized weight-and-pulley systems.b
suggest that outpatient rehabilitation involving resistance train-
The 4-repetition maximum was defined as the highest weight
ing and/or balance training may be a useful adjunct to current
the seated participant could lift 4 times only from 90° of knee
medical therapy in PD. To test this hypothesis, a 2-group
flexion to full knee extension, from 170° of knee extension to
experimental design was used. We compared the results from a
90° of knee flexion, and from 90° of ankle flexion (neutral) to
group with balance training alone to the results from a group
with a combination of resistance training and balance training.
After a 5-minute warm-up on a cycle ergometer, and famil-
Patients were tested before and at the end of the intervention as
iarization with the equipment, both legs were tested concur-
well as 4 weeks after cessation of training.
rently. Participants practiced 4 warm-up movements and thenperformed 4 maximum movements for each joint movement.
Weights were added in small increments (1.1–2.3kg), andparticipants rested 30 seconds between sets. The test ended
Participants
when the participant could no longer perform 4 maximum
Participants’ characteristics are listed in table 1. Participants
movements of full range of motion exercise. Reliability of the
were recruited from the members of the Big Bend Parkinson’s
measurements was tested; the test-retest correlation coefficient
Disease Support Group, Tallahassee, FL. Eligible participants
was .93 for knee extension, .98 for knee flexion, and .99 for
Arch Phys Med Rehabil Vol 84, August 2003 STRENGTH AND BALANCE IN PARKINSON’S DISEASE, Hirsch Table 2: Summary of Experiment Protocol for the Sensory
ments were altered systematically for fixed support and sway-
Organization Test (SOT)
referenced support and surround conditions, and under normal(eyes open), absent (eyes closed), and sway-referenced vision
(eyes sway-referenced). Under sway-referenced conditions, theplatform on which subjects stood and/or the visual surround
also moved proportionally to their AP sway. Sway-referenced
visual conditions show the participant’s ability to suppress
conflicting (inaccurate) visual inputs and to rely on alternative
An equilibrium score was determined for each balance con-
dition based on peak-to-peak sway amplitude in the AP axis.
This score expresses the participant’s sway relative to the
Abbreviations: Vestibular, vestibular apparatus; Prop, propriocep-
theoretical limits of stability; scores near 100 indicate minimal
tion; Condition 1, eyes open and fixed support; Condition 2, eyes
sway, whereas those near zero indicate more extreme sway.
closed and fixed support; Condition 3, eyes sway-referenced and
When a participant took a step, touched the surround panels, or
support sway-referenced; Condition 4, eyes open and support sway-
needed assistance from the technician, that trial was marked as
referenced; Condition 5, eyes closed and support sway-referenced;Condition 6, eyes sway-referenced and support sway-referenced.
a fall and the participant received an equilibrium score of zerofor that trial.
Participants were carefully positioned on the platform by
aligning the lateral malleoli (ankle joint) with the axis of
ankle plantarflexion, showing high reliability of the strength
rotation of the platform and visual surround. Before each trial,
participants were instructed to stand still and erect with arms by
Resistive intervention.
their side. Three 20-second trials were administered for each of
were performed on Nautilus equipmentb at a local health facil-
ity. Participants assigned to resistance training underwent a
Scores for conditions 1 through 3 did not change throughout
regimen of high-intensity progressive resistance training of the
the training period, so they were not included in the analysis.
ankle plantarflexors and knee extensors and flexors. These
Because the raw scores for conditions 4 through 6 were highly
muscle groups were chosen because of their presumed impor-
correlated, these data were combined to give a single summary
tance in balance in persons with PD.6,35 Resistance exercise
balance score. This summary balance score reflects perfor-
sessions lasted 15 minutes and were held 3 times weekly on
mance under the most difficult test conditions when the support
nonconsecutive days. Each participant was trained and super-
surface is sway-referenced and visual cues are misleading or
vised by an exercise leader who also recorded exercises com-
absent. Two other summary variables for conditions 4 through
pleted in a log. The 10-week resistance training protocol used
6, the mean latency to a fall (average number of seconds
an adaptation of standard rehabilitation principles of progres-
participants swayed before stepping or falling, touching the
sive-resistance training by using concentric and eccentric mus-
surrounding panels with hands, or needing assistance from the
cle contraction.43 The initial 4-repetition maximum was used to
technician to keep from sitting in the harness) and the propor-
set the load for the first 2 weeks at 60% of the 4-repetition
tion of falls (number of trials resulting in falls), were used as
maximum for each muscle group. Participants performed 1 set
additional measures of the subject’s ability to maintain postural
of 12 repetitions, moving both legs simultaneously at 6 to 9
stability under the most difficult conditions.
seconds per repetition, with no rest between repetitions, and
Balance intervention.
with a 2-minute rest between exercises. Emphasis was on
of balance training. Balance exercise sessions lasted 30 min-
performing the exercise with good form and minimal substitu-
utes and were performed on 3 nonconsecutive days per week.
tion of other muscle groups. At the end of the second week, the
The 10-week balance training program used an adaptation of
load was increased to 80% of the 4-repetition maximum. The
standard balance rehabilitation exercises that have been shown
4-repetition maximum was measured in all study participants
to improve balance in frail older adults,18-21 persons with PD,6
every 2 weeks; for those in the combined group, the training
and in older adults with vestibular pathology.49-51 Training was
stimulus was adjusted to keep the load at 80% of the new
in 2 areas: (1) standing with feet shoulder-width apart on foam
by using commercially available medium density foam padsc 4
Balance testing.
to 6in thick and (2) standing without foam. Training without
by using a computerized test for isolating individual sensory
foam included standing with feet shoulder-width apart and flat
and motor components of balance in standing humans.a The
on the ground with eyes open, eyes closed, and neck neutral or
EquiTest is a reliable method for following changes in balance
neck extended for 20 seconds. This sequence was repeated 5
after balance rehabilitation programs.6,41,44-51 The different sen-
times. Foam training involved balancing on a single 4-in thick
sory test conditions—1 through 6 — have been described table
piece of foam and then progressing to several pieces of foam
2.41 The EquiTest device consists of a moveable platform on
throughout the training period, with eyes open, eyes closed,
which a subject stands, which can rotate about an axis close to
and neck neutral or neck extended for 20 seconds. This se-
that of the ankle joint; and a surrounding screen enclosure that
quence was also repeated 5 times. By the end of the sixth week
can rotate about an axis close to that of the ankle joint. Two
of training, all participants were using 3 foam pads. Balancing
forceplates in the platform, 1 for each foot, are equipped with
on foam reduces the usefulness of somatosensory inputs of the
strain gauges that measure the x axis (anteroposterior [AP])
ankles for controlling balance, thereby challenging visual and
vestibular inputs for balance control. Head extension was used
We used a standardized EquiTest assessment protocol—
to provide unreliable vestibular feedback and, during this task,
Sensory Organization Test (SOT)— to measure how well par-
each participant extended their head as far as was comfortable.
ticipants maintained balance under progressively more difficult
During a second set of exercises the therapist gently per-
test conditions, which either disrupted or removed visual and
turbed the participant—pulling hard enough to challenge, yet
proprioceptive feedback. Visual and proprioceptive environ-
gently enough not to overshoot the participant’s limit of sta-
Arch Phys Med Rehabil Vol 84, August 2003 STRENGTH AND BALANCE IN PARKINSON’S DISEASE, Hirsch
bility. Perturbation exercises were designed to enhance the
(pretreatment, posttreatment, follow-up treatment) taken at dif-
participant’s limit of stability. The focus was on maintaining
ferent times, so the design for the balance scores was a 2ϫ3
equilibrium through counterbalancing motions by using the
(group by time of pre, post, follow-up) mixed model with
lower extremities. Sternal and dorsal perturbations were di-
repeated measures on the last factor.
rected at the participant’s shoulders, with the therapist standing
Latency to fall and proportion of falls analyses.
either behind the participant or in front. These exercises were
were 2 groups (balance, combined) and 3 sets of measurements
performed standing on the ground with eyes open or closed (20
(pretreatment, posttreatment, follow-up treatment) taken at dif-
times) and standing on foam with eyes open or closed (20
ferent times; the design for the latency to falls scores was a
times). Weight-shifting exercises were then performed with
2ϫ3 (group by time) mixed model with repeated measures on
eyes open on the ground and on foam; each weight shift was
the last factor. The proportion of falls scores were also ana-
held at the limit of stability (achieved with the ankle as ful-
lyzed with a 2ϫ3 (group by time) mixed model with repeated
crum) for 5 seconds. During weight shifting, participants gently
swayed to their limit of stability, leaning as far as they could
Muscle strength analyses.
without falling and keeping the ankle, hip, and shoulders in a
ance analyses, an attempt was made to use the same covariates
line. Participants swayed toward 1 of 4 imaginary targets
in the analyses of muscle strength. A regression was performed
(forward, backward, left, right), and each position was held for
on the 5 covariates of age of diagnosis with PD, duration of
disease, ratio of pretreatment muscle strength to body weight,
Compliance.
Participants in the balance group attended
ratio of hamstring muscle strength to quadriceps muscle
91.8% of all training sessions, and those in the combined group
strength, and pretreatment number of falls on EquiTest condi-
attended 89.4% of all sessions. During the training period, 1
tions 4 through 6. The coefficients for each of these variables
participant in the combined group developed an acute urinary
with the dependent variables of knee extension, knee flexion,
tract infection, requiring lengthy hospitalization. This occurred
and ankle plantarflexion muscle strength for pretreatment, post-
after 7 weeks of training. Another combined group participant
treatment, and follow-up treatment tests were low, however,
was rediagnosed as not having IPD by his neurologist. This
ranging from Ϫ.38 to .35 with most near zero. Thus, the
occurred after 5 weeks of training. Data for these 2 participants
analysis of muscle strength was repeated without covariates.
were eliminated from all statistical analyses. A third participant
Therefore, the design for the analysis of variance (ANOVA)
in the combined group reported a minor inguinal hernia after 3
for muscle strength was a 2ϫ3ϫ3 mixed model (groups by
days—presumably as a result of strength testing during base-
time of pre, post, follow-up by muscles of quadriceps, ham-
line evaluation—and chose not to perform resistance training
strings, gastrocnemius). For this design there were 2 repeated-
or strength testing. This participant continued with balance
training and completed all balance testing in a timely manner.
When the F ratios were significant, post hoc comparisons of
Data from this participant were included in balance group data
the means were analyzed with the Tukey honestly significant
analyses for latency to fall and balance analysis, but not in
difference (HSD) multiple-comparison test. Relations among
strength analyses. Data indicate that the protest scores of these
the covariates were analyzed pairwise with the Pearson corre-
3 individuals were comparable to those of the other subjects.
lation coefficient. Additionally, we compared baseline charac-
One participant in the balance group had minor outpatient
teristics by using 1-way ANOVA. All results are presented as
surgery in 1 eye after 9 weeks of training. This participant
means and standard errors of the mean (SEMs). A 2-sided P
chose not to complete any post or follow-up muscle strength
value of .05 or less was considered statistically significant.
measures but was able to complete all post and follow-upbalance testing in a timely manner. Data Analysis Baseline
All data were analyzed with SPSS.d We used 4 primary
Baseline characteristics of the subjects in the combined and
analyses, 1 each for balance scores, latency to fall scores,
balance groups did not differ significantly (table 1). The vari-
proportion of falls scores, and muscle strength scores.
ances of these variables also did not differ significantly for the
Balance analyses.
groups. In addition, before training started, the dependent vari-
scores used the analysis of covariance (ANCOVA) model for
ables did not differ significantly for the 2 groups, and the
repeated measures. Table 1 lists and defines the covariates and
variances also did not differ significantly.
the dependent variable and provides summary statistics. AN-COVA was deemed important to use based on prior analy-ses6,41 that showed high levels of variability in persons with
Effect of Training on Summary Balance Score
IPD on balance and strength measures. Covariates believed to
Analysis of balance scores for 9 participants from the balance
be important in the current analysis include the age at onset of
group and 6 participants from the combined group provides evi-
PD, the duration of PD, the number of falls in preexperiment
dence of the effects of training on the summed, averaged scores
balance tests, and subject’s initial muscle strength levels. We
of EquiTest conditions 4 though 6. There was a main effect for
selected these variables because empirical evidence shows: (1)
group (F ϭ14.16, Pϭ.006; effect sizeϭ.64; observed pow-
rapid deterioration of balance in patients who are older at onset
erϭ.91 [91% power is large]). Thus, when the balance scores were
of PD,52 (2) frequent falls on EquiTest conditions 4 through 6
collapsed over time (pretreatment, posttreatment, follow-up treat-
in patients with limited lower-extremity muscle strength,41 and
ment), the combined group had a significantly higher mean on the
(3) longer duration of PD associated with falling.22,29 The
EquiTest (mean Ϯ SEM, 69.28Ϯ4.7) than did the balance
covariates correlated highly, from Ϫ.93 to .56, with the depen-
group (mean, 55.9Ϯ4.3). The combination of balance and
dent variable for pre, post, and follow-up balance scores and
resistance training improved balance scores of persons with PD
there were no significant differences between the means of the
significantly more than did balance training alone.
covariates for the balance and combined groups.
The time effect for the training was not statistically signifi-
For the analysis of SOT summary balance scores, there were
cant; however, the pooled data from both groups showed a
2 groups (balance, combined) and 3 sets of measurements
trend (Pϭ.063) for change in balance scores over time, with a
Arch Phys Med Rehabil Vol 84, August 2003 STRENGTH AND BALANCE IN PARKINSON’S DISEASE, Hirsch Table 3: Covariate Coefficients for EquiTest ANCOVA
small effect size of .18. For both groups, the means of thesummed, averaged, balance scores for EquiTest conditions 4through 6 increased after training (balance pretreatment mean,52.8Ϯ8.2; balance posttreatment mean, 60.1Ϯ3.4; combined
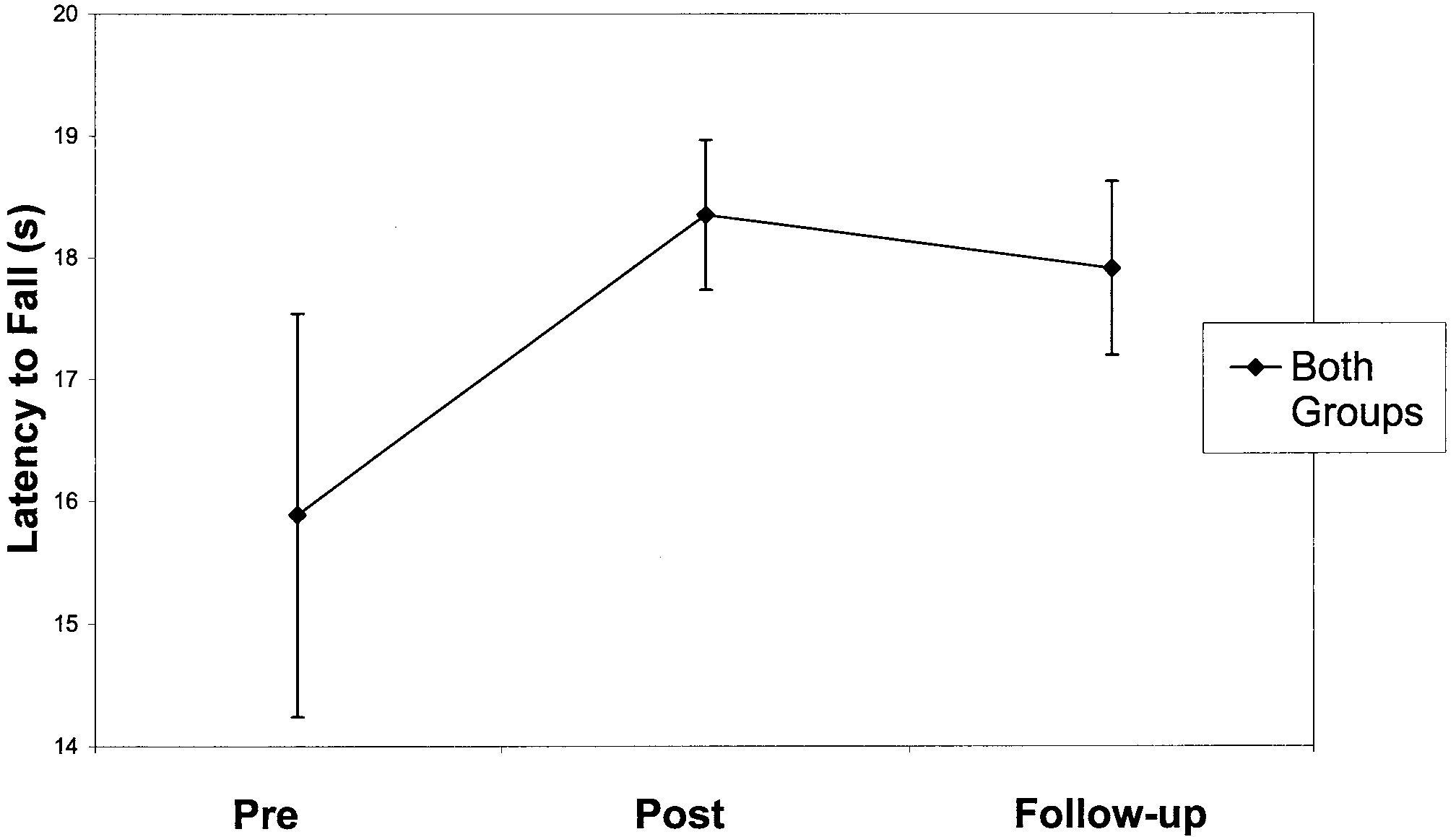
Fig 1. Latency to fall effect over the pretreatment, posttreatment,
pretreatment mean, 59.0Ϯ8.5; combined posttreatment mean,
and follow-up tests for both groups. Values refer to average latency to fall for summary balance conditions (SOT conditions 4 – 6 aver-
75.1Ϯ3.1). Four weeks after the training ended, the mean for
aged). Error bars indicate SEM.
the balance group declined to near pretreatment levels (mean,54.8Ϯ5.2), whereas scores for the combined group declinedmoderately (mean, 73.9Ϯ3.6).
Table 3 reports the ANCOVA results, showing a statistically
testing periods, the combined group was significantly higher in
significant relationship between the covariates and the dependent
strength (mean, 43.8Ϯ4.2kg) than the balance group (mean,
30.4Ϯ2.9kg). There was also a significant main effect for time
indicating that the covariates were significantly related to the
ϭ151.22, PϽ.001; effect sizeϭ.93 [a very large effect
summary EquiTest score. The relationship between the pre-
size]; observed powerϭ100%). Posttreatment strength was sig-
treatment number of falls for the participants was significantly
nificantly higher (mean, 40.4Ϯ3.7kg) than pretreatment
related to the EquiTest summary balance scores (PϽ.001). The
strength (mean, 31.0Ϯ2.3kg) and follow-up treatment strength
other covariates were not statistically significant and thus there
(mean, 38.3Ϯ3.4kg). The last significant main effect was mus-
was statistical evidence that they were not strongly related to
22.67, PϽ.001; effect sizeϭ.67; observed
the summary EquiTest scores in these participants. However,
powerϭ100%). The quadriceps was significantly stronger (mean,42.8Ϯ3.4kg) than the hamstrings (mean, 31.5Ϯ2.6kg) and the
because they all correlated moderately to highly with the Equi-
gastrocnemius (mean, 35.4Ϯ3.5kg), whereas the hamstrings and
Test balance score, all were used as covariates.
gastrocnemius did not differ significantly from one another.
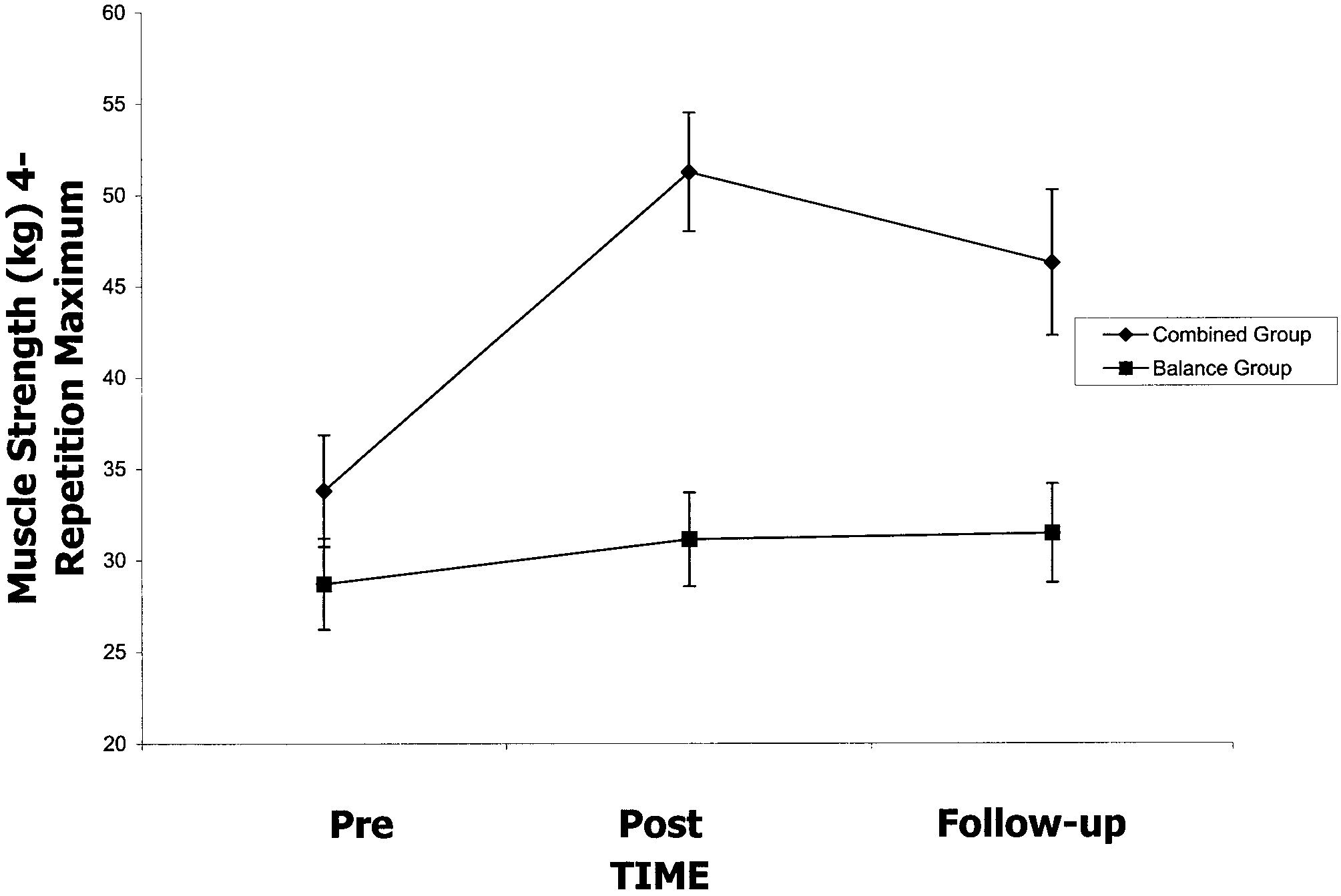
The group by time interaction was significant (F
Effect of Training on Latency to Fall and Proportion of Pϭ.001; effect sizeϭ.88 [a very large effect]; observed
Trials Resulting in Falls
powerϭ100%; fig 2, table 5). The combined group was signif-
The data provide evidence that training affects the average
icantly higher in average strength of the 3 muscle groups than
number of seconds a participant could balance and the percent-
the balance group at posttreatment and follow-up testing. Thebalance group had a modest and statistically significant im-
age of trials resulting in falls. Nine participants from the
provement (9%) in muscle strength from pretreatment to
balance group and 6 participants from the combined group
follow-up treatment testing (Tukey HSDϭ6.068 for all com-
were included in these analyses. For latency to fall, there was
parisons). By using the strength score, there was a 52% im-
ϭ4.25, Pϭ.025; effect sizeϭ.25;
provement from pre- to posttreatment for the combined group.
observed powerϭ69%; see fig 1, table 4), showing a significant
The combined group lost 10% of its posttreatment strength
(15%) change in the latency to fall data from pretreatment to
score (mean, 50.8kg posttreatment vs 45.9kg follow-up treat-
posttreatment testing (Tukey HSDϭ2.214) for both groups.
ment), which was a statistically significant decline, but its
Latency to fall was significantly longer after the treatment thanbefore in both groups (seconds to fall pretreatment, mean,15.89Ϯ1.10; posttreatment mean, 18.35Ϯ0.25). At follow-uptesting, participants in both groups showed a modest, but not
Table 4: Latency to Fall and Percentage of Trials
significant, decline in latency to fall (mean change, .44s). For
Resulting in Falls
the proportion of trials resulting in falls, there was a significant
ϭ4.67, Pϭ.018; effect sizeϭ.26; observed
powerϭ74%), showing a reduction in the percentage of trials
resulting in falls from pretreatment (mean, 32.86Ϯ8.04) to
posttreatment (mean, 12.77Ϯ4.07). There were no other sig-
Effect of Training on Muscle Strength
Seven participants from the balance group and 6 participants
from the combined group were included in this analysis. There
were 3 significant main effects for the strength analysis; the
Abbreviations: Latency to fall, average time to fall (in seconds) onSOT conditions 4 – 6; Percentage of trials resulting in falls, total
number of trials (conditions 4 – 6) divided by number of trials result-
effect sizeϭ.40; observed powerϭ69%). Over the combined
Arch Phys Med Rehabil Vol 84, August 2003 STRENGTH AND BALANCE IN PARKINSON’S DISEASE, Hirsch Fig 3. The time by muscle group interaction for strength. Values refer to changes in muscle strength (kg) on 4-repetition maximum Fig 2. The group and time interaction for strength. Values refer to test for knee extension (quadriceps), knee flexion (hamstring), and muscle strength (kg) on 4-repetition maximum test for 3 muscle ankle plantarflexion (gastrocnemius/soleus). Error bars indicate groups combined for the combined and balance groups. Error bars indicate SEM.
follow-up treatment strength score was still significantly higherthan pretreatment.
There were 4 main findings: (1) balance training improved
There was a time by muscle group interaction (F
performance on the summary balance measure and this effect
Pϭ.001; fig 3). One can observe the main finding from this
was enhanced by concurrent resistance training, (2) training
interaction by noticing that the pattern of results was similar for
increased latency to falling and reduced the percentage of trials
the quadriceps (knee extension) and hamstring (knee flexion)
resulting in falls, and this effect persisted for at least 4 weeks,
muscle groups. Both of these muscle groups improved signif-
(3) muscle strength was increased and this change also per-
icantly from pre- to posttesting and remained the same for
sisted for at least 4 weeks, and (4) in comparison to our earlier
follow-up tests (no significant change, Tukey HSDϭ6.69 for
work,6 we have extended our findings to show that balance and
all comparisons). For the gastrocnemius, a steeper change and
resistance-training benefits persist for 4 weeks even if partici-
significant improvement came about from pre- to posttests,
pants do not maintain their level of training.
with significant decline in muscle strength after 4 weeks of
Effect of Training on Muscle Strength
detraining. The interaction occurs with time and muscle groupbecause the pattern of changes over time for the gastrocnemius
High-intensity resistance training increased lower-extremity
is different from the other 2 muscle groups.
muscle strength by 52% with combined training and 9% with
There was a triple interaction among the 3 factors of group,
balance-only training. Our findings extend observations by
Fisher et al53 who reported similar increases in lower-extremity
tion is a combination of the last 2 interactions explained above,
muscle strength among 18 nursing home residents—2 of whom
and a third pattern of results among the 2 factors of group and
had PD. The effect of resistance training has rarely been
muscles. Post hoc analyses (Tukey HSDϭ17.83) showed that
studied in persons with PD and the results of 1 study54 using
both groups haved significantly less strength in their knee
rubber bands to improve muscle strength showed no improve-
flexor muscles than in their knee extensors and strength in
ment in knee extension strength. This lack of improvement
ankle plantarflexion was not significantly higher than knee
may be due to inappropriate exercise design, high variability
between repeated measures, or low exercise intensity. Higher-intensity resistance training has generally improved muscle
DISCUSSION
strength in older adults,18-20 so this failure may be attributed to
We examined the effect of balance training and high-inten-
sity resistance training on balance in 15 persons with IPD.
Muscle strength also increased significantly in the balance
group. Muscle strength is rarely tested in balance trainingstudies. Judge et al55 compared changes in muscle strength
Table 5: Strength
between balance training and combined resistance and balancetraining in healthy older adults, using foam-based balance
training and periodic 4-repetition-maximum strength tests sim-ilar to ours; they reported no change in muscle strength from
balance training alone. That study, unlike ours, did not test
muscle strength every 2 weeks to ensure that training intensity
was maintained at 80% of a 4-repetition maximum.55 Because
muscle strength was tested in both groups every 2 weeks, a
learning effect may account for the small (9%) but statistically
significant increase in muscle strength in the balance trained
group. It is also possible that the balance exercises themselves
contributed to increases in muscle strength, greater resistanceto fatigue, or greater tolerance to muscle discomfort during
NOTE. Values are mean Ϯ SEM, are in kilograms, and were recorded
Arch Phys Med Rehabil Vol 84, August 2003 STRENGTH AND BALANCE IN PARKINSON’S DISEASE, Hirsch
The effect of detraining on muscle strength is rarely reported
In persons with PD, muscle strength at the ankle and knee
in resistance-training studies of healthy or pathologic popula-
appears to affect performance on the SOT,6,22,41 which may
tions. In young healthy individuals trained using concentric and
partly explain why those in the combined group were able to
eccentric high-intensity resistance exercises for the quadriceps
stand with less sway than those in the balance group. Increased
and hamstring muscle groups for 16 to 24 weeks, detraining
steadiness of the knee may have resulted in higher summary
causes substantial decreases in maximum force production
balance scores.41 Apparently, greater muscle strength has no
after 8 to 12 weeks of inactivity.56 In our study, the combined
differential effect on latency to fall or the percentage of trials
group lost 10% of its average muscle strength, with the major-
resulting in falls; however, our results indicate higher levels of
ity of the loss in the gastrocnemius; however, muscle strength
ankle strength, knee extension, and knee flexion strength may
did not decrease to pretreatment levels after 1 month of de-
result in less sway. These effects on balance performance
training. In the gastrocnemius, there was greater improvement
indicate the benefit of training in our participants.
in strength and greater loss compared with the quadriceps and
The effect of detraining on balance performance is rarely
hamstring muscles (fig 3). Our results suggest that periods of
reported in the literature. For persons in our study, the effect of
inactivity lasting approximately 1 month did not result in
detraining appears to be negligible for up to 4 weeks. A
substantial loss of training effect for knee flexors and extensors
retrospective study49 reported sustained improvements in equi-
in persons with PD. In another study,53 chronically ill persons
librium associated with balance training in 85% of patients
living in a nursing home (among them, 1 subject with PD)
with chronic vestibular dysfunction. Future research should
maintained lower-body muscle strength gains for up to 4
focus more heavily on the effect of detraining on balance and
months after 10 weeks of high-intensity resistance training for
muscle strength and on the possibility that improved function
the knee extensors. This is important because older adults with
permits self-generated practice during activities of daily living.
PD may be prone to interruptions in their exercise programs
The evidence presented here is preliminary and does not
because of frequent travel, chronic illness, hospital admissions,
address the mechanisms involved in balance control in persons
and changes in medication. As long as these interruptions are
with PD, nor do the data permit any conclusive statements
not too extensive, they are unlikely to completely reverse the
regarding how change in function can result from high-inten-
sity resistance and/or balance training. We combined EquiTest
Although we did not assess the mechanisms responsible for
conditions 4 through 6 into a summary score because data for
increased muscle strength, gains in muscle strength in our
these conditions were highly correlated and we cannot make
participants may be because of improved neural activation, a
any conclusive statements regarding changes in individual test
generalized effect of resistive training or to changes in the
conditions; however, excessive sway and falls of PD patients
intrinsic contractile characteristics of muscle.57 Quadriceps,
during EquiTest conditions 5 and 6 have consistently been
hamstring, and gastrocnemius muscle strength differed signif-
reported.6,41 This shows that when somatosensory information
icantly from pretreatment values after 4 weeks of detraining,
is reduced by placing patients on foam or standing on a
indicating persistence of nonhypertrophic-related adaptions to
sway-referenced support surface, persons with PD are less able
high-intensity resistance training among those in the combined
to compensate by using visual or vestibular feedback. Perhaps
group. It is possible that the participants were able to maintain
the reason they cannot apply corrective torque about the ankle
muscle strength by engaging in more complex and extended
and knee during these conditions is because of lack of muscle
movements in their everyday repertoires, self-regulated by
strength, which can be corrected, in part, by a resistance or
improvements in balance and reduced fear of falling.
balance training program. Another reason why people with PDmight sway more with reduced or misleading somatosensoryankle joint feedback during EquiTest conditions 4 through 6 is
Effect of Training on Balance
because of an impaired transmission of motor programming
Training had 3 effects on balance: (1) training increased the
from the basal ganglia to brainstem and spinal cord, as sug-
latency to fall by 15% and the effect of detraining was minimal
gested by Garcia-Rill.58 It is unclear how balance and/or resis-
(2%); (2) training reduced the percentage of trials resulting in
tance training might serve to ameliorate this. However, it may
falls by 20% from pretreatment to posttreatment and this effect
be that balance training serves to increase frequency and in-
remained unchanged for 4 weeks; and (3) participation in the
tensity of neuromotor pathways in balance control facilitating
combined group improved the ability to maintain equilibrium,
neuronal transmission and muscle contraction. Thus, motor
(ie, sway less) during destabilizing conditions.
programs used for balance adaptation can be better tuned or
Our study indicates that a generalized effect of balance
preset so to enhance transmission and execution.
and/or resistance training is reduction of latency to fall in
We want to emphasize that the SOT portion of the EquiTest
persons with PD. Our results are consistent with those of Cass
quantifies only limited aspects of a person’s balance control.
et al,44 who reported increased latency to fall in 90% of patients
We used the EquiTest in this study because of its objectivity
on the 2 most difficult test conditions (EquiTest conditions 5
and its potential to assess responses to balance training among
and 6) in response to resistance and balance training, and those
persons with PD.6,41 The results might have differed and a more
of Horak et al,50 who reported increased single-leg stance time
complete picture of change over time might have been docu-
mented if we had used more functional balance tests.59
On the summary balance score measure, the combined group
Maximizing adherence and minimizing injury is an obvious
performed significantly better than the balance group. Training
concern. The injury and adherence rates in our study were
had a greater effect on the combined group, and this is reflected
similar to those in other studies with healthy older adults. We
in a higher summary balance score and less sway on the 3 most
used a conservative test of muscle strength because of the high
difficult balance conditions among participants in the combined
incidence of musculoskeletal injury (20%) reported in previous
group. Szturm et al51 used foam-based balance exercises in
studies utilizing a 1-repetition-maximum strength testing pro-
persons with chronic peripheral vestibular function. They re-
tocol.55 The greater incidence of dropouts in the combined
ported balance training reduced sway and falls on EquiTest
group suggests careful attention to exercise and form are im-
conditions 4 through 6. Presumably reductions in falls would
portant during resistance training and strength testing in per-
reduce latency to fall but this was not reported.51
sons with PD, as it is in all adults. Drop-out rates in the
Arch Phys Med Rehabil Vol 84, August 2003 STRENGTH AND BALANCE IN PARKINSON’S DISEASE, Hirsch
combined group may have been due to the initial high intensity;
motor cortex of adult squirrel monkeys. J Neurosci 1996;16:785-
lower intensities with a more gradual progression to higher
intensity training or beginning training with balance training
11. Jones TA, Kleim JA, Greenough WT. Synaptogenesis and den-
only and then gradually adding resistance training might have
dritic growth in the cortex opposite unilateral sensorimotor cortex
prevented the injury in the combined group.
damage in adult rats: a quantitive electron microscopic examina-
A limitation of our study is lack of a control group. Although
balance generally does not improve spontaneously and muscle
12. Johansson BB, Ohlsson A. Environment, social interaction, and
physical activity as determinants of functional outcome after ce-
strength declines over time in persons with PD,6 the present
rebral infarction in the rat. Exp Neurol 1996;139:322-7.
data suggest it is important to include untreated patients as a
13. Nudo RJ, Wise BM, SiFuentes F, Milliken GW. Neural substrates
control group to further study the effects of resistance and
for the effects of rehabilitative training on motor recovery after
balance training and detraining. Another limitation is sample
ischemic infarct. Science 1996;272:1791-4.
size and short training period. Group training requires extra
14. Kempermann G, Gage FH. New nerve cells for the adult brain. Sci
attention to safety and biomechanical technique during exercise
from many trained assistants, which prevented us from using a
15. Gould E, Beylin A, Tanapat P, Reeves A, Shors TJ. Learning
larger sample size. The extent to which balance can be altered
enhances adult neurogenesis in the hippocampal formation. Nat
through longitudinal resistance and balance programs is un-
16. Van Prag H, Kempermann G, Gage FH. Running increases cell
clear because of the small sample size and warrants further
proliferation and neurogenesis in the adult mouse dentate gyrus.
investigation with larger study samples.
17. Tillerson JL, Castro SL, Zigmond MJ, Schallert T. Motor reha-
CONCLUSION
bilitation of forelimb use in a unilateral 6-OHDA rat model ofParkinson’s disease. Soc Neurosci Abstr 1998;672:1720.
Maintaining functional ability and preventing falls in old age
18. Buchner DM, Cress ME, Wagner EH, de Lateur BJ, Price R,
are determined, in part, by maintaining some optimal level of
Abrass IB. The Seattle FICSIT/MoveIt study: the effect of exer-
body strength. Although further study is necessary to establish
cise on gait and balance in older adults. J Am Geriatr Soc 1993;
the relationship between muscle strength and balance in PD,
we hypothesize that a resistance and balance training program,
19. Fiatarone MA, O’Neill EF, Ryan ND, et al. Exercise training and
conducted under proper supervision, is enjoyable, effective,
nutritional supplementation for physical frailty in very elderly
and a relatively safe way to improve muscle strength and
people. N Engl J Med 1994;330:1769-75.
balance in persons with PD who fall during dynamic posturog-
20. Tinetti ME, Baker DI, McAvay G, et al. A multifactorial inter-
raphy and may reduce the likelihood of falls during balance
vention to reduce the risk of falling among elderly people living inthe community. N Engl J Med 1994;331:821-7.
assessment. We further postulate that a resistance and balance
21. Wolf S, Kutzer N, Green R, McNeely E. The Atlanta FICSIT
training program may reduce fall risk at home and in the
study: two exercise interventions to reduce frailty in elders. J Am
community with enhanced likelihood of long-term independent
22. Wolfson L, Judge J, Whipple R, King M. Strength is a major
factor in balance, gait, and the occurence of falls. J Gerontol A
Acknowledgments:
We acknowledge Elton Scott, PhD, for sta-
tistical advice, and Helen Ghiradella, PhD, Helmut V Hirsch, PhD, and
23. Aita JF. Why patients with Parkinson’s disease fall. JAMA 1982;
Timothy Schallert, PhD, for reading preliminary versions and for
24. Grisso JA, Kelsey JL, Strom BL, et al. Risk factors for falls as a
cause of hip fractures in women. N Engl J Med 1991;323:1326-31. References
25. Jankovic J. Pathophysiology and clinical assessment of motor
1. Kish SJ, Shannnak K, Hornykiewcz O. Uneven pattern of dopa-
symptoms in Parkinson’s disease. In: Koller WC, editor. Hand-
mine loss in the striatum of patients with idiopathic Parkinson’s
book of Parkinson’s disease. New York: Marcel Dekker; 1987. p
disease. N Engl J Med 1988;318:376-80.
2. Olanow CW, Koller WC. An algorithm (decision tree) for the
26. Klawans HL, Topel JL. Parkinsonism as a falling sickness. JAMA
management of Parkinson’s disease. Neurology 1998;50 Suppl
27. Koller WC, Glatt S, Vetere-Overfield B, Hassanein R. Falls and
3. American Academy of Neurology. Assessment: posturography.
Parkinson’s disease. Clin Neuropharmacol 1989;12:98-105.
28. Nevitt MC, Cummings SR, Kidd SR, Black D. Risk factors for
4. Comella CL, Stebbins GT, Brown-Toms N, Goetz CG. Physical
recurrent non-syncopal falls: a prospective study. JAMA 1989;
therapy and Parkinson’s disease: a controlled clinical trial. Neu-
29. Schenkman M, Butler RB. A model for multisystem evaluation
5. Palmer SS, Mortimer JA, Webster DD, Bistevins R. Exercise
treatment of individuals with Parkinson’s disease. Phys Ther
therapy for Parkinson’s disease. Arch Phys Med Rehabil 1986;
30. Johnell O, Melton LJ 3rd, Atkinson EJ, O’Fallon WM, Kurland
6. Toole T, Hirsch MA, Forkink A, Lehman DA, Maitland CG. The
LT. Fracture risk in patients with parkinsonism: a population
effects of a balance and strength training program on Parkinson-
based study in Olmsted County, Minnesota. Age Ageing 1992;21:
ism: a preliminary study. J Neurol Rehabil 2000;14:165-74.
7. Jones TA, Schallert T. Use-dependent growth of pyramidal neu-
31. Glendinning DS, Enoka RM. Motor unit behavior in Parkinson’s
rons after neocortical damage. J Neurosci 1994;14:2140-52.
8. Schallert T, Jones TA. Exhuberant neuronal growth after brain
32. Koller WC, Kase S. Muscle strength testing in Parkinson’s dis-
damage in adult rats: the essential role of behavioral experience.
J Neural Transplant Plastic 1993;4:193-8.
33. Nogaki H, Fukusako T, Sasabe F, Negoro K, Morimatsu M.
9. Greenough WT, Fass B, DeVoogd T. The influence of experience
Muscle strength in early Parkinson’s disease. Mov Disord 1995;
on recovery following brain damage in rodents: hypotheses based
on developmental research. In: Walsh R, Greenough W, editors.
34. Pedersen SW, Oberg B. Dynamic strength in Parkinson’s disease.
Environments as therapy for brain dysfunction. New York: Ple-
35. Saltin B, Landin S. Work capacity, muscle strength, and SDH
10. Nudo RJ, Milliken GW, Jenkins WM, Merzenich MM. Use-
activity in both legs of hemiparetic and patients with Parkinson’s
dependent alterations of movement representations in primary
disease. Scand J Clin Lab Invest 1975;35:531-8. Arch Phys Med Rehabil Vol 84, August 2003 STRENGTH AND BALANCE IN PARKINSON’S DISEASE, Hirsch
36. Yanagawa S, Shindo M, Yanagisawa N. Muscular weakness in
48. Monsell EM, Furman JM, Herdman SJ, Konrad HR, Shepard NT.
Parkinson’s disease. In: Streifler MB, Korczyn AD, Melamed E,
Computerized dynamic platform posturography. Otolaryngol
Youdim MB, editors. Advances in neurology: Parkinson’s dis-
ease—anatomy, pathology, and therapy. Vol 53. New York:
49. Smith-Wheelock M, Shepard NT, Telian SA. Physical therapy
program for vestibular rehabilitation. Am J Otol 1991;12:218-25.
37. Grimby L, Hannerz L. Disturbance in the voluntary recruitment
50. Horak FB, Jones-Rycewicz C, Black FO, Shumway-Cook A.
order of anterior tibial motor units in bradykinesia of parkinson-
Effect of vestibular rehabilitation on dizziness and imbalance.
ism. J Neurol Neurosurg Psychiatry 1974;37:47-54.
Otolaryngol Head Neck Surg 1992;106:175-80.
51. Szturm T, Ireland DJ, Lessing-Turner M. Comparison of different
38. Hayashi A, Kagamihara Y, Nakajima Y, Narabayashi H, Okuma
exercise programs in the rehabilitation of patients with chronic
Y, Tanaka R. Disorder in reciprocal innervation upon initiation of
peripheral vestibular dysfunction. J Vestib Res 1994;4:461-79.
voluntary movement in patients with Parkinson’s disease. Exp
52. Heley MA, Morris JG, Reid WG, et al. Age at onset: the major
determinant outcome in Parkinson’s disease. Acta Neurol Scand
39. Corocos DM, Chen CM, Quinn NP, McAuley J, Rothwell JC.
Strength in Parkinson’s disease: relationship to rate of force gen-
53. Fisher NM, Pendergast DR, Calkins E. Muscle rehabilitation in
eration and clinical status. Ann Neurol 1996;36:79-88.
impaired elderly nursing home residents. Arch Phys Med Rehabil
40. Jordan N, Sagar HJ, Cooper JA. A component analysis of the
generation and release of isometric force in Parkinson’s disease.
54. Pedersen SW, Insulaner OA, Vretman M. Group training in Par-
J Neurol Neurosurg Psychiatry 1992;55:572-6.
kinsonism: quantitative measurements of treatment. Scand J Re-
41. Toole T, Park S, Hirsch M, Lehman D, Maitland G. The multi-
component nature of equilibrium in persons with parkinsonism: a
55. Judge JP, Whipple RH, Wolfson LI. Effects of resistive and
regression approach. J Neural Transm Gen Sect 1996;103:561-80.
balance exercises on isokinetic strength in older persons. J Am
42. de Lateur BJ, Lehmann JF. Strengthening exercise. In: Leek JC,
Gershwin ME, Fowler WM, editors. Principles of physical med-
56. Hakkinen K, Komi PV, Tesch PA. Effect of combined concentric
icine and rehabilitation in musculoskeletal diseases. Orlando:
and eccentric strength training and detraining on force-time, mus-
Grune & Stratton; 1986. p 25-60.
cle fibre, and metabolic characteristics of leg extensor muscles.
43. DeLorme TL. Restoration of muscle power by heavy-resistance
57. Moritani T, deVries HA. Neural factors versus hypertrophy in the
exercises. J Bone Joint Surg 1945;27:645-67.
time course of muscle strength gain. Am J Phys Med 1979;58:
44. Cass SP, Borello-France D, Furman JM. Functional outcome of
vestibular rehabilitation in patients with abnormal sensory-orga-
58. Garcia-Rill E. The basal ganglia and the locomotor regions. Brain
nization testing. Am J Otol 1996;17:581-94.
45. Ford-Smith CD, Wyman JF, Elswick JF, Fernandez T, Newton
59. Berg K. Balance and its measure in the elderly: a review. Phys-
RA. Test-retest reliability of the sensory organization test in
noninstitutionalized older adults. Arch Phys Med Rehabil 1995;76:77-81. Suppliers
46. Hamid MA, Hughes GB, Kinney SE. Specificity and sensitivity
a. NeuroCom International Inc, 9570 SE Lawnfield Rd, Clackamas,
of dynamic posturography. Acta Otolaryngol (Stockh) 1991;481
b. Nautilus Group Inc, 1400 NE 136th Ave, Vancouver, WA 98684.
47. Minor LB. Utility of posturography in management of selected
c. Jo-Ann Stores Inc, 5555 Darrow Rd, Hudson, OH 44236.
conditions that cause dizzyness. Am J Otol 1997;18:113-5.
d. SPSS Inc, 233 S Wacker Dr, 11th F1, Chicago, IL 60606. Arch Phys Med Rehabil Vol 84, August 2003
In collaborazione con U.O.C. UROLOGIA tel. 0426/940334—Fax. 0426/940337 Storz Italia UOC UROLOGIA Coloplast RESPONSABILE DEL PROGETTO Manganotti snc Dr. Agostino Meneghini U.O.C. di UROLOGIA SEGRETERIA SCIENTIFICA Evento formativo riservato a 15 specialisti Dr. Agostino Meneghini in Urologia, durata 2 giorni, svolto U.O.C.
 STRENGTH AND BALANCE IN PARKINSON’S DISEASE, Hirsch
STRENGTH AND BALANCE IN PARKINSON’S DISEASE, Hirsch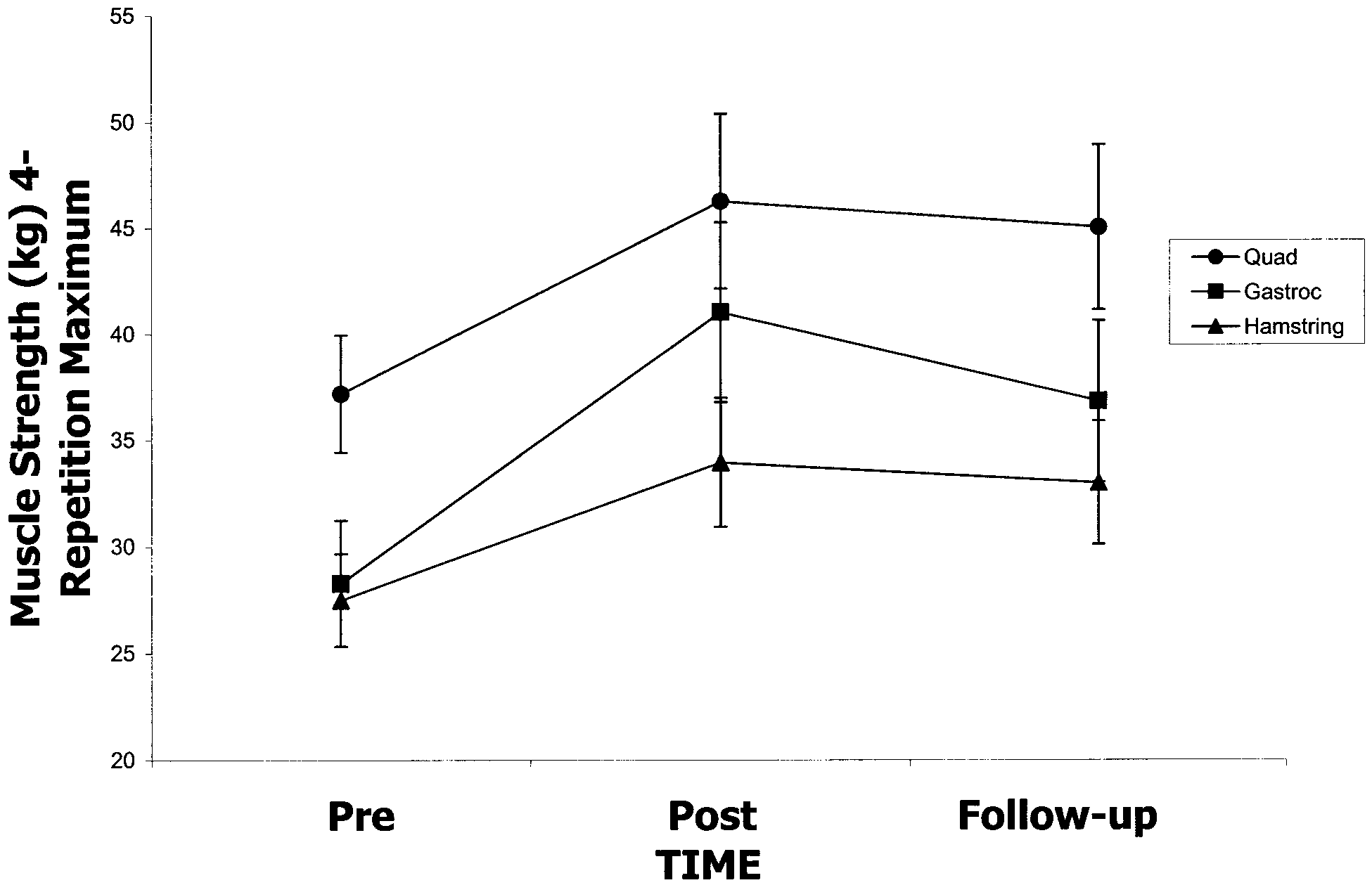
 STRENGTH AND BALANCE IN PARKINSON’S DISEASE, Hirsch
STRENGTH AND BALANCE IN PARKINSON’S DISEASE, Hirsch