Endothelial Function in Obstructive Sleep Apnea and Response to Treatment Mary S. M. Ip, Hung-Fat Tse, Bing Lam, Kenneth W. T. Tsang, and Wah-Kit Lam
Department of Medicine, The University of Hong Kong, Queen Mary Hospital, Hong Kong, China
Impaired endothelium-dependent vascular relaxation is a prognos-
evaluate vascular reactivity, in particular endothelium-dependent
tic marker of atherosclerosis and cardiovascular disease. We evalu-
flow-mediated dilation (FMD), in the brachial artery in subjects
ated endothelium-dependent flow-mediated dilation (FMD) and
with OSA compared with subjects without OSA, and its response
endothelium-independent nitroglycerin (NTG)–induced dilation of
to OSA treatment with nCPAP, in a randomized controlled
the brachial artery with Doppler ultrasound in 28 men with obstruc- tive sleep apnea (OSA) and 12 men without OSA. Subjects with OSA (apnea–hypopnea index; mean Ϯ SD, 46.0 Ϯ 14.5) had lower FMD compared with subjects without OSA (5.3 Ϯ 1.7% vs. 8.3 Ϯ 1.0%, p Ͻ 0.001), and major determinants of FMD were the apnea– Subjects and Study Protocol hypopnea index and age. There was no significant difference in
Subjects were recruited from the Sleep Laboratory, University Depart-
NTG-induced dilation. Subjects with OSA were randomized to nasal
ment of Medicine, Queen Mary Hospital. For sleep apnea subjects,
continuous positive airway pressure (nCPAP) or observation for 4
inclusion criteria were apnea–hypopnea index (AHI) of 15 or more
weeks. Subjects on nCPAP had significant increase in FMD, whereas
and male sex. Exclusion criteria were previous treatment for OSA,
those on observation had no change (4.4% vs. Ϫ0.8%, difference
presence of structural heart disease, history of hypertension, dyslipide-
of 5.2%, p Ͻ 0.001). Neither group showed significant change in
mia, diabetes mellitus, other chronic illness or medications (including
NTG-induced vasodilation. Eight subjects who used nCPAP for over
over-the-counter medicines or “health tonics”), acute illness, or medica-
3 months were reassessed on withdrawing treatment for 1 week.
tions within the past 2 weeks. Male subjects with an AHI of less than
On nCPAP withdrawal, FMD became lower than during treatment
5, matched to subjects with OSA for body mass index, were recruited
(p ϭ 0.02) and were similar to baseline values. Our findings demon-
with similar exclusion criteria to form the normal control group. strated that men with moderate/severe OSA have endothelial dys-
At baseline, all subjects underwent evaluation of clinical profile,
function and treatment with nCPAP could reverse the dysfunction;
polysomnography, echocardiography, and vascular reactivity study. the effect, however, was dependent on ongoing use.
Sleep apnea subjects were then randomized to receive nCPAP treat-ment or no intervention. After 4 weeks, they were reassessed with all
Keywords: vascular reactivity; flow-mediated dilation; obstructive sleep
measurements except echocardiography. Patients who continued to use
apnea; endothelial function; nasal continuous positive airway pressure
nCPAP for at least 3 months were asked to stop nCPAP for 1 weekand were reassessed.
Obstructive sleep apnea (OSA) is associated with cardiovascular
The study was approved by the ethics committee of The University
diseases, including hypertension, coronary artery disease, heart
of Hong Kong, and patients gave informed consent.
failure, and stroke (1–3). Various pathophysiologic mechanismsin sleep apnea have been proposed to contribute to the pathogen-
Polysomnography
esis of vascular morbidity (4, 5). Repetitive episodes of hypo-
Subjects underwent overnight polysomnography in the sleep laboratory
xemia, hypercarbia, sympathetic activation, and intrathoracic
(Alice 3 Diagnostics System; Respironics, Murrysville, PA) as pre-
pressure swings in OSA (6–8) may trigger cellular and biochemi-
viously described (19). Sleep data and respiratory events were manually
cal processes, which predispose to atherosclerosis (9–12).
scored according to established criteria (20–22). AHI referred to theaverage number of apneas and hypopneas per sleep hour.
Endothelial dysfunction has been found to occur in response
to cardiovascular risk factors and to precede or accelerate the
Echocardiography and Vascular Reactivity Study
development of atherosclerosis (11, 12). It has also been shown
Standard two-dimensional and Doppler echocardiogram was performed
to have a clear predictive value for future cardiovascular disease
at baseline. The method for measuring endothelium-dependent and
(13, 14). Impairment of endothelium-dependent vasodilation,
endothelium-independent brachial artery dilation has been described
which is mainly mediated by nitric oxide, has been reported in
previously (23). The brachial artery diameter was measured on B-mode
OSA (15–18). We have previously shown that circulating nitric
ultrasound images, with a 7.0-MHz linear-array transducer and Acuson
oxide levels were decreased in OSA, and this could be reversed
128XP/10 system (Mountain View, CA). Longitudinal scans of the bra-
by application of overnight nasal continuous positive airway pres-
chial artery were obtained at rest, then during reactive hyperemia pro-
sure (nCPAP) (19). We hypothesize that OSA contributes to
duced by inflation of a pneumatic tourniquet placed on the forearm
endothelial dysfunction. The present study was undertaken to
followed by release, and finally after sublingual nitroglycerin (NTG)spray. FMD and NTG-induced dilation were defined as the percentagechange in diameter between the initial scan and after cuff deflation andNTG, respectively. Doppler-derived arterial flow was also measured atrest, during hyperemia, and after sublingual NTG, as described pre-
(Received in original form June 10, 2003; accepted in final form October 7, 2003)
viously (23). All scans were performed by H-F.T., who was blinded to
Supported by grant no. 7307/00, Hong Kong Research Grants Council.
the status of sleep-disordered breathing or treatment of the subjects.
Correspondence and requests for reprints should be addressed to Mary S. M. Ip,
Statistical Analysis
M.D., Department of Medicine, The University of Hong Kong, Queen Mary Hospi-tal, Pokfulam Road, Hong Kong SAR, China. E-mail: [email protected]
Continuous data were given as mean Ϯ SD. Between-group compari-
This article has an online supplement, which is accessible from this issue’s table
sons for continuous variables were made by Mann-Whitney U test and
of contents online at www.atsjournals.org
t test. Multiplicity of comparisons among groups was accounted byusing Bonferroni correction. Within-group comparisons for continuous
Am J Respir Crit Care Med Vol 169. pp 348–353, 2004 Originally Published in Press as DOI: 10.1164/rccm.200306-767OC on October 9, 2003
variables were made by Wilcoxon signed rank test and Friedman test
Internet address: www.atsjournals.org
and for categorical variables by chi-square test. Associations between
Ip, Tse, Lam, et al.: Endothelial Dysfunction in Sleep Apnea
FMD and continuous parameters were described by Spearman’s rank
Echocardiography and Vascular Reactivity Study
correlation coefficient and between FMD and categorical variables by
Echocardiography did not demonstrate any overt abnormality
Fisher’s exact test. Forward stepwise linear regression with baselineFMD as dependent variable was done. Deleted studentized residuals
in all subjects, with left ventricular ejection fraction at 67.3 Ϯ
of the regression model were examined for validity of model assump-
7.0%. At baseline, subjects with OSA had significantly lower
tions. A two-sided p value of less than 0.05 was considered statistically
FMD at 5.3 Ϯ 1.7% compared with subjects without OSA at
significant. Statistical analysis was made with SPSS for Windows (ver-
8.4 Ϯ 1.0%, with a mean difference of 3.03% (p Ͻ 0.001; 95%
sion 11.0.1; SPSS, Inc., Chicago, IL).
confidence interval, 1.96–4.1%). NTG-induced dilation was simi-lar at 15.7 Ϯ 4.0% in subjects with OSA and 17.7 Ϯ 4.6% in
those without OSA (p ϭ 0.17) (Table E4).
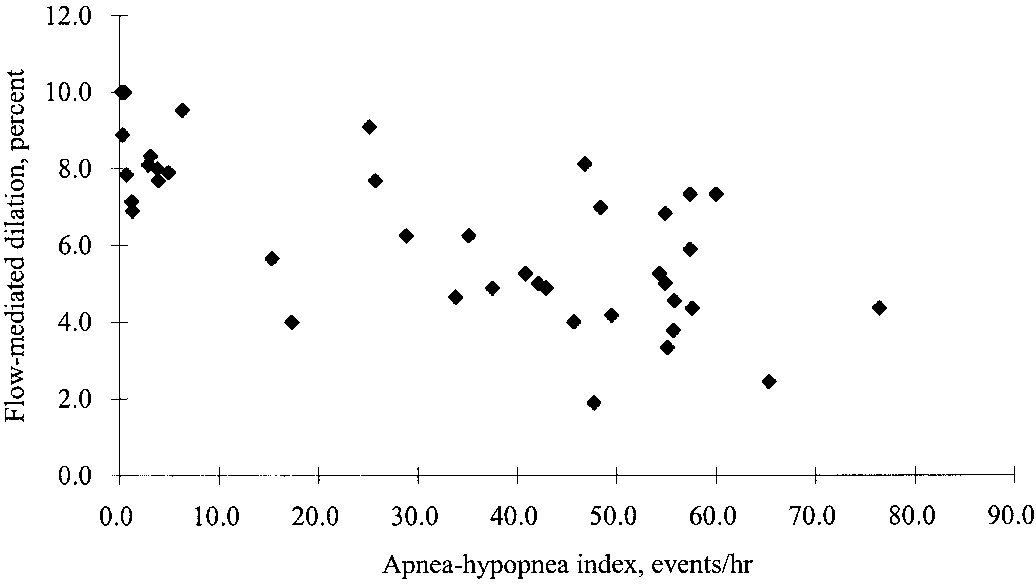
Correlation analysis (n ϭ 40) showed that FMD correlated
Patient Characteristics
negatively with AHI (r ϭ Ϫ0.655, p Ͻ 0.001) (Figure 1), time
Twenty-eight men with OSA (AHI, 46.0 Ϯ 14.5) were recruited
with oxygen saturation of less than 90% (r ϭ Ϫ0.620, p Ͻ 0.001),
and randomized to treatment (nCPAP) group and the control
and arousal index (r ϭ Ϫ0.516, p ϭ 0.001) and positively with
(observation) group, and 12 men without OSA (AHI 2.4 Ϯ 2.0),
minimum oxygen saturation (r ϭ 0.577, p Ͻ 0.001). FMD did
matched to OSA group for body mass index, were recruited.
not show significant correlation with age, body mass index, waist
Their baseline characteristics are shown in Table 1 and Table E1
circumference, lipids, glucose, blood pressure, and Epworth
All subjects in the nCPAP group completed the 4-week evalu-
Stepwise multiple linear regression analysis showed that AHI
ation, but one subject in the control group withdrew (he decided
and age were significant determinants of baseline FMD, indepen-
to use nCPAP). Objective data on use of nCPAP during the
dent of body mass index, diastolic blood pressure, total choles-
4 weeks averaged 4.3 hours per night. The two groups were
terol, and smoking status (Table 3). When AHI was replaced
comparable at baseline, and both groups had no significant
by other sleep parameters (time with oxygen saturation of less
change in anthropometric and metabolic profile over the 4-week
than 90%, minimum oxygen saturation, arousal index), the sleep
study period (Table E2 in online supplement). Diastolic blood
indices were shown up as significant determinants of FMD, re-
pressure decreased in the nCPAP group (77.9 Ϯ 11.1 to 69.2 Ϯ
spectively (Table E5 in online supplement).
15.2 mm Hg, p ϭ 0.04) but not in the control group.
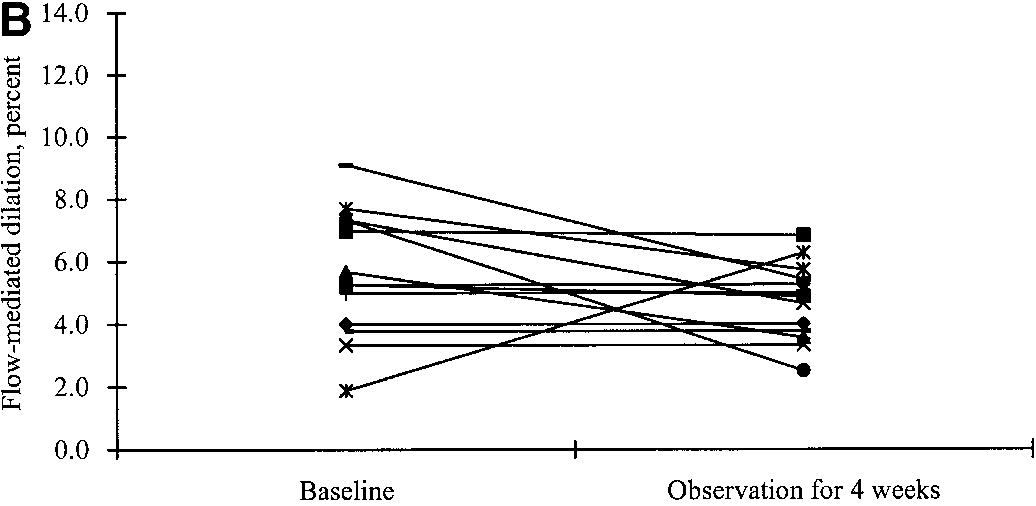
After 4 weeks, those who received nCPAP had a significant
Eight subjects who have used nCPAP for a median duration
increase in FMD from 5.1 Ϯ 1.4% to 9.6 Ϯ 1.6% (p ϭ 0.001)
of 15 weeks, range of 12–30 weeks, were reassessed after stopping
(Figure 2A), whereas those on observation had no significant
nCPAP for 1 week. Self-reported compliance to nCPAP was at
change from 5.6 Ϯ 2.0% to 4.7 Ϯ 1.2% (p ϭ 0.12) (Figure 2B).
an average of 5 nights per week, 4.2 hours per night. There was
The between-group difference of the change in FMD was highly
no significant change in anthropometric, metabolic profile, and
significant (4.5% vs. Ϫ0.9%, difference of 5.4%, p Ͻ 0.001). Both groups had no significant change in NTG-induced dilation,
blood pressure during the study period (see Table E3 in online
and the between-group difference of the change in NTG-induced
dilation was not significant (1.5% vs. 1.1%, difference of 0.4%,
Polysomnography Data
p ϭ 0.67) (Table 4 and Table E6 in the online supplement).
In the eight subjects who further used nCPAP and then with-
At baseline, OSA patients had moderate to severe sleep-
drew for 1 week, FMD after nCPAP withdrawal was significantly
disordered breathing, with no significant difference between
lower than that at 4 weeks of nCPAP (on nCPAP 8.9 Ϯ 1.9%,
nCPAP and control group (Table 2). At 4 weeks, the treatment
off nCPAP 5.0 Ϯ 0.7%, p ϭ 0.02) and was similar to baseline
group demonstrated abolition of apneas and hypopneas while
(Figure 3). NTG-induced dilation showed no significant change
using nCPAP, and the control group showed little change from
at the three assessments (see Table E7 in online supplement).
The eight subjects who were further reassessed longitudinally
DISCUSSION
demonstrated no significant change in the severity of sleep-disordered breathing after several months compared with base-
The findings demonstrated that otherwise healthy subjects with
line (baseline vs. off treatment, AHI, 52.4 Ϯ 13.4 vs. 53.2 Ϯ 21.5;
OSA have impaired endothelium-dependent flow-mediated vaso-
minimum oxygen saturation, 64.0 Ϯ 10.9% vs. 66.3 Ϯ 16.2%;
dilation in the brachial artery compared with subjects without
time with oxygen saturation less than 90%, 112.9 Ϯ 79.5 vs.
OSA, and the endothelial dysfunction was reversed after treat-
91.6 Ϯ 78.5 minutes; all p Ͼ 0.05).
ment with nCPAP for 4 weeks. This improvement in endothelial
TABLE 1. BASELINE CHARACTERISTICS Definition of abbreviations: nCPAP ϭ nasal continuous positive airway pressure; OSA ϭ obstructive sleep apnea. No significant difference was detected between obstructive sleep apnea and normal subjects or between obstructive sleep
apnea–continuous positive airway pressure and obstructive sleep apnea–control groups.
AMERICAN JOURNAL OF RESPIRATORY AND CRITICAL CARE MEDICINE
TABLE 2. POLYSOMNOGRAM DATA OF OBSTRUCTIVE SLEEP APNEA SUBJECTS
Time with oxygen saturation of less than 90%, min
For definition of abbreviations see Table 1. * p р 0.001 for comparison between baseline and 4-week within the nasal continuous positive airway pressure group. No
significant differences were found within the control group.
† p р 0.001 for comparison between nasal continuous positive airway pressure and control groups at 4 weeks. No significant
differences were found between the two groups at baseline.
The obstructive sleep apnea–control group data excludes one patient who withdrew from study.
function was not sustained after stopping nCPAP treatment for
endothelial function in OSA have shown conflicting data.
1 week, despite previous use for several months.
Blunted vasodilation in response to infusion of acetylcholine, a
OSA syndrome is a global problem that occurs in 1–5% of
vasodilator that stimulates endothelial release of nitric oxide,
adult men and 1–2% of adult women of various ethnic popula-
was demonstrated in forearm resistance vessels using occlusion
tions (24). OSA has many adverse physiologic consequences that
plethysmography (15, 16), but not confirmed in a more recent
potentially constitute risks for development of cardiovascular
study (32). Impaired relaxation response to bradykinin in the
diseases. One of the postulated mechanisms is that it can precipi-
forearm venous vasculature has been reported, suggesting endo-
tate or accelerate atherosclerosis, although to date there is no
thelial dysfunction in the venous vasculature (18). Using ultra-
sound Doppler method similar to ours, impairment of FMD in
The vascular endothelium participates in control of various
the brachial artery was reported to correlate with minimum
vascular functions through regulation of vasoactive mediators
oxygen saturation in subjects with OSA (17). In contrast to
in response to physical or biochemical stimuli in the body. Endo-
our findings, another study found no significant difference in
thelial injury, at cellular level or tissue level, is an important
conduit–vessel dilation between sleep apnea and control subjects
initial event in atherogenesis, preceding thickening of intima
(16). In that study, subjects underwent conduit–vessel studies at
and formation of atherosclerotic plaques (11, 12). Endothelial
least 1 hour after resistance–vessel studies, which involved intra-arterial infusion of acetylcholine, nitroprusside and verapamil,
dysfunction has been detected in disease states characterized by
and residual effect of drugs on the vasculature, which affected
atherosclerosis (11, 12) and also in conditions that predispose
their response to reactive hyperemia, cannot be completely
to atherosclerosis such as hypercholesterolemia and cigarette
excluded. Recently, impaired hyperemic blood flow response mea-
smoking, indicating that it is a marker of early atherogenesis
sured by forearm plethysmography, an indicator of altered myo-
(23, 25, 26). Endothelial dysfunction was shown to have a pre-
genic and/or endothelial activity, was reported, and seven subjects
dictive value for cardiovascular events in patients with chest pain
showed improvement with use of nCPAP for 2 weeks (33).
and/or coronary artery disease (13, 14).
These studies have used different methods for evaluation
Various circulating markers of endothelial dysfunction (27),
of vascular endothelial function. The mechanisms of vascular
including nitric oxide, soluble cell adhesion molecules, fibrino-
response to vessel occlusion followed by reactive hyperemia are
gen, and plasminogen activator inhibitor, have been reported to
clearly complex, involving myogenic, neurogenic, and vasculo-
be altered in OSA (1, 10, 28–31). Previous studies on vascular
genic components, mediated by a variety of metabolic alterationsand vasoactive factors (34–36). The exact mechanisms appar-ently differ with vascular beds and evoking stimuli (35, 36). Usingsimilar techniques, hyperemic FMD in the brachial artery orother conduit vessels has been demonstrated to reflect endothe-lial function, mainly mediated by endothelial nitric oxide (37–39). The test has been shown to be accurate and reproducible (40). It is regarded as a useful surrogate in assessing predisposition
TABLE 3. STEPWISE MULTIPLE LINEAR REGRESSION MODEL OF BASELINE FLOW-MEDIATED DILATION* Figure 1. Correlation between baseline flow-mediated dilation of bra-
The excluded parameters include body mass index, diastolic blood pressure,
chial artery and apnea–hypopnea index in obstructive sleep apnea (OSA)
total cholesterol, and smoking history.
and subjects without OSA (n ϭ 40, r ϭ Ϫ0.655, p Ͻ 0.001).
Ip, Tse, Lam, et al.: Endothelial Dysfunction in Sleep Apnea
ences in the response to endothelium-independent smooth mus-cle vasodilators might emerge.
“Uncomplicated” central obesity has been reported to be
associated with impaired endothelial function (43), but the OSAstatus of those subjects has not been defined. We postulate thatthe endothelial dysfunction attributed to obesity was at leastpartly related to the presence of OSA in some of these subjects. In this study, OSA and subjects without OSA were matched forobesity, and the body mass index was not a significant indepen-dent determinant of FMD on multiple regression analysis. Thechange in FMD with treatment of OSA without any concomitantchange in body weight and the use of a control group who didnot receive nCPAP treatment provided further evidence thatthe improvement in endothelial function in this study sample,most of whom were obese, was attributed to the use of nCPAP,whereas a placebo effect could not be definitively excluded.
Hypertension is associated with endothelial dysfunction (25).
Our subjects were normotensive, although there was a trendfor higher diastolic blood pressure in subjects with OSA and asignificant decrease in those treated with nCPAP, findings thatwere consistent with previous studies of OSA (44). There arefew data regarding the effect of blood pressure within the normo-tensive range on endothelial function. Hence, the role playedby the differences in blood pressure, if any, in the changes inendothelial function seen in these subjects is not known. Figure 2. (A) Flow-mediated dilation of brachial artery in 14 subjects
Sleep debt per se has been reported to result in increased
with OSA at baseline and after 4 weeks of nasal continuous positive
sympathetic nervous system activity and decreased glucose
airway pressure (nCPAP), showing significant increase in flow-mediated
tolerance (45), which theoretically may lead to alterations in
dilation (p ϭ 0.001). (B) Flow-mediated dilation of brachial artery in
endothelial function. The lack of correlation between endothelial
13 subjects with OSA at baseline and after 4 weeks of observation,
function and sleepiness score, an indicator of sleep debt, appar-
showing no change in flow-mediated dilation (p ϭ 0.12).
ently did not support this speculation. However, our study wasnot designed to investigate this issue, and the relationship be-tween sleep debt and endothelial function remains to beexplored.
to coronary atherosclerosis because it has been shown to corre-
Endothelial nitric oxide plays a central role in endothelial func-
late closely with endothelium-dependent vasomotor response of
tion (46) and endothelium-dependent flow mediated vasodilation
of the brachial artery (36–38). Many pathogenetic mechanisms
We have not been able to demonstrate any significant change
that may impair endothelium-dependent nitric oxide–mediated
in response to NTG, which produces brachial artery dilation
vasodilation have been shown to be present in OSA. During
mediated by vascular smooth muscle, independent of the endo-
recurrent apneas and hypopneas, the vascular endothelium is
thelium (38). In studies of subjects with OSA, results of vascular
conceivably subjected to recurrent shear stress and hypoxemia–
smooth muscle function have been variable. Again, studies have
reoxygenation, which may result in decreased synthesis or en-
used different evaluation techniques. Two studies that used ultra-
hanced degradation of endothelial nitric oxide (10, 46), and
sound Doppler to evaluate the brachial artery did not show any
recent studies have demonstrated that circulating nitric oxide
impairment of NTG-induced vasodilation in subjects with OSA
levels were decreased in subjects with OSA (10, 19). Other
(16) nor correlation with any measure of sleep apnea (17) . In
mechanisms for impaired nitric oxide–mediated endothelial
studies using other methods, conflicting data have been reported.
function, including increased oxidant load, enhanced oxidation
One study showed heightened vasoconstrictor sensitivity in OSA
of low density lipoprotein, insulin resistance, and increased sym-
(32), whereas others did not demonstrate significant differences
pathetic activity (46, 47), have been demonstrated to be present
(15, 16, 18). However, the numbers of subjects in individual
studies, including ours, have been small, and it is possible that
Because recurrent hypoxia–reoxygenation is believed to be
with substantially larger numbers of subjects, significant differ-
a key process that triggers endothelial dysfunction in OSA, it is
TABLE 4. VASCULAR REACTIVITY OF BRACHIAL ARTERY IN OBSTRUCTIVE SLEEP APNEA SUBJECTS
For definition of abbreviations see Table 1. * p р 0.001 for within-group comparison between baseline and 4 weeks. † p р 0.001 for between-group comparison of changes at 4 weeks.
AMERICAN JOURNAL OF RESPIRATORY AND CRITICAL CARE MEDICINE
2. Peppard PE, Young T, Palta M, Skaturd J. Prospective study of the
association between sleep-disordered breathing and hypertension. N Engl J Med 2000;342:1378–1384.
3. Peker Y, Hedner J, Norum J, Kraiczi H, Carlson J. Increased incidence
of cardiovascular disease in middle-aged men with obstructive sleepapnea. Am J Respir Crit Care Med 2002;166:159–165.
4. Hedner JA, Wilcox I, Sullivan CE. Speculations on the interaction be-
tween vascular disease and obstructive sleep apnea. In: Saunders NA,Sullivan CE, editors. Sleep and breathing. New York: Marcell Dekker;1994. pp. 823–846.
5. Dean RT, Wilcox I. Possible atherogenic effects of hypoxia during ob-
structive sleep apnea. Sleep 1993;16:S15–S22.
6. Shepard JW Jr. Gas exchange and hemodynamics during sleep. Med ClinFigure 3. Serial changes in flow-mediated dilation of brachial artery at North Am 1985;69:1243–1264.
baseline, after 4 weeks of nCPAP, and 1 week after withdrawal of nCPAP
7. Zwillich C, Sinoway L. Surges of muscle sympathetic nerve activity during
obstructive apnea are linked to hypoxemia. J Appl Physiol 1995;79:
in eight subjects with OSA. After withdrawal of nCPAP, flow-mediated
dilation was lower than during treatment (p ϭ 0.02).
8. Somers VK, Kyken ME, Clary MP, Abbound FM. Sympathetic neural
mechanisms in obstructive sleep apnea. J Clin Invest 1995;96:1897–1904.
9. Xie A, Skatrud JB, Brabtree DC, Puleo DS, Goodman BM, Morgan BJ.
interesting to note that AHI instead of hypoxemia indices
Neurocirculatory consequences of intermittent asphyxia in humans.
showed the best predictive value for reduced FMD. The ideal
J Appl Physiol 2000;89:1333–1339.
parameter of stress quantification in sleep-disordered breathing
10. Lavie L. Obstructive sleep apnoea syndrome: an oxidative stress disorder.
is still to be delineated. AHI embraces some information of
Sleep Med Rev 2003;7:35–51.
11. Ross R. Atherosclerosis: an inflammatory disease. N Engl J Med 1999;
hypoxemia because of the defining criteria for apnea and hypo-
pnea and, in addition, indicates the frequency of events that
12. Shimokawa H. Primary endothelial dysfunction: atherosclerosis. J Mol
pose recurrent oxidative, mechanical, or neurohormonal stimuli. Cell Cardiol 1999;31:23–27.
It may therefore be able to reflect total endothelial stress due
13. Neunteuff T, Heher S, Katzenschlager R, Wolfl G, Kostner K, Maurer
to sleep-disordered breathing despite many limitations.
G, Weidinger F. Late prognostic value of flow-mediated dilation in
Some risk factor intervention or drug treatment have shown
the brachial artery of patients with chest pain. Am J Cardiol 2000;S6:207–210.
favorable effects on endothelial function, including smoking ces-
14. Vogel RA. Heads and hearts: the endothelial connection. Circulation
sation, lipid lowering drugs, antioxidants, and antihypertensive
drugs (14, 25, 37, 50). Some of these therapeutic maneuvers also
15. Carlson JT, Rangemark C, Hedner JA. Attenuated endothelium-depen-
result in a decrease in clinical ischemic events (50, 51), suggesting
dent vascular relaxation in patients with sleep apnoea. J Hypertens
that at least part of the observed clinical benefits may be related
to reversal of endothelial dysfunction. Our findings demon-
16. Kato M, Roberts-Thomson P, Phillips BG, Hayes WG, Winnicki M,
strated that nCPAP therapy can correct endothelial dysfunction
Accurso V, Somers VK. Impairment of endothelium-dependent vaso-dilation of resistance vessels in patients with obstructive sleep apnea.
in OSA, but the beneficial effect was not apparent on withdrawal
Circulation 2000;102:2607–2610.
of nCPAP for 1 week, despite previous treatment for several
17. Kraiczi H, Caidahl K, Samuelsson A, Peker Y, Hedner J. Impairment
months, suggesting that the endothelial dysfunction was related
of vascular endothelial function and left ventricular filling: association
to relatively acute pathophysiologic changes. However, our study
with the severity of apnea-induced hypoxemia during sleep. Chest
design does not allow more precise information to be derived
regarding the temporal relationship between changes in endo-
18. Duchna HW, Guilleminault C, Stoohs RA, Faul JL, Moreno H, Hoffman
BB, Blaschke TF. Vascular reactivity in obstructive sleep apnea syn-
drome. Am J Respir Crit Care Med 2000;161:187–191.
In summary, the findings of endothelium-dependent vascular
19. Ip MSM, Lam B, Chan LY, Zheng L, Tsang KWT, Fung PCW, Lam
dysfunction in otherwise healthy subjects with OSA and the re-
WK. Circulating nitric oxide is suppressed in obstructive sleep apnea
versibility of such dysfunction with treatment of sleep apnea lend
and is reversed by nasal continuous positive airway pressure. Am J
strong circumstantial evidence to an independent contribution of
Respir Crit Care Med 2000;162:2166–2171.
OSA to atherosclerosis. They also connotate the possibility that
20. Rechtschaffen A, Kales AA, editors. A manual of standardized terminol-
treatment of OSA may prevent its long-term cardiovascular mor-
ogy, techniques and scoring for sleep stages of human subjects. Wash-ington, DC: Government Printing Office; 1968. NIH Publication No.
bidity. However, the subjects in this study are men with moderate
to severe OSA, and findings may not extrapolate to those with
21. American Academy of Sleep Medicine Task Force. Sleep-related breath-
mild sleep apnea or to women. Furthermore, the study subjects
ing disorders in adults: recommendations for syndrome definition and
had no overt atherosclerotic disease, and it is not known whether
measurement techniques in clinical research. Sleep 1999;22:667–89.
endothelial dysfunction attributable to OSA will be similarly
22. American Sleep Disorders Association. EEG arousals: scoring rules and
reversible in those subjects who also have established hyperten-
examples. Sleep 1992;15:175–184.
23. Celermajer DS, Sorensen KE, Gooch VM, Spiegelhalter DJ, Miller OI,
sion or other atherosclerotic vascular diseases.
Sullivan ID, Lloyd JK, Deanfield JE. Non-invasive detection of endo-
Conflict of Interest Statement : M.S.M.I. has no declared conflict of interest; H-F.T.
thelial dysfunction in children and adults at risk of atherosclerosis.
has no declared conflict of interest; B.L. has no declared conflict of interest;
K.W.T.T. has no declared conflict of interest; W-K.L. has no declared conflict of
24. Young T, Peppard PE, Gottlieb DJ. Epidemiology of obstructive sleep
apnea. Am J Respir Crit Care Med 2002;154:1217–1239.
25. Celermajer DS. Endothelial dysfunction: does it matter? Is it reversible?
Acknowledgment : The authors gratefully acknowledge Dr. Daniel Fong, Senior J Am Coll Cardiol 1997;30:325–333.
Medical Statistician, Clinical Trials Centre, The University of Hong Kong, for expert
26. Reddy KG, Nair RN, Sheehan HM, Hodgson JM. Evidence that selective
statistical advice; Ms. Audrey Ip for technical assistance; and Ms. Agnes Lai andMs. Wendy Mok for assistance in statistical analysis.
endothelial dysfunction may occur in the absence of angiographic orultrasound atherosclerosis in patients with risk factors for atherosclero-sis. J Am Coll Cardiol 1994;23:833–843. References
27. Anderson TJ. Assessment and treatment of endothelial dysfunction in
1. Leung RS, Bradley TD. Sleep apnea and cardiovascular disease. Am J
human. J Am Coll Cardiol 1999;34:631–638. Respir Crit Care Med 2001;164:2147–2165.
28. Dyugovskaya L, Lavie P, Lavie L. Increased adhesion molecules expres-
Ip, Tse, Lam, et al.: Endothelial Dysfunction in Sleep Apnea
sion and production of reactive oxygen species in leukocytes of sleep
human endothelium-dependent arterial responses: accuracy and repro-
apnea patients. Am J Respir Crit Care Med 2002;165:934–939.
ducibility. Br Heart J 1995;74:247–253.
29. Ohga E, Nagase T, Tomita T, Teramoto S, Matsuse T, Katayama H,
41. Anderson TJ, Uehata A, Gerhard MD, Meredith IT, Knab S, Delagrance
Ouchi Y. Increased levels of circulating ICAM-1, VCAM-1, and
D, Lieberman EH, Ganz P, Creager MA, Yeung AC, et al. Close
L-selection in obstructive sleep apnea syndrome. J Appl Physiol 1999;
relation of endothelial function in the human coronary and peripheral
circulations. J Am Coll Cardiol 1995;26:1235–1241.
30. Wessendorf TE, Thilmann AF, Wang YM, Wang YM, Schreiber A,
42. Takase B, Uehata A, Akima Ta, Nagai T, Nishiioka T, Hamabe A,
Konietzko N, Teschler H. Fibrinogen levels and obstructive sleep
Satomura K, Ohsuzu F, Jurita A. Endothelium-dependent flow-medi-
apnea in ischemic stroke. Am J Respir Crit Care Med 2000;162:2039–
ated vasodilation in coronary and brachial arteries in suspected coro-nary artery disease. Am J Cardiol 1998;82:1535–1539.
43. Arcaro G, Zamboni M, Rossi L, Turcato E, Covi G, Armellini F, Bosello
31. Rangemark C, Hedner JA, Carlson JT, Gleerup G, Winther K. Platelet
O, Lechi A. Body fat distribution predicts the degree of endothelial
function and fibrinolytic activity in hypertensive and normotensive
dysfunction in uncomplicated obesity. Int J Obes Relat Metab Disord
sleep apnea patients. Sleep 1995;18:188–194.
32. Kraiczi H, Hedner J, Peker Y, Carlson J. Increased vasoconstrictor sensi-
44. Pepperell JC, Ramdassingh-Dow S, Crosthwaite N, Mullins R, Jenkinson
tivity in obstructive sleep apnea. J Appl Physiol 2000;89:493–498.
C, Stradling JR, Davies RJO. Ambulatory blood pressure after thera-
33. Imadojemu VA, Gleeson K, Quraishi SA, Kunselman AR, Sinoway LI,
peutic and subtherapeutic nasal continuous positive airway pressure
Leuenberger UA. Impaired vasodilator responses in obstructive sleep
for obstructive sleep apnoea: a randomised parallel trial. Lancet 2002;
apnea are improved with continuous positive airway pressure therapy. Am J Respir Crit Care Med 2002;165:950–953.
45. Spiegel K, Leproult R, Van Cauter E. Impact of sleep debt on metabolic
34. Engelke KA, Halliwill HR, Proctor DN, Dietz NM, Joyner MJ. Contribu-
and endocrine function. Lancet 1999;354:1435–1439.
tion of nitric oxide and prostaglandins to reactive hyperemia in the
46. Busse R, Fleming I. Regulation and functional consequences of endothe-
human forearm. J Appl Physiol 1996;81:1807–1814.
lial nitric oxide formation. Ann Med 1995;27:331–340.
35. Schubert R, Mulvany MJ. The myogenic response: established facts and
47. Hijmering ML, Stores ESG, Olijhoek J, Hutten BA, Blankestijn PJ,
attractive hypotheses. Clin Sci 1999;96:313–326.
Rabelink TJ. Sympathetic activation markedly reduces endothelium-
36. Joyner MJ, Dietz NM. Nitric oxide and vasodilation in human limbs.
dependent, flow-mediated vasodilation. J Am Coll Cardiol 2002;39:
J Appl Physiol 1997;83:1785–1796.
37. Raitakari OT, Celermajer DS. Flow-mediated dilatation. Br J Clin Phar-
48. Schulz R, Mahmoudi S, Hattar K, Sibelius ULF, Olschewski H, Mayer
K, Seeger W, Grimminger F. Enhanced release of superoxide from
38. Corretti MC, Anderson TJ, Benjamin EJ, Celermajer D, Charbonneau
polymorphonuclear neutrophils in obstructive sleep apnea: impact of
F, Creager MA, Deanfield J, Drexler H, Herman MG, Herrington
continuous positive airway pressure therapy. Am J Respir Crit CareMed 2000;162:566–570.
D, et al. Guidelines for the ultrasound assessment of endothelium-
49. Ip MS, Lam B, Ng MM, Lam WK, Tsang KWT, Lam KSL. Obstructive
dependent flow-mediated vasodilation of the brachial artery. J Am
sleep apnea is independently associated with insulin resistance. Am JColl Cardiol 2002;39:257–265. Respir Crit Care Med 2002;165: 670–676.
39. Joannides R, Haefeli WE, Linder L, Richard V, Bakkali EH, Thuillez C,
50. Modena MG, Bonetti L, Coppi F, Bursi F, Rossi R. Prognostic role
Luscher TF. Nitric oxide is responsible for flow-dependent dilatation of
of reversible endothelial dysfunction in hypertensive postmenopausal
human peripheral conduit arteries in vivo. Circulation 1995;91:1314–
women. J Am Coll Cardiol 2002;40:505–510.
51. Randomised trial of cholesterol lowering in 4,444 patients with coronary
40. Sorensen KE, Celermajer DS, Spiegelhalter DJ, Georgakopoulos D,
heart disease: the Scandinavian Simvastatin Survival Study (4S).
Robinson J, Thomas O, Deanfield JE. Noninvasive measurement of
Introduction This Code applies to United States circuit judges, district judges, Court of InternationalTrade judges, Court of Federal Claims judges, bankruptcy judges, and magistrate judges. Certain provisions of this Code apply to special masters and commissioners as indicated in the“Compliance” section. The Tax Court, Court of Appeals for Veterans Claims, and Court ofAppeals for the Arme
Il Corriere della Sera Martedì 15 Settembre 2009 Focus Come cambia la vita degli italiani La psicoterapeuta esperta in crisi familiari «Le coppie hanno meno pazienza di un tempo L'importante è ridere e progettare il futuro» ROMA — Alessandra Lancellotti (foto a de- molte opportunità ai maschi: il nostro Paese si è tificano con la propria madre (a una madre non stra), psic
 AMERICAN JOURNAL OF RESPIRATORY AND CRITICAL CARE MEDICINE
TABLE 2. POLYSOMNOGRAM DATA OF OBSTRUCTIVE SLEEP APNEA SUBJECTS
AMERICAN JOURNAL OF RESPIRATORY AND CRITICAL CARE MEDICINE
TABLE 2. POLYSOMNOGRAM DATA OF OBSTRUCTIVE SLEEP APNEA SUBJECTS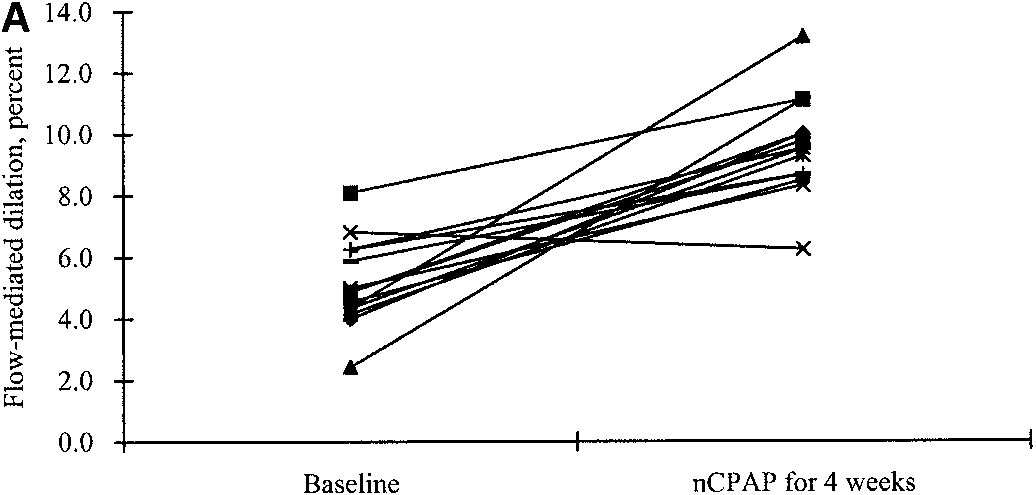
 Ip, Tse, Lam, et al.: Endothelial Dysfunction in Sleep Apnea
ences in the response to endothelium-independent smooth mus-cle vasodilators might emerge.
Ip, Tse, Lam, et al.: Endothelial Dysfunction in Sleep Apnea
ences in the response to endothelium-independent smooth mus-cle vasodilators might emerge.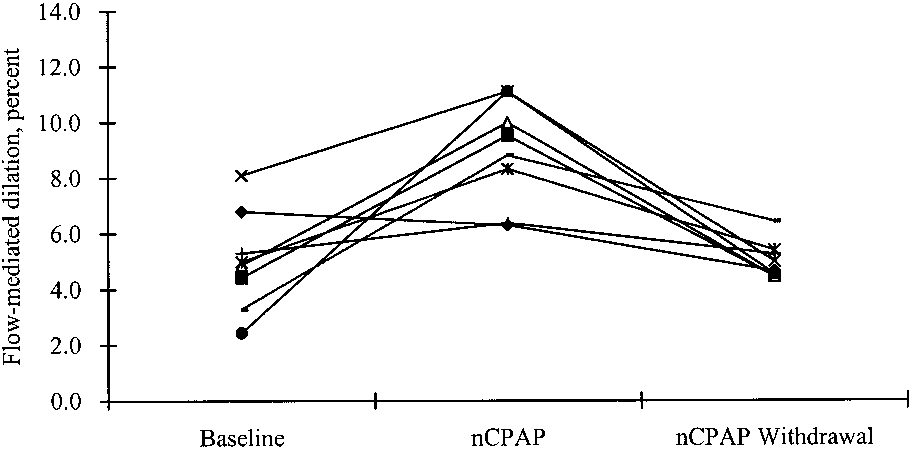 AMERICAN JOURNAL OF RESPIRATORY AND CRITICAL CARE MEDICINE
2. Peppard PE, Young T, Palta M, Skaturd J. Prospective study of the
association between sleep-disordered breathing and hypertension.
AMERICAN JOURNAL OF RESPIRATORY AND CRITICAL CARE MEDICINE
2. Peppard PE, Young T, Palta M, Skaturd J. Prospective study of the
association between sleep-disordered breathing and hypertension.