Psychoneuroendocrinology 28 (2003) 39–53
syndrome & premenstrual dysphoric disorder
UCLA School of Medicine, Department of Obstetrics and Gynecology, Center for the Health Sciences,Room 27-165, 10833 Le Conte Avenue, Los Angeles, CA 90095-1740, USAAbstract
Severe premenstrual syndrome (PMS) and, more recently, premenstrual dysphoric disorder
(PMDD) have been studied extensively over the last 20 years. The defining criteria for diag-nosis of the disorders according to the American College of Obstetricians & Gynecologists(ACOG) include at least one moderate to severe mood symptom and one physical symptomfor the diagnosis of PMS and by DSM IV criteria a total of 5 symptoms with 1 severe moodsymptom for the diagnosis of PMDD. There must be functional impairment attributed to thesymptoms. The symptoms must be present for one to two weeks premenstrually with reliefby day 4 of menses and should be documented prospectively for at least two cycles using adaily rating form. Nonpharmacologic management with some evidence for efficacy includecognitive behavioral relaxation therapy, aerobic exercise, as well as calcium, magnesium, vit-amin B6 L-tryptophan supplementation or a complex carbohydrate drink. Pharmacologic man-agement with at least ten randomized controlled trials to support efficacy include selectiveserotonin reuptake inhibitors administered daily or premenstrually and serotonergic tricyclicantidepressants. Anxiolytics and potassium sparing diuretics have demonstrated mixed resultsin the literature. Hormonal therapy is geared towards producing anovulation. There is goodclinical evidence for GnRH analogs with addback hormonal therapy, danocrine, and estradiolimplants or patches with progestin to protect the endometrium. Oral contraceptive pills preventovulation and should be effective for the treatment of PMS/PMDD. However, limited evidencedoes not support efficacy for oral contraceptive agents containing progestins derived from 19-nortestosterone. The combination of the estrogen and progestin may produce symptoms similarto PMS, such as water retention and irritability. There is preliminary evidence that a new oralcontraceptive pill containing low-dose estrogen and the progestin drospirenone, a spironolac-tone analog, instead of a 19-nortestosterone derivative can reduce symptoms of water retentionand other side effects related to estrogen excess. The studies are in progress, however, prelimi-
∗ Tel.: +1-310-794-1981; fax: +1-310-206-3670. E-mail address: [email protected] (A. Rapkin).
0306-4530/$ - see front matter 2003 Elsevier Ltd. All rights reserved. doi:10.1016/S0306-4530(03)00096-9
A. Rapkin / Psychoneuroendocrinology 28 (2003) 39–53
nary evidence suggests that the drospirenone-containing pill called Yasmin may be effectivethe treatment of PMDD.
2003 Elsevier Ltd. All rights reserved. Keywords: Premenstrual syndrome; Premenstrual dysphoric disorder; Hormones; Oral contraceptives;Drospirenone
Tempestuous premenstrual behavior was described by Hippocrates, who attributed
the symptoms to agitated blood seeking escape from the womb. However, it was inthe 1930’s that the premenstrual tension syndrome was first delineated, possiblycoinciding with the entry of women into the workforce. In the 1950’s, the termPremenstrual Syndrome (PMS) was applied to the physical and psychological symp-toms occurring for up to 2 weeks prior to menses with relief seen after the onset ofthe menstrual period. In the 1990’s, criteria were included in the Appendix of theDiagnostic and Statistical Manual for Mental Disorders, 3rd and then 4th edition,describing Late Luteal Phase Dysphoric Disorder (LLPDD) and finally PremenstrualDysphoric Disorder (PMDD), a particularly severe form of Premenstrual Syndromewith an emphasis on the affective symptoms (DSM-IV, 1994). In April, 2000 theAmerican College of Obstetricians and Gynecologists published a Practice Bulletinon the topic of PMS, that included criteria for diagnosis and recommendations forthe treatment of clinically significant Premenstrual Syndrome
The development of evidence-based guidelines for the treatment of severe
PMS/PMDD has been hampered for various reasons. Studies investigating the treat-ment of PMS have included subjects with a variety of different premenstrual symp-toms. Often the inclusion and exclusion criteria differed among studies. Earlier stud-ies also suffered from the use of retrospective recall as opposed to prospective dailyrecording to confirm the diagnosis of PMS. Retrospective recall correlates with pro-spective daily recording of symptoms in only 50% of the cases Even in the setting of well-defined diagnostic criteria, such as currently exist forPMS/PMDD, the methodology employed to rule out underlying or coexisting psychi-atric disorders and the specific daily rating scales utilized to record symptomatologyvary among studies. Many of the early studies were not placebo controlled or sufferedfrom a high placebo response rate. The latter outcome is often associated with evalu-ation of a large number of symptoms of mild to moderate severity. Furthermore,because the PMS patients studied in clinical trials may differ from the populationof women suffering from PMS/PMDD as a whole, it is important that more thanone treatment trial of a specific therapy demonstrate efficacy. Lastly by narrowlydelineating a severe syndrome, such as PMDD, women who seek treatment for aless severe condition, such as moderate PMS, and those with primarily somatic symp-toms and mild to moderate mood symptoms have been excluded from recent PMDDtreatment trials.
ACOG criteria for PMS and DSM-IV criteria for PMDD both require the presence
of at least one moderate to severe affective symptom and functional impairment
A. Rapkin / Psychoneuroendocrinology 28 (2003) 39–53
Table 1DSM-IV Diagnostic criteria for PMDD
b1-year duration of symptoms which are present for the majority of cycles [occur luteal/remit
b5 of the following symptoms (with at least 1 of these∗) must occur during the week before menses
–Affective lability∗ (sudden mood swings)
–Change in appetite, e.g., food cravingsbSeriously interferes with work, social activities, relationships
bConfirmed by prospective daily ratings during at least 2 consecutive symptomatic cycles
The overlap between severe PMS and PMDD has been estimatedto be approximately 79% Specific criteria for making thediagnoses of PMS and PMDD are described by in detail by Dr. Freeman in thisvolume. Once the diagnosis of severe PMS or PMDD has been established, treatmentcan ensue.
Since the diagnosis of PMS and PMDD both require prospective recording, it is
reasonable to initiate non-pharmacologic therapy during the two months of dailysymptom charting. Non-pharmacologic options for the treatment of PMS are outlined
bPatient reports Ն1 of the following affective and somatic symptoms during the 5 days beforemenses in each of 3 prior menstrual cycles:Affective
–Confusion–Social withdrawalbSymptoms relieved within 4 days of menses onset without recurrence until at least cycle day 13
bSymptoms present in absence of any pharmacologic therapy, hormone ingestion, or drug or alcohol
bSymptoms occur reproducibly during 2 cycles of prospective recording
bPatient suffers from identifiable dysfunction in social or economic performance
A. Rapkin / Psychoneuroendocrinology 28 (2003) 39–53
in If non-pharmacologic treatment is effective, the modality can be con-tinued and reassessed on a regular basis. Non-pharmacologic therapies include sup-portive or psychological therapy, aerobic exercise, and dietary supplementation. Diary symptom recording, discussion with family members regarding menstrual linkof symptoms and behavior modification are all considered supportive therapy. Thesesupportive measures have not been well studied.
Three published trials of cognitive therapy suggest that cognitive therapy is
superior to wait list (control) for improving premenstrual psychological and physicalsymptoms and functioning. Cognitive therapy was also found to be superior to groupawareness and to information focused therapy Group coping skills training was found to be superiorto relaxation training However, relaxation therapy twice daily wasfound to be superior to daily PMS symptoms charting alone
Diet, nutritional supplements and exercise have also been studied for PMS not
PMDD, albeit, in a limited number of investigations. A carbohydrate rich beveragemay help relieve premenstrual symptoms Aerobic exercisemay help the physical symptoms of PMS Calcium carbonate 1200 milligrams per day in divided doses has been foundin two controlled studies to reduce PMS symptoms Magnesium supplementation was found to be effective for the treatment of PMS inone placebo controlled trial Vitamin E, 400 units per day,may be minimally effective for PMS Vitamin B , 50–100 mg
per day, may be effective for PMS based on meta-analysis of inconsistent data There is also limited support (one placebo controlled trial) for L-trypto-phan, 6 grams per day, from ovulation until day 3 of menses for the treatment ofPMDD Dietary recommendations, such as avoiding salt,chocolate, caffeine and alcohol have never been subjected to either observational orcontrolled studies.
Pharmacologic interventions that have demonstrated efficacy for severe PMS or
PMDD include serotonergic anti-depressants, anxiolytics, and some agents which
Table 3Nonpharmacologic treatment of PMS and PMDD
PMS = premenstrual syndrome; PMDD = premenstrual dysphoric disorder. A. Rapkin / Psychoneuroendocrinology 28 (2003) 39–53
lead to ovulation suppression Currently ACOG recommends treatmentwith a selective serotonin reuptake inhibitor (SSRI) as the drug of choice for severePMS/PMDD. Symptoms associated with PMS/PMDD overlap those associated withreduced serotonin neurotransmission depression, mood swings, irri-tability,
aggression, decreased pain threshold, carbohydrate cravings and difficulty concen-trating. There is also ample evidence suggesting central nervous system serotonergicfunctioning is altered during the luteal phase in women with PMS and PMDD. Low-ered whole blood serotonin decreased platelet uptake of sero-tonin and decreased platelet MAO activity in the luteal phasehave all been noted. There is also evidence that ovarian sexsteroids effect serotonin uptake, turnover, binding, and transport It has been suggested that the symptoms of PMS/PMDD may resultat least in part from serotonergic dysregulation.
Numerous pharmacologic agents which increase CNS serotonin concentrations
levels have been shown to be effective for the treatment of severe PMS/PMDD. At least 15 double-blind placebo controlled trials of such antidepressants (selectiveserotonin reuptake inhibitors or serotonergic tricyclic agents) have been publishedover the last 10 years. All serotonergic antidepressants which have been studied thusfar have been found to be more effective than placebo with an average response rateof approximately 60% SSRIs, in particular fluoxetine and sertraline, have been shown to beeffective for the treatment of both the affective and the physical symptoms of PMDDand both medications lead to improved psychosocial functioning, work performanceand quality of life Luteal phase administration has also beenfound to be effective for fluoxetine citalopram sertraline and clomipramine Prolonged efficacy, up to 47months has been demonstrated for fluoxetine in open trials The specificity of response to serotonergic antidepressants in women withPMDD is marked. Trials comparing fluoxetine to bupropion sertraline to desipramine and paroxetine to maprotiline
Table 4Evidence based pharmacologic treatments for PMS and PMDD
A. Rapkin / Psychoneuroendocrinology 28 (2003) 39–53
demonstrate that augmenting noradrenergic activity alone isnot effective for the treatment of PMDD.
For women with persistent anxiety after adequate trial of SSRI’s, anxiolytics can
be added in the luteal phase of the menstrual cycle. Although, there is contradictoryevidence, there are at least two positive placebo controlled trials demonstrating effi-cacy for luteal phase administration of alprazolam for treatment of PMS Buspirone, a 5HT agonist, has also been shownto be more effective than placebo in at least one randomized trial Often the most severe symptoms occur in the late lutealphase at the time of declining progesterone concentrations and progesterone can haveanxiolytic properties due to the action of progesterone metabolites at the GABAAreceptors Early therapeutic interventions thus utilized pro-gesterone supplementation without suppression of ovulation. However, there is noevidence of a consistent hormonal aberration in PMS, progesterone levels are notaltered in women with PMS and double blind placebo con-trolled trials of progesterone supplementation for the treatment of PMS have notdemonstrated efficacy
There is an obvious link between the appearance of PMS/PMDD symptomatology
and the rise and fall of sex steroids associated with ovulation. PMS and PMDD do notoccur premenarchally or in post menopausal women who are not receiving hormonereplacement therapy, or for the most part during spontaneously anovulatory cycles. Symptoms resolve with pregnancy and with oopherectomy Attention has therefore focused on ovulation suppression for the treatment ofPMS/PMDD.
The administration of a gonadotropin releasing hormone agonist (GnRH agonist)
results in a “medical oopherectomy” and menopausal concentrations of plasma estro-gen and progesterone. GnRH agonists have been found to be effective for the treat-ment of PMS and PMDD Thehypoestrogenic state afforded by GnRH agonists has the unfortunate consequences ofhot flashes, vaginal dryness, and occasionally depression, headaches and muscleaches. Furthermore, long-term GnRH treatment can result in osteoporosis andincreased risk of cardiovascular disease. Women with severe PMS and predominantor concomitant depression may not respond to GnRH agonists Add-back therapy with estrogen and progesterone or tibolonein menopausal doses can theoretically prevent the long-term risk of osteoporosis andheart disease while continuing to provide relief of symptoms however, these add-back hormones may, at least initially,induce mood symptoms in women with severe PMS or PMDD
Several studies have investigated the use of the androgen derivative, danazol for
the treatment of PMS. In a dose of 200 mg per day danazol reduced mood andsomatic symptoms, especially migraine and mastaglia However, danazol seems to be effectiveprimarily if anovulation is produced Contraception is manda-tory when prescribing danazol because some women will ovulate on low-dose dana-zol and danazol can virilize the fetus. At the higher doses of 600–800 mg per day
A. Rapkin / Psychoneuroendocrinology 28 (2003) 39–53
required to suppress ovulation, danazol is associated with side effects such as weightgain, mood changes, fluid retention and acne.
High-dose transdermal estradiol 200 mcg provided via patch can prevent ovulation
and reduce symptoms of PMS However, this high-dose estro-gen therapy with cyclic low-dose progestin supplementation for the last 7 days ofthe cycle has not been clearly demonstrated to eliminate the risk of endometrialhyperplasia associated with estrogen administration.
Ovulation suppression is often efficacious for the treatment of PMS/PMDD. Long-
term therapy for PMS/PMDD is necessary as symptoms recur upon discontinuationof treatment and the syndrome usually persists until thewaning of ovarian function with the menopause. Furthermore, women of repro-ductive age often require contraception. It is surprising therefore that there are veryfew double blind, placebo controlled trials of oral contraceptive (OC) agents for thetreatment of PMS. One OC trial for the treatment of PMDD has been publishedA randomized placebo, controlled trial concluded that a tri-phasic OC formulation reduced physical symptoms but not mood abnormalities ofPMS Another study comparing a tri-phasic to a mono-phasic OC regimen demonstrated that the mono-phasic regimen was less likely tocause adverse mood changes Conclusions regarding thetreatment of PMS/PMDD with oral contraceptives are limited by a dearth of placebocontrolled trials. Further complicating the issue is the fact that, many symptoms ofPMS/PMDD such as breast tenderness, headache, bloating, and depression can alsobe side effects of some oral contraceptive pills. Future studies will determine whethercontinuous OCP intake with limited active pill withdrawal at intervals of 3 monthsor longer will help to ameliorate the symptoms associated with the limited rise andfall of sex steroids associated with monthly cyclic regimens
There are numerous health advantages afforded by oral contraceptive pill intake.
The OCs provide effective, reversible contraception but also have other known bene-fits including prevention of bone loss, decreased risks for ovarian and endometrialcancer, anemia, abnormal uterine bleeding, uterine myomata, endometriosis, pelvicinflammatory disease, as well as complications of unplanned pregnancy, such asectopic pregnancy and molar gestation. Some methods of ovarian suppression forPMS do not reliably provide contraception and may have potential risk for the endo-metrium (e.g., danazol or estradiol) or bones (GnRH agonists).
As ovulation suppression should be effective for the treatment of PMS/PMDD,
the obvious challenge is to identify an oral contraceptive pill formulation that hasminimal “PMS-like” side-effects. The adverse mood effects of oral contraceptivepills in some women may be related to the fact that the progestins utilized in mostoral contraceptives are derived from testosterone (19-nortestosterone derivatives). reported that women with PMS had a higher level of serumfree testosterone, suggesting androgens may be associated with premenstrual irrita-bility and dysphoria. Increased levels of testosterone during the late luteal phasehave been postulated to be related to irritative and impulsive symptoms The most bothersome physical side-effects of the OC are bloating andbreast tenderness, and these symptoms are at least in part, attributable to water reten-
A. Rapkin / Psychoneuroendocrinology 28 (2003) 39–53
tion, probably related to the estrogenic component of the OC. Spironolactone, apotassium sparing diuretic with antiandrongenic and antimineralocorticoid propertieshas been used with modest success in the treatment of PMS
The major trend in the formulation of oral contraceptives over the last 40 years
has been a reduction in the doses of both the estrogen and the progestin components,and more recently, chemical alterations of the progestins to provide less androgeniccompounds. Estradiol (ethinyl estradiol) doses have decreased from 100 microgramsto 20–30 micrograms. The dose of the progestin component has also decreased. Allbut one currently prescribed OC still contains a progestin derived from 19-nortestos-terone. summarizes the pharmacologic profile of progesterone, 19-nortestos-terone and a new progestin, structurally unrelated to other classes of progestins,derived from spirolactone, called drospirenone.
Drospirenone is an analog of the mineralocorticoid antagonist, spironolactone. Spi-
ronolactone and drospirenone bind antagonistically to the androgen receptor. Drospir-enone has also been demonstrated to have a high binding affinity for the progesteroneand glucocorticoid receptor and both progesterone and drospirenone have anti-min-eralocorticoid activity and both are progestagenic and anti-androgenic
An oral contraceptive containing drospirenone, a spironolactone analog, instead
of a 19-nortestosterone derived progestin should ameliorate water retention, bloating,weight gain and breast tenderness. Furthermore, the anti-androgenic properties ofdrospirenone are theorized to decrease irritability and tension.
conducted an open label multi-center study to evaluate
the efficacy, safety, and cycle control of a new low-dose combination OC containing3 mg of drospirenone and 30 mcg of ethinyl estradiol called Yasmin. Menstrualsymptoms were assessed in 326 women at baseline and at cycle 6, using a modified
Table 5Pharmacologic profile of progestins (in animal models)
+ = distinct effect: (+) = negligible effect at therapeutic doses; Ϫ = no effect. ∗Metabolized to levonorges-trel-3-oxime and levonorgestrel. ∗∗Not available in the USA. A. Rapkin / Psychoneuroendocrinology 28 (2003) 39–53
menstrual distress questionnaire The occurrence of menstrual relatedsymptoms was documented for three phases of the menstrual cycle: premenstrual—the four day periods before menstruation, menstrual—the first through the last dayof menstruation, postmenstrual—the remainder of the menstrual cycle. The resultsof the Women’s Health Assessment Questionnaire are shown in Statisticallysignificant decreases from baseline to cycle 6 were observed in all menstrual phasesfor negative affect and water retention. In the premenstrual and menstrual phases,severity of appetite increase was also significantly lower in cycle 6 compared withbaseline. The OC containing ethinyl estradiol and drospirenone (Yasmin) was foundto be an effective and safe method of oral contraception, with the effectiveness asmeasured by Pearl Index similar to that of other combination OCs and with an accept-able rate of breakthrough bleeding, spotting, and amenorrhea
As Yasmin was well tolerated and demonstrated an impact on the severity of
menstrual cycle symptoms, a double blind placebo controlled trial for the treatmentof PMS was undertaken. 261 women with PMS completed a 6 month double blind,randomized placebo controlled trial. Of the 82 women in this PMS group who alsofulfilled criteria for PMDD, 42 were in the drospirenone/EE treatment arm. Theprimary assessment tool for this study was the Calendar of Premenstrual Experiences(COPE) Symptoms were followed on a daily basis for twobaseline and three treatment cycles. The 22 symptoms were grouped into four factorsIn addition, the clinical global impression (CGI) was asked of investigatorsand subjects at the end of treatment for a subgroup of subjects. The primary objectiveof the study was to evaluate the efficacy of DSRP 3 mg and EE 30 mcg in thetreatment of PMDD by looking at the change from baseline in the luteal phase factor1 (mood score). Secondary outcome measures were between group differences in
Table 6Women’s health assessment questionnaire
A. Rapkin / Psychoneuroendocrinology 28 (2003) 39–53
Mean changes in menstrually related symptoms from baseline to cycle 6 for three phases of the
menstrual cycle. The premenstrual phase (A) included the 4-day period before menstruation; the menstrualphase (B) included the first through last day of menstruation; and the postmenstrual phase (C) includedthe remainder of the cycle.
∗Numbers in parentheses are the COPE item numbers.
change from baseline to last treatment cycle in luteal phase factors 2–4 scores andchange from baseline in the total luteal COPE score and CGI. The drop out rate didnot differ from those receiving active drug vs. placebo, indicating that the medicationwas well tolerated.
The results of the COPE score for the 82 PMDD subjects showed that improve-
A. Rapkin / Psychoneuroendocrinology 28 (2003) 39–53
ment occurred in all 22 measured symptoms over 3 treatment cycles for both theDRSP/EE group and the placebo group The DRSP/EE arm showed greatermagnitude of change from baseline in each of the 22 items. The DRSP/EE treatmentshowed a statistically better response than placebo for three questions; increasedappetite p = 0.034, wish to be alone p =0.018 and hot flashes p = 0.017 with a trendfor improvement in forgetfulness p = 0.0178 and food cravings p = 0.077. Analysesof the factor 1 (mood) showed that active treatment produced a better response thanplacebo but did not reach statistical significance. In the secondary analysis of individ-ual factors, the subjects receiving the active drug showed better results than placeboin all factors and the overall total COPE score. Statistical significance was reachedfor factors 3 items: increased appetite, food cravings and acne. Investigators ratedsubjects (CGI) on the active treatment as improved by 100% at cycle 3 comparedwith improvement by 50% on placebo In sum, data from a double blindplacebo controlled study using DSRP/EE demonstrated that women on active drugfared better than women on placebo, significantly for some symptoms with a trendfor others. However, the PMDD trial was hampered by a high placebo response rate(43%) that was sustained beyond initial treatment cycle. The study was initiallyproposed to evaluate PMS and not PMDD. As the symptoms of PMS can be morenumerous and less severe than those of PMDD the placebo response is often higher. Furthermore, the study did not have adequate power i.e. enough subjects, to detecta treatment response difference between the PMDD and control groups. Additionally,the COPE, which has a range from 0 to 3, is not sensitive enough to detect differencesbetween mild and moderate improvement over time. Further studies are in progressto investigate the magnitude of the effect of drospirenone/EE in reducing the symp-toms of PMS/PMDD.
CGI scores for PMDD subjects receiving placebo (n = 6) or DRSP/EE (n = 8) assessed at the
A. Rapkin / Psychoneuroendocrinology 28 (2003) 39–53
Currently, SSRIs are the treatment of choice for PMS/PMDD, and at this time,
fluoxetine and sertraline are the only FDA approved SSRIs for the indication ofPMDD. However, current investigations with novel oral contraceptive agents admin-istered cyclically or continuously, which provide both contraception and other healthbenefits and which prevent ovulation and significantly ameliorate symptoms ofPMDD may be on the horizon. References
ACOG (American College of Obstetricians and Gynecologists), 2000. Premenstrual Syndrome. ACOG
APA (American Psychiatric Association), 1994. Diagnostic and Statistical Manual of Mental Disorders,
fourth ed. (DSM-IV). American Psychiatric Association, Washington, DC, pp. 715-718.
Ashby, C.R., Carr, L.A., Cook, C.L., Steptoe, M.M., Franks, D.D., 1988. Alteration of platelet serotonergic
mechanisms and monoamine oxidase activity in premenstrual synrome. Biol. Psychiatry 24, 225–233.
Aslaksen, K., Falk, V., 1991. Spironolactone in the treatment of premenstrual tension: A double-blind
study of spironolactone versus bendrflumehtiazide and placebo. Curr. Ther. Res. 49, 120–130.
Ba¨ckstro¨m, T., Hansson-Malmstro¨m, Y., Lindhe, B.A
˚ , Cavalli-Bjo¨rkman, B., Nordenstro¨m, S., 1992. Oral
contraceptives in premenstrual syndrome: A randomized comparison of triphasic and monophasicpreparations. Contraception 46, 253–268.
Biegon, A., McEwen, B.S., 1982. Modulation by estradiol of serotonin receptors in brain. J. Neurosci.
Blake, F., Salkovskis, P., Gath, D., Day, A., Garrod, A., 1998. Cognitive therapy for premenstrual syn-
drome: A controlled trial. J. Psychosom. Res. 45, 307–318.
Brown, C.S., Ling, F.W., Andersen, R.N., Farmer, R.G., Arheart, K.L., 1994. Efficacy of depot leuprolide
in premenstrual syndrome: effect of symptom severity and type in a controlled trial. Obstet. Gynecol. 84, 779–786.
Casper, R.F., Hearn, M.T., 1990. The effect of hysterectomy and bilateral oophorectomy in women with
severe premenstrual syndrome. Am. J. Obstet. Gynecol. 162, 105–109.
Christensen, A.P., Oei, T.P., 1995. The efficacy of cognitive behaviour therapy in treating premenstrual
dysphoric changes. J. Affect. Disor. 33, 57–63.
Di Carlo, C., Palomba, S., Tommaselli, G.A., Guida, M., Di Spiezio Sardo, A., Nappi, C., 2001. Use of
leuprolide acetate plus tibolone in the treatment of severe premenstrual syndrome. Fertil. Steril. 75(2), 380–384.
Dimmock, P.W., Wyatt, K.M., Jones, P.W., O’Brien, P.M.S., 2000. Efficacy of selective serotonin-reup-
take inhibitors in premenstrual syndrome: A systematic review. Lancet 356 (9236), 1131–1136.
Dougherty, D.M., Bjork, J.M., Moeller, F.G., Swann, A.C., 1997. The influence of menstrual-cycle phase
on the relationship between testosterone and aggression. Physiol. Behav. 62, 431–435.
Eriksson, E., Hedberg, M.A., Andersch, B., Sundblad, C., 1995. The serotonin reuptake inhibitor paroxet-
ine is superior to the noradrenaline reuptake inhibitor maprotiline in the treatment of premenstrualsyndrome. Neuropsychopharmacology 12, 167–176.
Eriksson, E., Sundblad, C., Lisjo, P., Modigh, K., Andersch, B., 1992. Serum levels of androgens are
higher in women with premenstrual irritability and dysphoria than in controls. Psychoneuroendocrinol-ogy 17, 195–204.
Facchinetti, F., Borella, P., Sances, G., Fioroni, L., Nappi, R.E., Genazzani, A.R., 1991. Oral magnesium
successfully relieves premenstrual mood changes. Obstet. Gynecol. 78, 177–181.
Freeman, E.W., Rickels, K., Sondheimer, S.J., Wittmaack, F.M., 1996. Sertraline versus desipramine in
the treatment of premenstrual syndrome: An open-label trial. J. Clin. Psychiatry 57, 7–11.
Freeman, E.W., Rickels, K., Sondheimer, S.J., Polansky, M., 1995. A double-blind trial of oral progester-
one, alprazolam, and placebo in treatment of severe premenstrual syndrome. JAMA 274, 51–57.
Freeman, E.W., Sondheimer, S.J., Rickels, K., Albert, J., 1993. Gonadotropin-releasing hormone agonist
A. Rapkin / Psychoneuroendocrinology 28 (2003) 39–53
in treatment of premenstrual symptoms with and without comorbidity of depression: A pilot study. J. Clin. Psychiatry 54, 192–195.
Freeman, E.W., Kroll, R., Rapkin, A., for the PMS/PMDD Research Group 2001a. Evaluation of a unique
oral contraceptive in the treatment of premenstrual dysphoric disorder. J. Womens Health Gend. BasedMed. 10, 561–569.
Freeman, E.W., Rickels, K., Yonkers, K.A., Kunz, N.R., McPherson, M., Upton, G.V., 2001b. Venlafaxine
in the treatment of premenstrual dysphoric disorder. Obstet. Gynecol. 98 (5), 737–744.
Fuhrmann, U., Krattenmacher, R., Slater, E.P., Frizemeier, K.H., 1996. The novel progestin drospirenone
and its natural counterpart progesterone: Biochemical profile and antiandrogenic potential. Contracep-tion 54, 243–251.
Goodale, I.L., Domar, A.D., Benson, H., 1990. Alleviation of premenstrual syndrome symptoms with the
relaxation response. Obstet. Gynecol. 75, 649–655.
Graham, C.A., Sherwin, B.B., 1992. A prospective treatment study of premenstrual symptoms using a
triphasic oral contraceptive. J. Psychosom. Res. 36, 257–266.
Halbreich, U., Rojansky, N., Palter, S., 1991. Elimination of ovulation and menstrual cyclicity (with
danazol) improves dysphoric premenstrual syndromes. Fertil. Steril. 56, 1066–1069.
Halbreich, U., Smoller, J.W., 1997. Intermittent luteal phase sertraline treatment of dysphoric premenstrual
syndrome. J. Clin. Psychiatry 58, 399–402.
Harrison, W.M., Endicott, J., Nee, J., 1990. Treatment of premenstrual dysphoria with alprazolam. A
controlled study. Arch. Gen. Psychiatry 47, 270–275.
Jermain, D.M., Preece, C.K., Sykes, R.L., Kuehl, T.J., Sulak, P.J., 1999. Luteal phase sertraline treatment
for premenstrual dysphoric disorder. Results of a double-blind, placebo-controlled, crossover study. Arch. Fam. Med. 8, 328–332.
Kirkby, R.J., 1994. Changes in premenstrual symptoms and irrational thinking following cognitive-
behavioral coping skills training. J. Consult. Clin. Psychol. 62, 1026–1032.
London, R.S., Murphy, L., Kitlowski, K.E., Reynolds, M.A., 1987. Efficacy of alpha-tocopherol in the
treatment of the premenstrual syndrome. J. Reprod. Med. 32, 400–404.
Morse, C.A., Dennerstein, L., Farrell, E., Varnavides, K., 1991. A comparison of hormone therapy, coping
skills training, and relaxation for the relief of premenstrual syndrome. J. Behav. Med. 14, 469–489.
Mortola, J.F., 1993. Applications of gonadotropin-releasing hormone analogues in the treatment of pre-
menstrual syndrome. Clin. Obstet. Gynecol. 36, 753–763.
Mortola, J.F., Girton, L., Beck, L., Yen, S.S., 1990. Diagnosis of premenstrual syndrome by a simple,
prospective, and reliable instrument: The calendar of premenstrual experiences. Obstet. Gynecol. 76,302–307.
Mortola, J.F., Girton, L., Fischer, U., 1991. Successful treatment of severe premenstrual syndrome by
combined use of gonadotropin-releasing hormone agonist and estrogen/progestin. J. Clin. Endocrinol. Metab. 72, 252A–252F.
Muse, K.N., Cetel, N.S., Futterman, L.A., Yen, S.C., 1984. The premenstrual syndrome. Effects of “medi-
cal ovariectomy”. N. Engl. J. Med. 311, 1345–1349.
O’Brien, P.M.S., Craven, D., Selby, C., Symonds, E.M., 1979. Treatment of premenstrual syndrome by
spironolactone. Br. J. Obstet. Gynaecol. 86, 141–147.
O’Brien, P.M.S., Abukhalil, I.E.H., 1999. Randomized controlled trial of the management of premenstrual
syndrome and premenstrual mastalgia using luteal phase-only danazol. Am. J. Obstet. Gynecol. 180,18–23.
Parsey, K.S., Pong, A., 2000. An open-label, multicenter study to evaluate Yasmin, a low-dose combi-
nation oral contraceptive containing drospirenone, a new progestogen. Contraception 61, 105–111.
Pearlstein, T.B., Halbreich, U., Batzar, E.D., Brown, C.S., Endicott, J., Frank, E., Greeman, E.W., Harri-
son, W.M., Haskett, R.F., Stout, A.L., Yonkers, K.A., 2000. Psychosocial functioning in women withpremenstrual dysphoric disorder before and after treatment with Sertraline or placebo. J. Clin. Psy-chiatry 61, 101–109.
Pearlstein, T.B., Stone, A.B., 1994. Long-term fluoxetine treatment of late luteal phase dysphoric disorder.
Pearlstein, T.B., Stone, A.B., Lund, S.A., Scheft, H., Zlotnick, C., Brown, W.A., 1997. Comparison of
A. Rapkin / Psychoneuroendocrinology 28 (2003) 39–53
fluoxetine, bupropion, and placebo in the treatment of premenstrual dysphoric disorder. J. Clin. Psycho-pharmacol. 17, 261–266.
Prior, J.C., Vigna, Y., Sciarretta, D., Alojado, N., Schulzer, M., 1987. Conditioning exercise decreases
premenstrual symptoms: a prospective, controlled 6-month trial. Fertil. Steril. 47, 402–408.
Rapkin, A.J., 1992. The role of serotonin in premenstrual syndrome. Clin. Obstet. Gynecol. 35, 629–636. Rapkin, A.J., Chang, L.C., Reading, A.E., 1988. Comparison of retrospective and prospective assessment
of premenstrual symptoms. Psychol. Rep. 62, 55–60.
Rapkin, A.J., Edelmuth, E., Chang, L.C., Reading, A.E., McGuire, M.T., Su, T.P., 1987a. Whole-blood
serotonin in premenstrual syndrome. Obstet. Gynecol. 70, 533–537.
Rapkin, A.J., Chang, L.C., Reading, A.E., 1987b. Premenstrual syndrome: a double blind placebo con-
trolled study of treatment with progesterone vaginal suppositories. J. Obstet. Gynecol. 7, 217–220.
Rapkin, A.J., Morgan, M., Goldman, L., Brann, D.W., Simone, D., Mehesh, V.B., 1997. Progesterone
metabolite allopregnanolone in women with premenstrual syndrome. Obstet. Gynecol. 90, 709–714.
Rickels, K., Freeman, E., Sondheimer, S., 1989. Buspirone in treatment of premenstrual syndrome [letter].
Rubinow, D.R., Hoban, M.C., Grover, G.N., et al. 1988. Changes in plasma hormones across the menstrual
cycle in patients with menstrually related mood disorder and in control subjects. Am. J. Obstet. Gyn-ecol. 158, 5–11.
Sarno, A.P. Jr, Miller, E.J. Jr, Lundblad, E.G., 1987. Premenstrual syndrome: Beneficial effects of per-
iodic, low-dose danazol. Obstet. Gynecol. 70, 33–36.
Sayegh, R., Schiff, I., Wurtman, J., Spiers, P., McDermott, J., Wurtman, R., 1995. The effect of a carbo-
hydrate-rich beverage on mood, appetite, and cognitive function in women with premenstrual syn-drome. Obstet. Gynecol. 86, 520–528.
Schmidt, P.J., Nieman, L.K., Danaceau, M.A., Adams, L.F., Rubinow, D.R., 1998. Differential behavioral
effects of gonadal steroids in women with and in those without premenstrual syndrome. N. Engl. J. Med. 338, 209–216.
Steege, J.F., Blumenthal, J.A., 1993. The effects of aerobic exercise on premenstrual symptoms in middle-
aged women: A preliminary study. J. Psychosom. Res. 37, 127–133.
Steinberg, S., Annable, L., Young, S.N., Liyanage, N., 1999. A placebo-controlled clinical trial of L-
tryptophan in premenstrual dysphoria. Biol. Psychiatry 45, 313–320.
Steiner, M., Korzekwa, M., Lamont, J., Wilkins, A., 1997. Intermittent fluoxetine dosing in the treatment
of women with premenstrual dysphoria. Psychopharmacol. Bull. 33, 771–774.
Steiner, M., Steinberg, S., Stewart, D., et al. 1995. Fluoxetine in the treatment of premenstrual dysphoria.
Canadian Fluoxetine/Premenstrual Dysphoria Collaborative Study Group. N. Engl. J. Med. 332,1529–1534.
Sulak, P.J., Scow, R.D., Preece, C., Riggs, M.W., Kuehl, T.J., 2000. Hormone withdrawal symptoms in
oral contraceptive users, continuous use. Obstet. Gynecol. 95, 261–266.
Sundblad, C., Hedberg, M.A., Eriksson, E., 1993. Clomipramine administered during the luteal phase
reduces the symptoms of premenstrual syndrome: a placebo-controlled trial. Neuropsychopharmacol-ogy 9, 133–145.
Sundblad, C., Modigh, K., Andersch, B., Eriksson, E., 1992. Clomipramine effectively reduces premen-
strual irritability and dysphoria: a placebo-controlled trial. Acta. Psychiatr. Scand. 85, 39–47.
Thys-Jacobs, S., Starkey, P., Bernstein, D., Tian, J., 1998. Calcium carbonate and the premenstrual syn-
drome: effects on premenstrual and menstrual symptoms. Premenstrual Syndrome Study Group. Am. J. Obstet. Gynecol. 179, 444–452.
Thys-Jacobs, S., Ceccarelli, S., Bierman, A., et al. 1989. Calcium supplementation in premenstrual syn-
drome: A randomized crossover trial. J. Gen. Intern. Med. 4, 183–189.
Watson, N.R., Studd, J.W.W., Savvas, M., Garnett, T., Baber, R.J., 1989. Treatment of severe premen-
strual syndrome with oestradiol patches and cyclical oral norethisterone. Lancet 2, 730–732.
Wikander, I., Sundblad, C., Andersch, B., et al. 1998. Citalopram in premenstrual dysphoria: is intermittent
treatment during luteal phases more effective than continuous medication throughout the menstrualcycle? J. Clin Psychopharmacol. 18, 390–398.
Wyatt, K.M., Dimmock, P.W., Jones, P.W., Shaughn O’Brien, P.M., 1999. Efficacy of vitamin B-6 in
the treatment of premenstrual syndrome: systematic review. BMJ 318, 1375–1381. A. Rapkin / Psychoneuroendocrinology 28 (2003) 39–53
Yonkers, K.A., Halbreich, U., Freeman, E., et al. 1997. Symptomatic improvement of premenstrual dysph-
oric disorder with sertraline treatment. A randomized controlled trial. Sertraline Premenstrual Dysph-oric Collaborative Study Group. JAMA 278, 983–988.
Young, S.A., Hurt, P.H., Benedek, D.M., Howard, R.S., 1998. Treatment of premenstrual dysphoric dis-
order with sertraline during the luteal phase: a randomized, double-blind, placebo-controlled crossovertrial. J. Clin. Psychiatry 59, 76–80.
WARNING: Dance is a Drug I’ve been noticing the various and ever more present advertisements for drugs on television. One of them is a full 2 minute 30 second ‘mind-bender’(Celebrex) that displays a pretty blue background throughout (for the feeling of comfort) and full of many distractions happening while they tell you about what their product does. With fish swimming around whose
MC Vol. 19 - No.2 - 2012 ( 93 - 96 ) Talpur A. A. et al APRIL - JUNE 2012 SENSITIVITY PATTERN OF SALMONELLA TYPHI IN PATIENTS WITH TYPHOID SMALL BOWEL PERFORATIONS ALTAF AHMED TALPUR ABSTRACT NAND LAL KELLA ABDUL RASHID SURAHIO Background: Enteric fever caused by Salmonella Typhi, gram negative bacilli, is counted MUHAMMAD JAVED as a major public health problem, especi

 Psychoneuroendocrinology 28 (2003) 39–53
syndrome & premenstrual dysphoric disorder
UCLA School of Medicine, Department of Obstetrics and Gynecology, Center for the Health Sciences,
Room 27-165, 10833 Le Conte Avenue, Los Angeles, CA 90095-1740, USA
Abstract
Psychoneuroendocrinology 28 (2003) 39–53
syndrome & premenstrual dysphoric disorder
UCLA School of Medicine, Department of Obstetrics and Gynecology, Center for the Health Sciences,
Room 27-165, 10833 Le Conte Avenue, Los Angeles, CA 90095-1740, USA
Abstract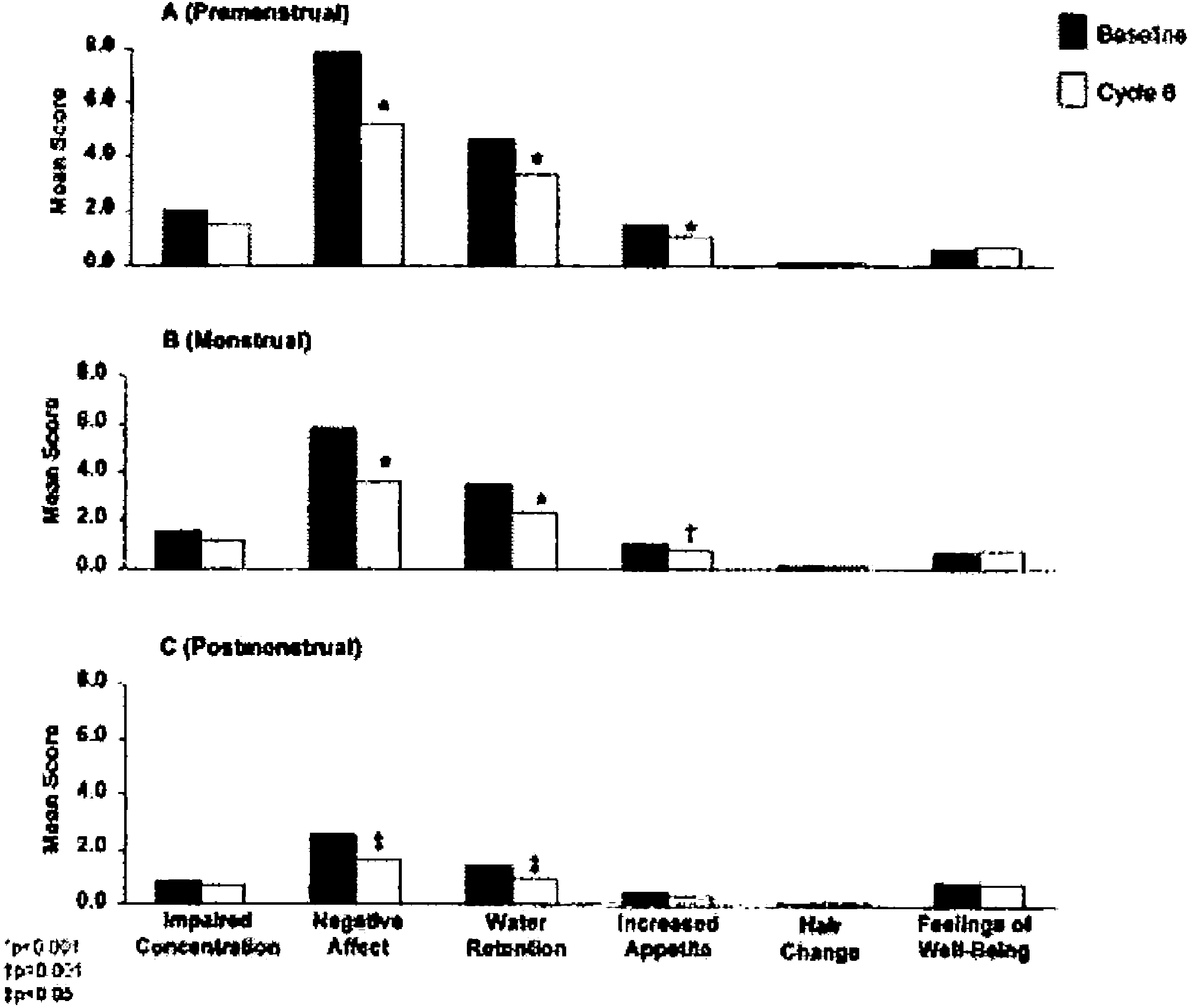 A. Rapkin / Psychoneuroendocrinology 28 (2003) 39–53
Mean changes in menstrually related symptoms from baseline to cycle 6 for three phases of the
menstrual cycle. The premenstrual phase (A) included the 4-day period before menstruation; the menstrualphase (B) included the first through last day of menstruation; and the postmenstrual phase (C) includedthe remainder of the cycle.
A. Rapkin / Psychoneuroendocrinology 28 (2003) 39–53
Mean changes in menstrually related symptoms from baseline to cycle 6 for three phases of the
menstrual cycle. The premenstrual phase (A) included the 4-day period before menstruation; the menstrualphase (B) included the first through last day of menstruation; and the postmenstrual phase (C) includedthe remainder of the cycle.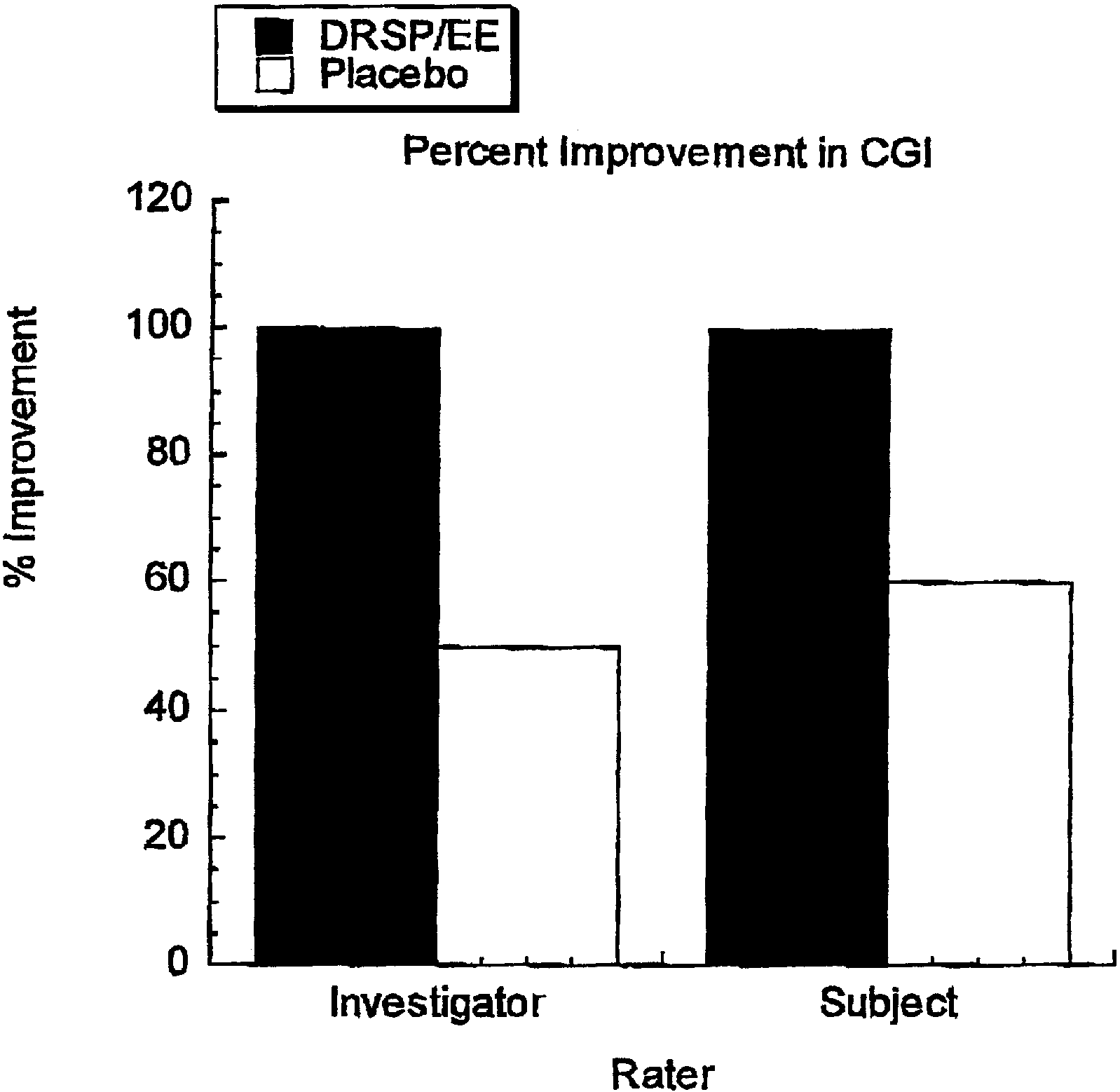 A. Rapkin / Psychoneuroendocrinology 28 (2003) 39–53
ment occurred in all 22 measured symptoms over 3 treatment cycles for both theDRSP/EE group and the placebo group The DRSP/EE arm showed greatermagnitude of change from baseline in each of the 22 items. The DRSP/EE treatmentshowed a statistically better response than placebo for three questions; increasedappetite p = 0.034, wish to be alone p =0.018 and hot flashes p = 0.017 with a trendfor improvement in forgetfulness p = 0.0178 and food cravings p = 0.077. Analysesof the factor 1 (mood) showed that active treatment produced a better response thanplacebo but did not reach statistical significance. In the secondary analysis of individ-ual factors, the subjects receiving the active drug showed better results than placeboin all factors and the overall total COPE score. Statistical significance was reachedfor factors 3 items: increased appetite, food cravings and acne. Investigators ratedsubjects (CGI) on the active treatment as improved by 100% at cycle 3 comparedwith improvement by 50% on placebo In sum, data from a double blindplacebo controlled study using DSRP/EE demonstrated that women on active drugfared better than women on placebo, significantly for some symptoms with a trendfor others. However, the PMDD trial was hampered by a high placebo response rate(43%) that was sustained beyond initial treatment cycle. The study was initiallyproposed to evaluate PMS and not PMDD. As the symptoms of PMS can be morenumerous and less severe than those of PMDD the placebo response is often higher.
A. Rapkin / Psychoneuroendocrinology 28 (2003) 39–53
ment occurred in all 22 measured symptoms over 3 treatment cycles for both theDRSP/EE group and the placebo group The DRSP/EE arm showed greatermagnitude of change from baseline in each of the 22 items. The DRSP/EE treatmentshowed a statistically better response than placebo for three questions; increasedappetite p = 0.034, wish to be alone p =0.018 and hot flashes p = 0.017 with a trendfor improvement in forgetfulness p = 0.0178 and food cravings p = 0.077. Analysesof the factor 1 (mood) showed that active treatment produced a better response thanplacebo but did not reach statistical significance. In the secondary analysis of individ-ual factors, the subjects receiving the active drug showed better results than placeboin all factors and the overall total COPE score. Statistical significance was reachedfor factors 3 items: increased appetite, food cravings and acne. Investigators ratedsubjects (CGI) on the active treatment as improved by 100% at cycle 3 comparedwith improvement by 50% on placebo In sum, data from a double blindplacebo controlled study using DSRP/EE demonstrated that women on active drugfared better than women on placebo, significantly for some symptoms with a trendfor others. However, the PMDD trial was hampered by a high placebo response rate(43%) that was sustained beyond initial treatment cycle. The study was initiallyproposed to evaluate PMS and not PMDD. As the symptoms of PMS can be morenumerous and less severe than those of PMDD the placebo response is often higher.