Edwin P. Su, MD Hospital for Special Surgery 535 East 70th Street New York, NY 10021 212-606-1128 Specializing in Joint Reconstruction Surface Replacement of the Hip
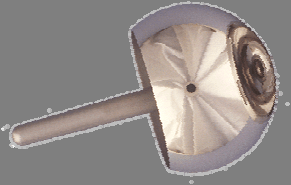
Surface replacement of the hip is an alternative to traditional hip replacement for the treatment of conditions such as osteoarthritis, avascular necrosis, and post-traumatic arthritis. It provides a bone-conserving artificial hip joint, and is designed to preserve bone for younger, active patients. The gold standard of the treatment of end-stage hip arthritis for the last 30 years has been a total hip replacement in which the upper part of the femur (the head and neck) are replaced with a stemmed device and prosthetic head (see below). The socket is replaced with a hemispherical shaped cup which usually contains a bearing surface of either metal, ceramic or polyethylene (plastic). Total hip replacement is an extremely successful operation that allows patients to return to pain-free activity and improve their quality of life. Unfortunately, over time prosthetic (artificial) hip implants can wear-out as well as loosen. When this occurs, patients encounter pain, a loss of functional ability and possibly even loss of bone. With both traditional hip replacement and surface replacement, the socket is inserted in a similar fashion. The two procedures differ in the way the femur is prepared. Whereas traditional hip replacement involves removing the head and neck of the femur, surface replacement preserves this bone (see picture). With a traditional hip replacement, after this bone is removed, a prosthesis with a stem is inserted within the thigh bone. With a surface replacement, the preserved bone is sculpted to accept a metal cap with a short stem. Traditional Total Hip Hip Resurfacing
The preservation of bone has several potential advantages. The first is that more bone is retained in the femur, should another hip replacement become necessary. Over time, any hip replacement may loosen or show signs of wear. In a young, active population, there is a high likelihood that more than one hip replacement operation will be necessary over the lifetime of the patient. It is a well documented principle that the more bone that remains during a revision hip operation, the greater chances of success. The second advantage to a surface replacement is that the preservation of bone allows for a much larger ball size. This allows for greater stability of the hip joint prior to dislocation. The dislocation rate after surface replacement of the hip is about 10 times lower than for a traditional hip replacement. General Risks of Hip resurfacing surgery Some of the risks of surgery of the hip include the loss of blood, formation of a clot in your leg, and the chance of infection. The overall incidence of these risks is very small. They should be discussed with your surgeon prior to proceeding with the operation. Some of the risks of having a prosthetic hip include the chance that the ball will dislocate (come out of the socket), the parts may loosen or wear out over time, or the prosthesis may become infected. As the hip prosthesis is a foreign body, it may become infected when there are bacterial infections elsewhere in the body. It is important for patients to be aware of this possibility and make other physicians and dentists aware about the presence of a hip prosthesis. Again, these issues will be discussed with you by your surgeon. Risks specific to surface replacement Metal ion dispersal The current generation of surface replacements are metal-on-metal bearings. That means both the ball and the socket are made entirely of metal. Although this cuts down dramatically on wearing out of the components, it has been shown to cause metal ions to be dispersed through the body. Cobalt and chromium ions are measurable in the blood stream, but have not been shown to cause cancer or any other disease in humans. Although the metal ions are measurable, no one knows what a safe level is. Generally, people with functioning kidneys are able to excrete the ions in their urine. There is also a rare possibility of developing a reaction to the metal particles that could result in pain or joint swelling. Femur fracture Because the bone of the femur is retained, it is possible to fracture it after surface replacement. Most of the fractures occur early in the post-operative period if too much weight is put on the leg too early. The body needs time to adapt to the new prosthesis. Post-operatively, crutches are used for 3-4 weeks to protect the amount of weight put on the leg. With current techniques and rehabilitation protocol, the risk of fracture is less than 2%. Nerve injury Working around the bone of the femur may cause extra pressure to be put on the nerves in the hip area, specifically the sciatic nerve. This may cause a transient weakness of some of the muscles of the leg in less than 1% of cases. Heterotopic ossification The hip resurfacing procedure may lead to extra bone forming around the hip, leading to stiffness, called heterotopic ossification. We now take measures to prevent this, using either a medication called Indocin, or one dose of radiation to the hip area after surgery. The radiation treatment, known as XRT (external radiation therapy), may be performed in the first 2 days after surgery and does not have any association with cancer. With XRT, the risk of extra bone forming is less than 2%. If Indocin is given to you, it will be a daily medication for 3 weeks post-operative. Unknowns of Surface Replacements Activity resumption
At this time, it is not clear what limitations of activity patient with surface
replacements should adhere to. With traditional bearing surfaces such as polyethylene or ceramics, repetitive impact has been associated with accelerated wear and even potential catastrophic breakage. Whether this will occur with the current metal-on-metal bearings such as those used in surface replacements is not known. Longevity of Implant
The short term results (4-6 year follow-up) of hip resurfacing are encouraging.
However, the early failures of hip resurfacing appears to be greater than for total hip replacement (2.2% vs 1.9%), with the majority of the early failures due to femoral neck fracture. Whether the newer forms of hip resurfacing will be successful long term is unknown. It may require 10 years or longer to determine whether this newer form of hip resurfacing is superior to total hip replacement at comparable time intervals. Recommendation Improvements in hip implant design as well as materials are frequent in joint replacement. Extensive prospective clinical trials over many years are necessary to determine the long term outcome and the true benefits and risks of new innovations. Should you be a candidate for hip replacement, a discussion regarding your options for treatment with your physician is recommended. There is no “right” answer as to whether total hip replacement or hip resurfacing is a better procedure for you. Only your surgeon can advise you on the option best suited for your unique circumstances and if necessary, which procedure is best for you. Details of the procedure The hip resurfacing is performed in an operating room with a special laminar airflow system, which helps reduce the chance of infection. Your surgeon will be wearing a “spacesuit”, also designed to reduce the chance of infection. The entire surgical team will consist of your surgeon, two to three assistants, and a scrub nurse. The anesthesia for a hip resurfacing is given through an epidural catheter, which is a small tube inserted into the back. This is the same type of anesthesia given to women in labor. You will be made numb from the waist down so that you will not feel anything. The catheter stays in for 1-2 days after the surgery to help with your post-operative pain control. During the course of the operation, you can be as awake or as sleepy as you want to be. After the epidural block is administered, you will be placed on your side. The incision for a total hip replacement is made along the side of your hip. The incision will measure anywhere from 6 to 10 inches depending upon your anatomy. It is well-covered by undergarments and is usually not visible when wearing clothes. The arthritic ball and socket are exposed and sculpted to accept the resurfacing implant. The socket is placed into the body without cement; over time your bone will grow onto the socket. The resurfacing ball is inserted with cement. During the closure, two drains are inserted around the operated area to assist with evacuation of blood. Staples and sutures are used to close the skin. The entire operation will take from 1.5 to 2 hours. Afterwards, you will be brought to the recovery room, where your blood work will be checked, and an x-ray of your new hip will be taken. Most patients can be brought to a regular room within a few hours; others will need to stay overnight in the recovery room, as determined by your surgeon and anesthesiologist. Patients generally stay in the hospital for 2-3 days following hip resurfacing surgery. Pre-operative orientation Most patients will be asked to donate 1 pint of their own blood in the weeks preceding hip resurfacing. This helps reduce the need for a blood transfusion from our blood bank. Almost all of the patients will receive the donated blood as a transfusion after surgery. Rarely, an additional transfusion is necessary from our blood bank. The blood from the blood bank is carefully screened to the best of our ability to detect any infectious diseases. You will be asked to see a medical doctor at HSS prior to your surgery. This is a precaution to make certain that you are healthy enough to undergo hip replacement surgery. In the course of this workup, you may be asked to have additional testing to examine your heart and lung function. After your surgery, this medical doctor will see you in the hospital. Post-operative course Immediately after hip resurfacing surgery, you will be in the recovery room. Most patients are able to go to a regular room after a few hours, when the sensation returns in your legs. You will be given a pain pump connected to your epidural catheter which will allow you to control when you are given pain medicine. Most people are quite comfortable with the pain pump in place.
On the day of surgery, you may do some of the exercises as instructed by your physical therapist, including buttock clenches and moving the feet up and down. You will be allowed to take some ice chips after surgery to wet your mouth, but drinking liquids or eating may cause you to become nauseated. You will have a catheter in your bladder so that you do not have to worry about urinating. Following the surgery, this is mainly a day of rest. The first day after surgery will have a lot of activity. You will meet our physiotherapists, who will instruct you in more exercises to perform while in bed. In addition, they will help you stand today and take a few steps with a walker. Generally, you will be allowed to drink clear liquids in the morning and regular food by the evening. The next day you will find it easier and easier to move about. You will be freed up from the pain and urinary catheters. Pain medication will be given in the form of tablets. Eventually you will progress to walking with 2 crutches, either under the armpit or forearm crutches. You will be discharged home when you have demonstrated that you can get in and out of bed and walk safely. A physiotherapist will come to your house to continue rehabilitation. A case manager will discuss these options with you and help you plan for your eventual return home. Your return to activity will be guided by your surgeon and therapists. After 3 weeks, you may transition to a single cane or crutch. Generally, patients are able to walk as much as they want by 6 weeks post-operatively. Patients are able to resume driving an automatic transmission at 3-4 weeks, as long as reaction times are normal and he/she is not requiring pain medication. At 8 weeks, patients are able to resume playing golf and swimming; at 12 weeks, they may play tennis. Your surgeon will help you decide what activities you may resume.
Approximate seed count (raw): 7,400 to 7,600 Soil temperature: 71 to 73°F (21 to 22°C) Light: Up to 2,500 f.c. (26,900 Lux) Moisture: Reduce soil moisture slightly (level 3 Key flowering facts: to 4) to allow the roots to penetrate into the • Vernalization: not required but beneficial as Fertilizer: Apply fertilizer at rate 1 (less than 100 flowering will occur 2 to
To Anticoagulate or not to Anticoagulate? A Common Dilemma for the Provider: Physicians’ Opinion Poll Based on a Case Study of an Older Long-term Care Facility Resident With Dementia and Atrial Fibrillation T.S. Dharmarajan, MD, FACP, AGSF, Surendran Varma, MD, Shailaja Akkaladevi, MD, Anna S. Lebelt, MD, andEdward P. Norkus, PhD, FACN Objective: Anticoagulation therapy is an acceptableT


 Edwin P. Su, MD
Edwin P. Su, MD