Early patient outcomes after primary and revision total knee arthroplasty A PROSPECTIVE STUDY R. C. Hartley, N. G. Barton-Hanson, R. Finley, R. W. Parkinson From Arrowe Park Hospital, Upton, England There has been speculation as to how the outcome those after primary TKA, varying between 37% and of revision total knee arthroplasty (TKA)
89%.1-30 Many of the series were retrospective, included
compares with that of primary TKA. We have
small numbers of patients and involved numerous surgeons
collected data prospectively from patients operated
using a variety of prostheses in different hospitals. In this
on by one surgeon using one prosthesis in each
study we have assessed prospectively the outcome of revi-
group. One hundred patients underwent primary
sion and primary TKA performed by a single surgeon, in
TKA and 60 revision TKA. They completed SF-12
one hospital, using a single design of implant in each
and WOMAC questionnaires before and at six and 12
group. The outcome measures which we used were the
months after operation.
generic short-form health questionnaire (SF-12)31 and the
The improvements in the SF-12 physical scores and
disease-specific Western Ontario and McMasters osteo-
WOMAC pain, stiffness and function scores in both primary and revision TKA patients were highly
The primary prosthesis was a modular, cruciate-retaining
statistically significant at six months. There was no
implant. The femoral component was porous-coated and
statistically significant difference in the size of the
uncemented. The tibial component was cemented and the
improvement in the SF-12 physical and WOMAC
patella was resurfaced with a cemented polyethylene but-
pain, stiffness and function scores between the
ton. The revision implant used a fluted, canal-filling,
primary and revision patients at six months after
cementless stem to obtain a press-fit with augments and/or
surgery. The SF-12 mental scores of patients in both
wedges to address bony deficiency. The stem was 95 mm
groups showed no statistically significant difference
long in most cases. Occasionally, we used a short tapered
after surgery at the six- and 12-month assessments.
stem if the bone stock was good or a 140 mm canal-filling
Our findings show that primary and revision TKA
stem if there was major osteolysis. The patella was resur-
lead to a comparable improvement in patient-
faced whenever possible. If the bone stock was poor or the
perceived outcomes of physical variables in both
patella too thin it was not resurfaced. The housing of both
generic and disease-specific health measures at
femoral and tibial components was cemented in all cases. follow-up at one year.
The insert used was either posterior-stabilised or varus-valgus-constrained (Fig. 1). J Bone Joint Surg [Br] 2002;84-B:994-9. Received 6 July 2001; Accepted after revision 3 April, 2002
The revision TKAs were performed for failure of the
primary Accord implant (Thackray, Leeds, UK) (Fig. 2). The causes of failure included aseptic loosening, wear of
There has been speculation as to how the outcome of
polyethylene, meniscal subluxation and instability, mal-
revision total knee arthroplasty (TKA) compares with that
alignment and patellofemoral maltracking.
of primary TKA. The former is technically demanding andthe rates of satisfactory results have not been as high as
We included in the study all patients undergoing revision
R. C. Hartley, FRCS Ed, Specialist Registrar
TKA between 1997 and 2000 and 100 consecutive patients
R. Finley, MSc, Advanced Nurse Practitioner
R. W. Parkinson, FRCS Orth, Consultant Orthopaedic Surgeon
undergoing primary TKA between 1997 and 1999, in 85 for
Department of Orthopaedics, Arrowe Park Hospital, Arrowe Park Road,
osteoarthritis and in 15 for rheumatoid arthritis. In the
revision group there were 35 women and 25 men with a
N. G. Barton-Hanson, FRCS Orth, Consultant Orthopaedic Surgeon
University Hospital Aintree, Lower Lane, Liverpool L9 7AL, UK.
mean age at surgery of 75 years (57 to 88) and in theprimary group 54 women and 46 men with a mean age of
Correspondence should be sent to Mr R. C. Hartley at Beach View, 36
Seabank Road, Lower Heswall, Wirral CH60 4SW, UK.
2002 British Editorial Society of Bone and Joint Surgery
All the operations were performed by the senior author
(RWP). The prosthesis used in the primary TKA was the
EARLY PATIENT OUTCOMES AFTER PRIMARY AND REVISION TOTAL KNEE ARTHROPLASTY
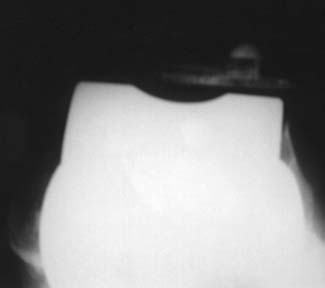
Radiographs showing a) anteroposterior, b) lateral and
c) skyline views of the Co-Ordinate revision TKA with
canal-filling inserts on the femoral and tibial
Radiographs showing a) anteroposterior (AP), b) lateral and c) skyline views of the Accord TKA. There is a loose, extended femoral
component, patellar maltracking and patella baja. Osteolysis is present in the lateral femoral condyle with a ‘crescent sign’ on the AP
Anatomic Modular Knee (AMK-DePuy, Warsaw, Indiana).
health (mental component summary scale - MCS). It is a
The Co-Ordinate prosthesis (DePuy) was used for revision
reliable and validated outcome measure.
surgery until 1999 and the Co-Ordinate Ultra prosthesis
The disease-specific WOMAC questionnaire is also a
(DePuy) thereafter. The latter had screw-on stems as
reliable and validated outcome measure. It was developed
opposed to the taper-fit stems of the Co-Ordinate
to assess outcomes in studies of osteoarthritis of the hip and
knee32,33 and consists of three areas: pain (five items),
All the patients were interviewed and completed the SF-
stiffness (two items) and function (17 items). The total
12 and WOMAC questionnaires before and at six and 12
score is obtained by summating the individual scores, but
the individual scores allow assessment of changes in the
The SF-12 generic health status questionnaire is derived
separate variables. The responses were entered into a data-
from the SF-36 questionnaire.31 It is used to assess overall
base. The SF-12 PCS and MCS health summary scales
health status and measures two components, physical health
were calculated using the SF-12 interpretation manual34
(physical component summary scale - PCS) and mental
and changes in the WOMAC score were determined.
R. C. HARTLEY, N. G. BARTON-HANSON, R. FINLEY, R. W. PARKINSON
Statistical analysis. We used the SPSS statistical software
package (SSPS Inc, Chicago, Illinois). For between-groupcomparisons (primary versus revision TKA) a two-way
WOMAC scores. Table I gives the mean scores and the
hierarchical repeated measures analysis of variance (ANO-
mean changes in scores with 95% confidence intervals.
VA) was performed and for within-group comparisons
There was no significant difference in the preoperative
(primary and revision separately) a simple repeated-
score between the two groups using an unpaired t-test
measures ANOVA. Only if the results of the latter were
(pain, p = 0.697; stiffness, p = 0.978; function, p =
significant were paired t-tests performed to compare pairs
of times using a Bonferroni post-hoc adjustment to the p
Two-way hierarchical repeated-measures ANOVA of the
value to avoid spurious results. Since the changes in the
mean scores showed that they were significantly different
mean scores from before operation to 6 and to 12 months
over time in both groups (p < 0.001). When applied to the
after operation are of interest, a two-way hierarchical
change in score there was no significant difference in the
repeated-measures ANOVA was used for between-group
magnitude of the changes in pain, stiffness and function
comparisons. The within-group comparisons of the change
scores between the preoperative and 6-month and between
in score either preoperative to 6 months or preoperative to
the preoperative and 12-month assessments (ANOVA F
12 months were evaluated using a paired t-test.
values for pain change = 0.029, p = 0.864; for stiffness
Preliminary analysis of the data showed that the mean
change = 1.543, p = 0.216; for function change = 0.764, p
scores and changes in scores over time had a normal
= 0.383). Comparison between the two groups showed that
distribution. A p value < 0.05 was taken to be significant.
the revision patients had significantly higher pain and
Table I. Mean scores with mean changes in score, 95% confidence intervals and post-hoc adjusted Bonferroni t-test results of pairs of times after simple repeated-measures ANOVA Revision Mean (95% CI) Mean (95% CI)
*post-hoc Bonferroni t-test
EARLY PATIENT OUTCOMES AFTER PRIMARY AND REVISION TOTAL KNEE ARTHROPLASTY
function scores (p < 0.001) but not stiffness scores (p =
groups (p < 0.001) but not between groups (p = 0.618). The
0.168). The improvements in the pain, stiffness and func-
preoperative PCS score was significantly higher in the
tion scores over time were statistically significant in both
primary group than in the revision group using an unpaired
groups (ANOVA F values for primary pain = 545.6, stiff-
t-test (p = 0.012). In both groups there were statistically
ness = 112.9, function = 376.8, p < 0.001; for revision pain
significant improvements in the PCS score with time on
= 69.8, stiffness = 35.7, function = 36.7, p < 0.001).
analysis by a simple repeated-measures ANOVA (primary
In the primary group, only pain and function scores
F = 19.6, p < 0.001, revision F = 7.4, p = 0.008). Bonferro-
improved significantly between 6 and 12 months (p = 0.026
ni post-hoc adjusted t-tests on pairs of times showed sig-
and p = 0.002, respectively). There was no significant
nificant changes between the preoperative and 6-month
improvement in any of the scores in the revision group
assessment (primary p < 0.001, revision p < 0.001) and the
between 6 and 12 months. The changes in pain and func-
preoperative and 12-month assessment (primary p < 0.001,
tion scores in the primary group were significantly greater
revision p < 0.001). There was no significant change in
than those in the revision group between 6 and 12 months
score in either group between 6 and 12 months (primary p
(pain F = 20.160, p = 0.009 and function F = 20.714, p <
Two-way hierarchical repeated-measures ANOVA of the
Comparison of the magnitude of the changes in scores
changes in score between the preoperative and 6-month and
from the preoperative to the 6-month assessment, using
preoperative and 12-month assessments for the between-
unpaired t-tests, revealed no significant differences between
group comparisons showed that there was no significant
the two groups (pain p = 0.056, stiffness p = 0.208,
difference in the size of the changes in the PCS score
function p = 0.079). Comparison of the changes in scores
between primary and revision patients (F = 0.467, p =
within the two groups using paired t-tests showed that the
0.495) or between the preoperative and 6-month and pre-
magnitude of change in pain, stiffness and function scores
operative and 12-month assessments (F = 0.354, p = 0.553).
was greater in the preoperative to 6-month period than in
Comparison of the size of the changes in score from the
the 6- to 12-month period (Table II).
preoperative to 6-month assessment, using unpaired t-tests,
SF-12 scores
showed no significant differences between the two groups
PCS. Table I gives the mean scores and the mean changes
in scores with 95% confidence intervals. Two-way hier-
Comparison of the changes in scores within the two
archical repeated-measures ANOVA of the scores showed
groups using paired t-tests showed that the size of the
that they were significantly different over time in both
change in score is greater in the preoperative to 6-monthperiod than in the 6- to 12-month period (primary p = 0.006and revision p = 0.004) (Table II). Table II. Results of paired t-test for comparison of changes of score MCS. Analysis of the MCS scores using a two-way hierar-
within groups between the preoperative and 6-month assessment and the
chical repeated-measures ANOVA showed no significant
6- and 12-month assessment with mean differences in change between thetime periods, 95% confidence intervals and t values
difference between the two groups (p = 0.489) or with time(p = 0.79). Revision
Revision TKA is a technically difficult procedure. Expo-
sure can be difficult because of stiffness and adhesions. In
addition, there is often instability due to ligamentous laxity
and the bone stock may be poor. The results of revision
surgery have not matched those of primary TKA.1-30 Our
aim in this prospective study was to evaluate the results of
revision TKA performed by one surgeon, using one pros-
thesis and compare them with those in a group of primary
TKA patients operated on by the same surgeon using one
prosthesis during the same time period. The revision TKAs
were performed for failure of the primary Accord implant
which was locally popular but not successful in terms of
There have been many studies which have determined
the effectiveness of TKA in reducing pain and deformity
and improving function.35-41 Most have assessed out-
comes using standardised knee scoring systems such as
the Hospital for Special Surgery (HSS) score or The
R. C. HARTLEY, N. G. BARTON-HANSON, R. FINLEY, R. W. PARKINSON
Knee Society score (KSS).38,41-47 These have not been
however, continued improvement in stiffness scores in the
validated and are surgeon-specific. They have poor
revision patients, but this was not statistically significant.
internal reliability and small effect sizes and are there-
This is not the case in terms of the SF-12 generic health
fore not good for assessing outcomes in TKA.48 This
measure, as both groups attain maximum improvements at
casts doubt on the validity of the results of these studies.
six months after surgery. This may be because the
Several papers have specifically considered the out-
WOMAC outcome measure is designed to be maximally
sensitive in patients with knee symptoms as a result of
The outcome measures which we have used (SF-12 and
osteoarthritis, whereas the SF-12 is intended to address a
WOMAC) are reliable and validated scoring sys-
wide range of health problems and is therefore less
tems.31-33,48 To our knowledge, no study has been pub-
specific.52 The mental scores of patients in both groups
lished which has prospectively assessed patient-perceived
showed no statistically significant improvement after the
outcomes after revision TKA and compared them with
operation. Also, there was no statistically significant differ-
ence in the mental scores before and after operation
Anderson et al51 showed a significant correlation between
between the primary and revision groups. Thus, the com-
the SF-36 score, the WOMAC pain and function scores and
monly held perception that mental state and sense of well-
patient satisfaction. Those patients with better WOMAC
being are improved after TKA is not true. This may be
function scores also had higher SF-36 physical scores, indi-
because patients’ poor preoperative mental state reflects
cating a relationship between improved knee function and
their type of personality rather than their physical prob-
improved overall function. The HSS score did not correlate
lems. We aim to perform further research into this area by
with patient satisfaction. Neither the HSS nor the KSS scores
attempting to identify a correlation between high pre-
showed any correlation with the WOMAC pain score, the SF-
operative SF-12 mental scores and high postoperative SF-
36 bodily pain score or patient satisfaction.
Our findings show no significant difference in the pre-
We conclude that revision TKA leads to a comparable
operative WOMAC scores between the two groups. The
improvement in both generic health outcome measures
revision patients, however, had worse preoperative PCS
and disease-specific outcome measures as does primary
scores than the primary patients. This may be due to the
fact that they already had had surgery on their knees using
No benefits in any form have been received or will be received from a
commercial party related directly or indirectly to the subject of this
We have also shown that the improvements in SF-12
PCS and WOMAC pain, stiffness and function scores inprimary and revision TKA are highly statistically sig-
nificant at the six-month assessment. There was no statis-
1. Ahlberg A, Lunden A. Secondary operations after knee joint replace-
tically significant difference in the size of the mean
ment. Clin Orthop 1981;156:170-4.
improvement from the preoperative to the six-month
2. Bargar WL, Cracchiolo AI, Amstutz HC. Results of constrained
total knee prosthesis in treating severely disabled patients and patients
assessment between the primary and revision patients in
with failed total knee replacements. J Bone Joint Surg [Am]
SF-12 PCS scores and WOMAC pain, stiffness and func-
tion scores. This indicates that in terms of patient-perceived
3. Bertin KC, Freeman MAR, Samuelson KM, Ratcliffe SS, Todd RC. Stemmed revision arthroplasty for aseptic loosening of total knee
outcome measures, revision TKA leads to as great an
replacement. J Bone Joint Surg [Br] 1985;67-B:242-8.
improvement as does primary TKA. Both groups of
4. Brady TA, Ranawat CS, Kettelkamp DB, Rapp GF. Salvage of the
patients showed a statistically significant improvement in
failed total knee arthroplasty. Orthop Trans 1977;1:101-2.
WOMAC pain, stiffness and function scores and SF-12
5. Bryan RS, Rand JA. Revision total knee arthroplasty. Clin Orthop
PCS scores between the preoperative and 12-month assess-
6. Cameron HU, Hunter GA. Failure in total knee arthroplasty: mecha-
ments. There was no significant change in SF-12 MCS
nisms, revisions, and results. Clin Orthop 1982;170:141-6.
scores in either group over this period of time. 7. Donaldson WF III, Sculco TP, Insall JN, Ranawat CS. Total
condylar III knee prosthesis: long-term follow-up study. Clin Orthop
There was no significant change in SF-12 PCS scores in
either group between 6 and 12 months. This indicated that
8. Dupont JA, Campbell ED Jr, Lumsden RM. Total knee arthroplasty
the patients had reached an ‘end-stage’ in recovery of
revisions. Orthop Trans 1980;4:321-2.
generic physical health status at six months. However, in
9. Friedman RJ, Hirst P, Poss P, Kelley K, Sledge CB. Results of
revision total knee arthroplasty performed for aseptic loosening. Clin
the WOMAC pain and function areas, the primary patients
continue to improve up to 12 months, whereas the revision
10. Goldberg VM, Figgie MP, Figgie HE, Sobel M. The results of
revision total knee arthroplasty. Clin Orthop 1988;226:86-92.
patients did not improve significantly between the 6- and
11. Hanssen AD, Rand JA. A comparison of primary and revision total
knee arthroplasty using the Kinematic Stabilizer prosthesis. J Bone
The perception among knee surgeons is that a TKA will
Joint Surg [Am] 1988;70-A:491-9.
continue to improve up to 12 months after surgery. We have
12. Hood RW, Insall JN. Total knee revision arthroplasty: indications,
surgical techniques and results. Orthop Trans 1981;5:412-3.
shown that this is true of the primary patients in terms of
13. Insall JN, Dethmers DA. Revision of total knee arthroplasty. Clin
pain and function but not of revision patients. There is,
EARLY PATIENT OUTCOMES AFTER PRIMARY AND REVISION TOTAL KNEE ARTHROPLASTY
14. Insall JN, Lachiewicz PF, Burstein AH. The posterior stabilized 33. Bellamy N, Buchanan WW, Goldsmith CH, Campbell J, Stitt LW.
condylar prosthesis: a modification of the total condylar design: two to
Validation study of WOMAC: a health status instrument for measuring
four-year clinical experience. J Bone Joint Surg [Am]
clinically important patient relevant outcomes to antirheumatic drug
therapy in patients with osteoarthritis of the hip or knee. J Rheumatol15. Jacobs MA, Hungerford DS, Krackow KA, Lennox DW. Revision
total knee arthroplasty for aseptic failure. Clin Orthop34. Ware JE Jr, Kosinski M, Keller S. SF-12: how to score the SF-12
physical and mental health summary scales. QualityMetric Incorporat-
16. Kim L, Finerman G. Results of revision for aseptic failed knee
arthroplasties. Orthop Trans 1983;7:535. 35. Goldberg VM, Figgie MP, Figgie HE, Heiple KG, Sobel M. Use of
a total condylar knee prosthesis for treatment of osteoarthritis and
17. Lewis JL, Askew MJ, Jaycox DP. A comparative evaluation of tibial
rheumatoid arthritis: long term results. J Bone Joint Surg [Am] 1988;
component designs of total knee protheses. J Bone Joint Surg [Am]36. Hungerford DS, Krackow KA. Total joint arthroplasty of the knee. 18. Rand JA, Bryan RS. Revision after total knee arthroplasty. Orthop Clin North Am 1982;13:201-12. 37. Insall JN, Scott WN, Ranawat CS. The total condylar knee pros- 19. Rand JA, Bryan RS. Results of revision total knee arthroplasties
thesis: a report of two hundred and twenty cases. J Bone Joint Surg
using condylar prostheses: a review of fifty knees. J Bone Joint Surg38. Insall JN, Hood RW, Flawn LB, Sullivan DJ. The total condylar 20. Rand JA, Peterson LF, Bryan RS, Ilstrup DM. Revision total knee
knee prosthesis in gonarthrosis: a five to nine-year follow-up of the
arthroplasty. Instr Course Lect 1986;35:305-18.
first one hundred consecutive replacements. J Bone Joint Surg [Am]21. Ritter MA. The Herbert total knee replacement: a longer than three
year follow-up. Clin Orthop 1977;129:232-5. 39. Murray DG. Total knee arthroplasty. Clin Orthop 1985;192:59-68. 22. Scuderi GR, Insall JN, Windsor RE, Moran MC. Survivorship of 40. Riley LH. Total knee arthroplasty. Clin Orthop 1985;192:34-9.
cemented knee replacements. J Bone Joint Surg [Br] 1989;71-B:798-
41. Stern SH, Bowen MK, Insall JN, Scuderi GR. Cemented total knee
arthroplasty for gonarthrosis in patients 55 years old or younger. Clin23. Stern SH, Insall JN. Total knee arthroplasty in obese patients. J Bone Joint Surg [Am] 1990;72-A:1400-4. 42. Cohn BT, Krackow KA, Hungerford DS, Lennox DW, Bachner 24. Thornhill TS, Dalziel RW, Sledge CB. Alternatives to arthrodesis for EJ. Results of total knee arthroplasty in patients 80 years and older.
the failed total knee arthroplasty. Clin Orthop 1982;170:131-40. 25. Thornhill TS, Hood RW, Dalziel RW, et al. Knee revision in failed 43. Insall JN, Binazzi R, Soudry M, Mestriner LA. Total knee arthro-
non-infected total knee arthroplasty: the Robert B. Brigham Hospital
plasty. Clin Orthop 1985;192:13-22.
and Hospital for Special Surgery experience. Orthop Trans 1982;
44. Insall JN, Dorr LD, Scott RD, Scott WN. Rationale of the Knee
Society clinical rating system. Clin Orthop 1989;248:13-4. 26. Vince KG, Long W. Press fit long stem revision total knee arthro-
plasty. Poster presentation. Annual Meeting of the Knee Society , New
45. Ranawat CS, Flynn WF, Saddler S, Hansraj KK, Maynard MJ.
Long term results of the total condylar knee arthroplasty: a 15-year
survivorship study. Clin Orthop 1993;286:94-102. 27. Walker PS, Greene D, Reilly D, et al. Fixation of tibial compo-
nents of knee prostheses. J Bone Joint Surg [Am] 1981;63-A:258-
46. Vince KG, Insall JN. Long term results of cemented total knee
arthroplasty. Orthop Clin North Am 1988;19:575-80. 28. Wertzberger KL, Bryan RS. Analysis of failed total knee arthro- 47. Vince KG, Insall JN, Kelly MA. The total condylar prosthesis: 10- to
plasty, excluding infection, undergoing reoperation. Orthop Trans
12-year results of a cemented knee replacement. J Bone Joint Surg29. Wilde AH, Schickendantz MS, Stulberg BN, Go RT. The incorpora- 48. Barton-Hanson NG. Outcome measures in total knee replacement.
tion of tibial allografts in total knee arthroplasty. J Bone Joint Surg
Poster presentation SICOT. Sydney, Australia, April 1999. 49. L’Insalata JC, Stern SH, Insall JN. Total knee arthroplasty in elderly 30. Su DHC, Chan CW, Seow KH, et al. Results of revision total knee
patients: comparison of tibial component designs. J Arthroplasty
arthroplasty. Singapore Med J 2000;41:6-8. 31. Stewart AL, Hays RD, Ware JE Jr. The MOS short-form general 50. Zicat B, Rorabeck CH, Bourne RB, Devance PA, Nott L. Total knee
health survey: reliability and validity in a patient population. Med
arthroplasty in the octogenarian. J Arthroplasty 1993;8:395-400. 51. Anderson JG, Wixson RL, Tsai D, Stulberg SD, Chang RW. 32. Bellamy N, Buchanan WW, Grace E. Double-blind randomized
Functional outcome and patient satisfaction in total knee patients over
controlled trial of isoxicam vs piroxicam in elderly patients with
the age of 75. J Arthroplasty 1996;11:831-40.
osteoarthritis of the hip and knee. Br J Clin Pharmacol 1986;22
52. Dawson J, Carr A. Outcomes evaluation in orthopaedics. J Bone Joint Surg [Br] 2001;83-B:313-5.
Emergency Contraception: A Cost-Effective Approach to Preventing Unintended Pregnancy 1 Professor of Economics and Public Affairs and Director, Office of Population Research, Princeton University, Wallace Hall, Princeton University, Princeton NJ 08544. Tel: 609-258-4946, Fax: 609-258-1039, Email: [email protected] 2 Women’s Health Center, UCSF Center for Reproductive Health
Information Regarding Your Upcoming Angiogram - UMass You are scheduled for an arteriogram (angiogram) with Dr. Stephen Hoenig at UMass Medical Center, 55 Lake Avenue North in Worcester, MA, scheduled for __________________________________. UMass will contact you the evening prior or morning of the scheduled procedure regarding arrival time. In preparation for your angiogram you should




 EARLY PATIENT OUTCOMES AFTER PRIMARY AND REVISION TOTAL KNEE ARTHROPLASTY
Radiographs showing a) anteroposterior, b) lateral and
c) skyline views of the Co-Ordinate revision TKA with
canal-filling inserts on the femoral and tibial
Radiographs showing a) anteroposterior (AP), b) lateral and c) skyline views of the Accord TKA. There is a loose, extended femoral
component, patellar maltracking and patella baja. Osteolysis is present in the lateral femoral condyle with a ‘crescent sign’ on the AP
Anatomic Modular Knee (AMK-DePuy, Warsaw, Indiana).
EARLY PATIENT OUTCOMES AFTER PRIMARY AND REVISION TOTAL KNEE ARTHROPLASTY
Radiographs showing a) anteroposterior, b) lateral and
c) skyline views of the Co-Ordinate revision TKA with
canal-filling inserts on the femoral and tibial
Radiographs showing a) anteroposterior (AP), b) lateral and c) skyline views of the Accord TKA. There is a loose, extended femoral
component, patellar maltracking and patella baja. Osteolysis is present in the lateral femoral condyle with a ‘crescent sign’ on the AP
Anatomic Modular Knee (AMK-DePuy, Warsaw, Indiana).