Nancy B. Davis, MDa, Ashesh B. Jani, MDb,
aDepartment of Medicine, Section of Hematology/Oncology, The University of Chicago Medical Center,
5841 South Maryland Avenue, MC2115, Chicago, IL 60637, USA
bDepartment of Radiation and Cellular Oncology, The University of Chicago Medical Center,
5841 South Maryland Avenue, MC 9006, Chicago, IL 60637, USA
cThe Ben May Institute for Cancer Research, The University of Chicago Cancer Research Center,
5841 South Maryland Avenue, MC 1140, Chicago, IL 60637, USA
Because of the widespread use of prostate-
Additionally, the PSA doubling time (PSADT)
specific antigen (PSA) for screening, most prostate
at the time of biochemical failure, with a cut-
cancers are now being detected in a localized stage;
off PSADT of less than 10 months, predicts for
therefore, most of the 190,000 men destined to be
the early development of distant metastasis and is
diagnosed with prostate cancer in 2002 are able to
predictive of death from prostate cancer [5,6].
undergo therapy with curative intent [1]. Parallel
Biochemical failure is defined differently after
with screening efforts have been efforts both in the
prostatectomy than after radiotherapy and gener-
surgery and radiotherapy arenas in technically
ally predates clinical failure by about 5 years. The
improving treatment. Specifically, bilateral nerve-
failure rate–biochemical or clinical–increases, of
sparing prostatectomy has improved the quality of
course, with advancing stage of disease. Following
life of surgery patients, and technical advances in
radical prostatectomy, 27% to 53% of men will
external beam radiation treatment (EBRT) plan-
experience biochemical (PSA only) failure within
ning (particularly intensity-modulated radiother-
10 years [5,7]. Biochemical relapse has been dem-
apy) and in low-dose rate (LDR) and high-dose rate
onstrated to be the single most sensitive sign of
(HDR) brachytherapy have allowed many options
treatment failure and probably identifies patients
to become available for treatment of early-stage
who fail to achieve eradication of disease years
prostate cancer. Such advances have allowed ex-
before clinically apparent recurrences [6]. Early use
cellent biochemical control rates for early-stage
of hormonal therapy, although widespread, has not
disease. Recurrence of prostate cancer remains
necessarily translated into increased survival [8].
a significant problem, however, with only 40% of
Choice of therapy following failed radical pros-
patients being disease-free at 15 years [2]. Pre-
tatectomy includes EBRT or a variety of hormonal
operative PSA levels of 10 or higher, positive sur-
manipulations. Therapies available for patients
gical margins, a Gleason score of 8 or higher, and
who have failed EBRT include salvage prostatec-
seminal vesicle (SV) invasion [3] are predictors of
tomy, brachytherapy, cryosurgery, and hormonal
biochemical and clinical failures following either
manipulation [6,9,10]. This article presents a gener-
radical prostatectomy or radiation therapy [4].
al review of secondary therapy, both local andsystemic, with a synopsis of the current data. Figure1 shows the suggested clinical flow for patientsrelapsing after primary therapy for localized
* Corresponding author. University of Chicago
Cancer Research Center, 5841 South Maryland Avenue,
E-mail address: [email protected]
0094-0143/03/$ - see front matter Ó 2003, Elsevier Science (USA). All rights reserved. doi:10.1016/S0094-0143(02)00192-1
N.B. Davis et al / Urol Clin N Am 30 (2003) 403–414
N.B. Davis et al / Urol Clin N Am 30 (2003) 403–414
nature of a recurrence as well as in defining thetumor bed target for radiotherapy.
The decision to undertake a prostatectomy is
The role of hormones in addition to or in-
based primarily on patient age, stage of disease,
dependent of adjuvant radiotherapy is discussed
pretreatment PSA, and Gleason score. Although
the pathologist can provide accurate informationabout the status of margins, extracapsular exten-sion (ECE), SV invasion, and perineural or lymph-
ovascular invasion, there is not yet a well-developed
consensus on the criteria for offering immediateadjuvant radiotherapy [11]. Focal margin positivity
External beam radiotherapy requires periodic
or ECE are not, generally speaking, strong enough
follow up by digital rectal examination (DRE)
to warrant immediate radiotherapy, but diffuse
and PSA. Biochemical failure usually predates
margin positivity, SV invasion, or ECE generally are.
clinical failure, especially in the T1c patient pop-
ulation. Because a PSA bounce phenomenon can
nadir that is undetectable as opposed to a nadir
be inherent in any treatment modality that does
that remains detectable postoperatively. An un-
not completely remove the prostate, well-devel-
detectable postoperative nadir, with a subsequent
oped criteria by the ASTRO consensus panel
rise to a detectable value, is more strongly in-
[21,22] recommend that biochemical failure be
dicative of a local-only recurrence amenable to
declared only after three successive rises from the
salvage by local radiotherapy. A PSA concen-
nadir. The consensus panel warns that declaration
tration that is persistently detectable after prosta-
of biochemical failure serves primarily as an
tectomy, unless the source is apparently grossly
endpoint for clinical trials and not necessarily
positive margins, speaks strongly for undetectable
for clinical intervention. Furthermore, a different
metastases, and cure for such patients is unlikely
ASTRO consensus panel [18] did not recommend
with treatment directed at only the pelvis. In
routine prostate bed biopsy for rising PSA after
addition to post-prostatectomy PSA value and
velocity [12], grade (GS ‡ 7), SV involvement, and
Nonetheless, the clinician must often decide,
PSA recurrence within 2 years of prostatectomy
based on the parameters previously discussed,
[13] have been found to be prognostic for reduced
whether to use local therapy after biochemical
efficacy of local-only salvage therapy.
or clinical failure [23–25]. The local treatment op-
Although retrospective reviews of the role of
tions after EBRT are prostatectomy, cryotherapy,
immediate or delayed adjuvant therapy report
freedom from failure rates at 3 years of 20% to
Prostatectomy can be technically challenging as
65% [14–17], results of post-prostatectomy radio-
first-line therapy but becomes more so after pre-
therapy treatment have not yet been reported
vious radiotherapy. The fibrosis in the prostate and
in the randomized setting. Ongoing European
periprostatic tissue frequently results in inconti-
Organization for Research and Treatment of
nence following salvage prostatectomy. This qual-
Cancer (EORTC), National Cancer Institute
ity-of-life issue, taken in context with the increased
age of the patients, means that only a few patients
(CALGB) studies are still examining this impor-
failing EBRT opt for salvage prostatectomy.
tant clinical question. If adjuvant EBRT is given,
Nonetheless, the CALGB has an ongoing salvage
a consensus statement by the American Society of
prostatectomy trial, and the final analysis of this
Therapeutic Radiology and Oncology (ASTRO)
trial should cast more light on the morbidity and
[18] recommends a dose of 64 Gy or slightly
outcome of post-EBRT salvage prostatectomy. In
higher to the prostate bed. This dose level is
the meantime, smaller studies [26–32] have reported
considered tumoricidal and yet tolerable to tissue
techniques that are encouraging with regard to im-
surrounding the prostate bed. ProstaScintÒ (Cy-
proving outcome (long-term disease-free survival
togen Corp, Princeton, NJ) [19,20] a nuclear
rates of 30%–40%) while minimizing morbidity.
medicine scan using technetium-labeled anti-
Similar to prostatectomy, salvage brachyther-
PSMA directed at the intracellular portion of
apy poses morbidity concerns. Although many
the PSMA protein, which has increased yield
providers decline this form of salvage therapy
when the PSA concentration is greater than 0.25
because of morbidity concerns, the dose that can
ng/dL, may assist in determining the local-only
be given by brachytherapy is by its nature more
N.B. Davis et al / Urol Clin N Am 30 (2003) 403–414
focused within the prostate. Small, single-institu-
radical prostatectomy [40,41]. Increasing use of
tion studies [33,34] have reported biochemical
salvage brachytherapy is being reported [42].
control rates ranging from 25% to 70% at 5 years
Androgen ablation, however, is effective in treat-
ing both local and distant relapse but is gener-
Cryotherapy salvage after EBRT failure has
ally viewed as palliative, whereas postoperative
been reported [35–38]. Although the likelihood of
radiation therapy has potential to eradicate local
success with EBRT salvage for initial cryotherapy
disease [24,40,41]. Androgen deprivation may
failure is high, the reported biochemical control
be achieved by bilateral orchiectomy, estrogen
rates with cryotherapy after EBRT failure are
therapy, luteinizing hormone-releasing hormone
somewhat lower (20%–50% at 2 years), with
(LHRH) analogue therapy, antiandrogen therapy,
acceptable morbidity in the reported series.
and combined androgen blockade (CAB).
Immediate versus delayed hormonal therapy
Brachytherapy has undergone a revolution in
technique and has been shown to have biochemical
Both the timing and form of androgen ablation
control results for early-stage disease that are
are controversial, with no evidence that early
roughly equivalent with prostatectomy and EBRT.
hormonal intervention improves survival in PSA-
Because of the more extensive experience with LDR
only relapse [13,42], although in node-positive
brachytherapy over HDR brachytherapy, both as
patients early hormone therapy does improve
initial therapy and as salvage, this discussion is
survival [43]. The only absolute indication for
treatment of patients with recurrence following
The indications for immediate adjuvant local
primary curative therapy is symptomatic metas-
therapy for brachytherapy failure are limited to
tatic disease [41]. Relative indications for early
those unusual situations when the quality of the
hormone therapy include radiographic evidence of
implant, using well-established dosimetric end-
disease progression, a rapid PSADT, and patient
points, is inferior enough to warrant immediate
preference. Early studies (Veterans Administration
EBRT. The much more common situation with
Cooperative Urological Research Group (VA-
brachytherapy, as with EBRT, is delayed bio-
CURG 1 and 2)) suggested that delaying hormonal
chemical or clinical failure. Although the ASTRO
therapy did not adversely effect survival [44], al-
consensus panel definition of biochemical failure
was designed primarily for determining PSA failure
advantage to early therapy for metastatic disease
after EBRT, it has been applied with some success
[43,45,46]. Additionally, in a patterns-of-care study
to brachytherapy failure. Because of morbidity
of patients with a PSADT of less than 12 months
concerns by providers about adding a course of
following EBRT failure, early hormonal manipu-
curative EBRT or cryotherapy to a prostate already
lation was associated with a significant increase in
treated with brachytherapy, the primary local
freedom from disease progression at 5 years when
salvage option after brachytherapy local failure
compared with observation; no such difference was
has been declared is radical prostatectomy.
seen in patients with a PSADT greater than 12
Even the prostatectomy literature in this
months [6]. In general, men with localized disease
regard is scant. Results for salvage prostatectomy
who fail after radical prostatectomy will have
after initial LDR brachytherapy organ-confined
a median time to progression of 8 years after
recurrence have been demonstrated to be poor
biochemical relapse before development of meta-
static disease [5] and a median survival time of 12 to13 years [40]. Application of androgen deprivationtherapy at the time of PSA progression will prolong
Systemic therapy for either prostatectomy or
time to disease progression but also will expose
patients to adverse effects for excessive timeperiods. Deferred endocrine manipulation remains
a reasonable option for elderly, asymptomatic men
Androgen deprivation is used as frequently as
with localized disease as well as for those who
radiation therapy after failure of primary radical
cannot tolerate prolonged hormonal therapy [47];
prostatectomy; in contrast, 90% of patients failing
however, these and other patients who choose to
EBRT will undergo hormonal treatment, with
defer treatment should be prepared to undergo
small numbers of patients undergoing salvage
N.B. Davis et al / Urol Clin N Am 30 (2003) 403–414
does not incur a risk of cardiovascular toxicity[50]. For these reasons, LHRH agonists are a
Estrogens provide negative feedback to the
preferred form of therapy for most patients and
hypothalamus and decrease the release of LHRH,
thereby suppressing anterior pituitary gland release
Impotence and hot flashes are similar to those
of luteinizing hormone (LH). Because testicular
seen with estrogen therapy. The latter may be
Leydig’s cells rely on LH stimulation to produce
particularly troublesome, and although no med-
testosterone, suppression of LH results in cessation
ical therapy has consistently prevented or allevi-
of testicular testosterone production. In addition,
ated the problem, megestrol acetate, cyproterone
estrogen may have a direct effect on prostate cancer
acetate, clonidine, the antidepressant venlafexine
cells [48]. Achieving castration levels of testoster-
(EffexorÒ, Wyeth, Madison, NJ), and a belladon-
one may take 1 to 2 weeks following initiation of
na-phenobarbitol-ergotamine preparation (Beller-
galÒ, Novartis Pharmaceuticals, East Hanover,
The optimal dosage of estrogen therapy has not
NJ) have all been used with varying success and
been established. Oral diethylstilbestrol (DES) at
may be tried for the patient with unacceptable
3 mg/day results in castration levels of serum
testosterone, whereas doses of 1 mg/day inconsis-
Initial randomized trials of LHRH agonist
tently lower serum testosterone and doses less than
compared 1 mg subcutaneous leuprolide (Lu-
1 mg/day are not effective [49]. Higher doses of
pronÒ, Tap Pharmaceuticals, St. Louis, MO)
DES, such as the 5 mg/day used in the oft-cited
with 3 mg/day oral DES, revealing no statistically
Veterans Administration (VA) trials, were associ-
significant difference in efficacy but excess cardio-
ated with an increased incidence of fatal cardio-
vascular toxicity with DES [51]. Subsequently,
vascular events [48]. Serious side effects of estrogen
a series of trials compared goserelin acetate
therapy include myocardial infarction, cerebrovas-
(ZoladexÒ, Astra-Zeneca, Wilmigton, DE) with
cular accident, and pulmonary embolus. Other side
orchiectomy in patients with advanced prostate
effects are attributable to loss of testosterone and
cancer and found no difference in efficacy. Leu-
include loss of libido, impotence, lethargy, gyneco-
prolide availability in depot formulation enabled
mastia, and nipple tenderness. Conjugated estro-
maintenance of castration levels of testosterone
gens, ethinyl estradiol, and medroxyprogesterone
for up to 5 weeks with a single injection and
acetate have been used unsuccessfully in an effort
prompted the US Food and Drug Administration
to decrease side effects. Estrogen use has dimin-
(FDA) approval of this formulation for adminis-
ished in prostate cancer patients because of the high
tration every 4 weeks in 1989. The FDA granted
incidence of cardiovascular complications as well
approval for depot goserelin acetate in 1991.
as the availability of more convenient therapies.
Leuprolide and goserelin acetate are equallyeffective in suppressing LH and FSH productionand are available in various strengths for admin-
Luteinizing hormone-releasing hormone agonists
istration every 1 to 4 months, increasing conve-
nience and patient compliance. Three other
more potent and act by abolishing the pulsatile
LHRH analogues exist: buserelin (SuprefactÒ,
effects of endogenous LHRH. After an initial,
Arentis, Portugal), used extensively in Europe,
transient release of LH and follicle-stimulating
nafarelin acetate (SynarelÒ, Searle, Chicago, IL),
hormone (FSH), both number and function of
approved in the United States for gynecologic use
LHRH receptors on pituitary gonadotropin cells
and seldom used for prostate cancer and triptor-
decline rapidly. Ultimately, minimal to no LH
elin pamoate (TrelstarÒ, Pharmacia Oncology,
and FSH release occurs, and there is a conse-
Kalamazoo, MI), recently FDA approved for
quent rapid decrease of testicular testosterone
advanced prostate cancer as either a 1 month
production [48]. The initial stimulation of LH and
(3.75 mg) or 3 month (11.25 mg) injectable
FSH release causes a surge in testosterone pro-
duction and may transiently worsen pre-existing
Investigations of new delivery methods for
bone pain or urethral obstruction. This effect
LHRH agonists are ongoing. The ViadurÒ system
lasts approximately 1 week before the decline of
(Bayer Corp, West Haven, CT) is a subcutaneous
LHRH receptors, and symptoms should be man-
osmotic pump that delivers leuprolide minidoses
aged expectantly. The use of LHRH agonists com-
for up to 1 year. Implantation of the titanium
pares favorably with orchiectomy but, unlike DES,
cylinder is performed with a short trocar in the
N.B. Davis et al / Urol Clin N Am 30 (2003) 403–414
upper arm between the biceps and triceps; re-
seen with estrogen use and also include a low
moval and replacement are likewise easy pro-
incidence of stimulation of the cancer [53].
cedures. Other designs (eg, AbarelixÒ, Praecis
Therefore, these agents are uncommonly used.
Pharmaceuticals, Waltham, MA.) include novel
Megestrol acetate is primarily used as an anti-
amino acid substitutions in the LHRH deca-
cachectic agent in the setting of cancer, and CPA
peptide that immediately suppress androgen pro-
is used in Europe as part of maximal or CAB.
duction, thus bypassing the initial surge of
Neither agent used alone completely suppresses
testosterone seen with traditional LHRH agonists.
testosterone production; additionally, tachyphy-laxis may develop, with testosterone levels return-
Bilateral orchiectomy removes approximately
90% of circulating testosterone, decreases serum
Nonsteroidal antiandrogens are used in CAB
PSA concentration, and improves symptomatic
but may also be effective as monotherapy. Three
bone pain. The low cost, simplicity, lack of
agents, flutamide (EulexinÒ, Schering-Plough,
compliance issues, and immediate decrease in cir-
culating testosterone make orchiectomy a prac-
Aventis Pharmaceuticals, Bridgewater, NJ) and
tical alternative. Although generally safe and
bicalutamide (CasodexÒ, Astra-Zeneca, Wilming-
performed on an outpatient basis under local anes-
ton, DE), are currently available. Although
thesia with low morbidity, surgery still poses a
flutamide has a relatively short half-life necessi-
small risk of hemorrhage and infection. Subcapsu-
tating frequent oral dosing, both nilutamide and
lar orchiectomy, in which the tunica albuguinea
bicalutamide are given once daily. Because there is
and epididymis of each testis are left intact, has
no decrease in LH production, testosterone levels
been criticized for possibly leaving functional
may be normal or slightly increased, and potency
testicular tissue intact as well. Postoperative
may be spared. The most common side effects are
hormonal assays, however, show this risk to be
diarrhea, nausea, and vomiting. Rare adverse
negligible [48]. The only major drawback to
events include hepatotoxicity with flutamide,
orchiectomy is the psychologic trauma of removal
pulmonary fibrosis with bicalutamide, and de-
of the testes; a subset of men will not consider
creased adaptation to darkness with nilutamide.
orchiectomy, and for these patients medical cas-
Some non–cross-resistance exists between first-,
second-, and third-generation antiandrogens de-
spite a similar mechanism of action. Scher et al [52]used bicalutamide to treat 51 patients with tumor
Antiandrogens bind to androgen receptors in
progression after primary androgen ablation and
the cytoplasm of target cells and prevent activa-
found a response rate of 24%, with 38% of re-
tion of many androgen responsive genes. Alter-
sponders having previously been treated with flut-
natively, anti-androgens may stimulate activation
amide. Another study evaluated 31 patients treated
of androgen-withdrawal genes. Classically inhib-
with bicalutamide; the response rate of 23% in-
iting binding of dihydrotestosterone (DHT) and
cluded 6 men previously treated with flutamide [54].
testosterone, antiandrogens may be used as mono-
Similar responses to nilutamide following fluta-
therapy [52] but primarily are used in combina-
mide and bicalutamide therapy are reported, al-
tion with an LHRH agonist for maximal androgen
though no reports exist of responses to flutamide
blockade. There are two types of anti-androgens:
following bicalutamide or nilutamide therapy.
steroidal, which mimic the progesterone molecule,and nonsteroidal.
Because the mechanism of antiandrogens is to
Steroidal antiandrogens include cyproterone
inhibit binding of testosterone and DHT to both
acetate (CPA) and megestrol acetate (MegaceÒ,
peripheral and central androgen receptors, mono-
Bristal-Myers Squibb, Princeton, NJ). Both block
therapy should be as effective as castration,
androgen binding to receptors in target tissues,
although there remains a risk of overcoming this
possess progestational activity, which indepen-
inhibition by testosterone, which may be present
dently decreases LH production, and have low
in supranormal levels [41]. Evidence exists for
levels of androgenic activity. Side effects, includ-
decreases in PSA concentration and objective
ing cardiovascular morbidity, are similar to those
responses for both flutamide and bicalutamide
N.B. Davis et al / Urol Clin N Am 30 (2003) 403–414
monotherapy in both androgen-dependent and
androgen-independent advanced prostate cancer
[52], although the latter has been more extensively
androgen is derived from the adrenal gland, and
studied. Most studies show bicalutamide to be
a higher proportion of androgen within prostate
inferior to either medical or surgical castration [41]
cancer cells may be of adrenal origin. The two
but document a significant quality-of-life advan-
most commonly used nonclassic antiandrogens
tage to bicalutamide monotherapy in terms of
are ketoconazole (NizoralÒ, Janssen Pharmaceu-
sexual interest and overall physical capacity [55].
conjunction with corticosteroid replacement doses
Staten, NJ) is a 5-alpha reductase inhibitor that
to block adrenal androgen production. Ketoco-
blocks conversion of testosterone to DHT.
nazole is an antifungal that interferes with
Commonly used for benign prostatic hypertro-
cytochrome (CYP) 3A4 and inhibits steroidogen-
phy, there is interest in finasteride use for
esis in both the testes and adrenal glands, resulting
prevention of prostate cancer. The results of an
in castration-range androgen levels within 24
ongoing 7-year, double-blind, intergroup trial of
hours. Most studies of ketoconazole report PSA
finasteride versus placebo for the prevention of
prostate cancer are eagerly awaited. There is also
patients. The precise dose necessary to induce
some evidence of activity in metastatic prostate
a PSA decline is unclear, but most studies use
cancer. A small, double-blind, placebo-controlled
a dose of 400 mg three times/day. Long-term
trial in men with hormone-sensitive prostate can-
patient compliance is poor because of cost,
cer found a distinct delay in time to PSA progres-
difficulty of administration, and the side-effect
sion with finasteride, although not approaching
profile which includes nausea and vomiting, pru-
that seen with castration in other studies [41].
ritus, nail dystrophy, impotence in some cases,
Additionally, androgen ablation was still effective
and adrenal crisis, which can be averted by
after treatment with finasteride in this popula-
concomitant administration of hydrocortisone.
tion. No phase III data support the use of fina-
Aminoglutethimide blocks adrenocorticoid syn-
steride as initial monotherapy; however, use in
thesis by inhibiting conversion of cholesterol to
combination with an antiandrogen (flutamide)
pregnenolone, a precursor to both cortisol and
may be a potency-sparing alternative to tradi-
aldosterone. Studies have primarily been in the
tional therapy in patients with metastatic disease
hormone-refractory metastatic population. Both
agents are typically reserved for second-linehormonal therapy after LHRH agonist or CABfailure.
responses in patients with tumor progression
Hydrocortisone, prednisone, and dexametha-
while undergoing treatment with primary andro-
sone have documented activity in prostate cancer
gen ablation. Reasons for these responses are
and can be used as a third-line hormonal therapy.
multifactorial and include further reduction in
Studies of hormone-refractory prostate cancer
testosterone production, blockade of the residual
patients given steroids versus steroids plus che-
serum androgens through binding of the androgen
motherapy (mitoxantrone) demonstrated response
receptors, reduction in adrenal androgen pro-
rates of 22% in patients in the steroid-only arm.
duction, and binding to other nuclear receptors,
Once a patient fails an LHRH agonist, anti-
such as the alpha or beta estrogen receptor, in the
androgen and antiandrogen withdrawal, and
prostate cancer cells. It is also clear that testos-
second-line therapy with ketoconazole, reason-
terone can still stimulate prostate cancer cell
able options include chemotherapy, participation
growth, even in most hormone-resistant cases.
in a clinical trial. or palliative care. Treatment
For this reason, continued testosterone depletion
considerations should include the patient’s per-
is recommended in all clinical trials of secondary
N.B. Davis et al / Urol Clin N Am 30 (2003) 403–414
level [65]. Phase II studies have found this therapyto be well tolerated and to improve quality of life
[44,64]. Patients can be maintained off androgen
androgen in combination with either an LHRH
deprivation therapy for prolonged periods of time
agonist or orchiectomy to eliminate testicular and
without disadvantages in either time to progression
adrenal androgen production simultaneously and
or survival [63,65]. This approach is still undergo-
completely and was shown in animal models to
ing phase II testing and should be considered
enhance antitumor effects [58]. Although a more
investigational until survival data are mature.
rapid and pronounced response may be seen withcombination therapy, this response may not trans-
late into an advantage in either survival or time toprogression [40]. Numerous randomized studies
have been conducted to evaluate the effects of CAB
antiandrogen therapy while maintaining testoster-
and have used various primary androgen depriva-
one suppression may be associated with a bio-
tion techniques with various forms of antiandrogen
chemical response in up to 20% of patients [66] and,
therapy, with conflicting results. Comparisons of
in some cases, with symptomatic and objective
castration plus cyproterone, DES [59], or flutamide
responses. The mechanism for this response is
[58] versus castration alone have failed to show
unknown. Mutated androgen receptors, seen al-
a benefit of CAB in terms of overall or progression-
most exclusively in tumors treated with CAB and
free survival. The most recent meta-analysis
stimulated by binding of antiandrogens, have been
suggested a statistically significant survival advan-
ruled out as a general explanation for this pheno-
tage in using CAB with the non-steroidal agents
menon [67]. Because antiandrogen withdrawal is
(flutamide and nilutamide). In contrast, the use of
required for enrollment in clinical trials, and this
a steroidal agent (cyproterone acetate) was associ-
potential benefit exists, it is reasonable to initiate
ated with a decreased survival. Conflicting studies,
withdrawal for patients with progressive disease
evaluating LHRH agonist therapy with or without
receiving antiandrogen therapy. Withdrawal re-
antiandrogen therapy [60], LHRH agonist plus
sponses occur in approximately 10% to 30% of
antiandrogen therapy versus castration alone [61],
patients [44], and the likelihood of response may
and castration with or without nilutamide [62],
correlate with duration of exposure to the anti-
showed a benefit to CAB. Additionally, compari-
androgen. Responses will generally be observed
son of LHRH agonist plus flutamide versus
within a few weeks after withdrawal, although
bicalutamide revealed a benefit in time to pro-
responses to bicalutamide withdrawal may occur
gression for LHRH agonist plus bicalutamide [25].
later, possibly because of the longer half-life. The
Currently, CAB should be considered for palliation
duration of response is typically 3 to 4 months but
in symptomatic, advanced prostate cancer.
does not usually last more than 6 months.
The concept of intermittent hormonal therapy is
based on the hypothesis that prolonged androgendeprivation therapy may stimulate progression
Salvage surgery, cryotherapy, and hormonal
from androgen-dependent to androgen-indepen-
deprivation are options for the patients who have
dent prostate cancer [63,64] Periodic reintroduc-
failed primary radiation therapy for prostate
tion of endogenous androgen after androgen
cancer. Although salvage surgery has been shown
withdrawal may result in generation of differenti-
to lead to long-term disease-free survival [68],
ated tumor cells and therefore may delay emergence
associated morbidity (eg, incontinence) and high
of the androgen-independent phenotype [44,64].
recurrence rates have prevented wide acceptance.
Preclinical evidence exists in some cell lines
Use of androgen deprivation as neoadjuvant
(LNCaP, Shionogi), but not in others (Dunning)
therapy with salvage surgery for clinically localized
[65]. Clinically, intermittent hormonal therapy
recurrent prostate cancer has been studied by
consists of androgen deprivation continued for
Garzotto et al [68] in 29 men with locally recurrent
some time following adequate testosterone sup-
prostate cancer following primary radiation ther-
pression. Following discontinuation of hormone
apy. They used either surgical or medical castration
therapy, resumption is determined by PSA progres-
for 3 months preoperatively, followed by salvage
sion, usually caused by a recovering testosterone
surgery, and continued androgen deprivation post-
N.B. Davis et al / Urol Clin N Am 30 (2003) 403–414
operatively indefinitely in patients with T3 or T4 or
overall survival, disease-specific survival, or free-
node-positive disease. For those responding to
dom from local relapse were evident. The addition
androgen ablation preoperatively, there was a de-
of androgen deprivation to EBRT has been shown
creased incidence of surgical margin involvement,
to improve both disease-free and overall survival
correlating with improved disease-free (79%) and
rates for men with locally advanced prostate can-
disease-specific (92%) survival at 5.7 years. The
cer. The optimal timing and duration of hormone
5 patients who did not respond to preoperative
manipulation is still undefined, and whether
androgen ablative therapy had a low disease-
early hormonal therapy as a single method is as
specific survival rate (20%), a higher rate of positive
effective as radical prostatectomy, radiation ther-
surgical margins, and perhaps should not be
apy, or combined-modality therapy for locally ad-
considered candidates for salvage surgery [68].
vanced prostate cancer remains to be answered [4].
The effect of EBRT on locally recurrent disease
Eventually, prostate cancer becomes hormone
following radical prostatectomy has been con-
refractory, and the treatments discussed previously
firmed in several studies, and generally 30% to
will cease to be of use. Median survival time
60% of patients will revert to an undetectable
following development of hormone-resistant pros-
PSA concentration following salvage radiation
tate cancer is 12 to 15 months. Survival is likely to
therapy [42]. Responses correlate to preoperative
be longer in those with biochemical failure only
PSA concentration, pathologic features of the
[69]. Primary androgen deprivation with an LHRH
primary tumor, the absolute PSA concentration at
agonist should continue for the life of the patient to
the time of salvage radiation (PSA < 1.0 being
prevent testosterone production with a concomi-
best), and the timing of PSA recurrence, with men
tant worsening of disease symptoms. If the patient
whose PSA concentration increased more than 1
maintains a good performance status following
year following surgery maintaining undetectable
antiandrogen withdrawal and any second- or third-
levels more often than those whose PSA concen-
line hormonal therapies, treatment with either
tration increased earlier. Studies evaluating radi-
standard chemotherapy or on a clinical trial is
ation therapy versus combined radiation plus
reasonable. For patients with poor performance
hormone manipulation for locally advanced
status and for elderly patients who are asymptom-
prostate cancer are difficult to interpret; adding
atic, palliative care is reasonable.
hormones may enhance radiation-induced apo-
ptosis, prolonging suppression of tumor growth,
agents have been studied both as single agents
or may have a direct effect on tumor cells in
and in combination, appreciable rates of objective
patients in whom radiation failed [50,42]. Early
radiologic and PSA responses are 20% to 50%.
studies found a benefit in disease-free survival, but
Additionally, despite observations that chemo-
not in overall survival, with radiation plus either
therapy improves quality of life in men with
orchiectomy or DES when compared with radia-
hormone-resistant prostate cancer [70–72], no
tion alone [44,45], although the lack of benefit in
agent or regimen has yet demonstrated a survival
overall survival with DES was probably caused by
advantage in randomized clinical trials.
A study in 1998 by Eulau et al [50] evaluated 105
men treated with radiation therapy for locally
advanced prostate cancer following radical prosta-tectomy. Twenty-nine evaluable patients under-
There is compelling evidence that early hor-
went androgen deprivation therapy (median 6
monal therapy prolongs life in many stages of
months, range 2–10 months) combined with ra-
prostate cancer. Large-scale trials to answer this
diation therapy. Although there were 4 local
question have not yet been conducted in surgically
recurrences following therapy, none were seen in
treated patients or in patients with PSA-only
the men given hormone therapy. Both freedom
relapse. Thus, many physicians and patients use
from clinically evident distant relapse (p=0.014)
early hormone therapy in PSA-only relapse. Many
and freedom from biochemical relapse (p=0.004)
unique new agents are being tested in this pop-
were significantly superior in patients treated with
ulation and may offer benefits. Patients and
combination therapy, although no differences in
physicians are encouraged to participate in such
N.B. Davis et al / Urol Clin N Am 30 (2003) 403–414
trials, with hormone therapy reserved for sub-
[13] Ornstein DK, Oh J, Herschman JD, et al. Evalu-
ation and management of the man who has failed
Following failure of primary hormone therapy,
primary curative therapy for prostate cancer. Urol
a standard algorithm of care exists: antiandrogen
[14] Morris MM, Dallow KC, Zietman AL, et al.
withdrawal, use of alternative or first-line anti-
Adjuvant and salvage irradiation following radical
androgens, ketoconazole, and chemotherapy. At
prostatectomy for prostate cancer. Int J Radiat
each interval, clinical trials should be offered since
none of these maneuvers are proven to prolong life.
[15] Schild SE, Buskirk SJ, Wong WW, et al. The use of
radiotherapy for patients with isolated elevation of
serum prostate specific antigen following radicalprostatectomy. J Urol 1996;156:1725.
[1] Catalona WJ, Ramos CG, Carvalhal GF. Contem-
[16] Schild SE, Wong WW, Grado GL, et al. Radio-
porary results of anatomic radical prostatectomy.
therapy for isolated increases in serum prostate-
specific antigen levels after radical prostatectomy.
[2] Zincke H, Oesterling JE, Blute ML, et al. Long-
term (15 years) results after radical prostatectomy
[17] Anscher MS. Adjuvant radiotherapy following
for clinically localized (Stage T22c or lower) pros-
radical prostatectomy is more effective and less
toxic than salvage radiotherapy for a rising prostate
[3] Walsh PC, Partin AW, Epstein JI. Cancer control
specific antigen. Int J Cancer 2001;96:91.
and quality of life following anatomical radical
[18] Cox JD, Gallagher MJ, Hammond EH, et al. Con-
retropubic prostatectomy: results at 10 years. J Urol
sensus statements on radiation therapy of prostate
cancer: guidelines for prostate re-biopsy after radiation
[4] Smith MR, Garnick MB. Primary hormonal therapy
and for radiation therapy with rising prostate-specific
for locally advanced prostate cancer. In: Vogelzang
antigen levels after radical prostatectomy. American
NJ, Scardino PT, Shipley WU, et al, editors.
Society for Therapeutic Radiology and Oncology
Comprehensive textbook of genitourinary oncology.
Consensus Panel. J Clin Oncol 1999;17:1155.
2nd edition. Philadelphia: Lippincott Williams &
[19] Elgamal AA, Troychak MJ, Murphy GP. Pros-
taScint scan may enhance identification of prostate
[5] Pound CR, Partin AW, Eisenberger MA, et al.
cancer recurrences after prostatectomy, radiation,
Natural history of progression after PSA elevation
or hormone therapy: analysis of 136 scans of 100
following radical prostatectomy. JAMA 1999;
[20] Fang DX, Stock RG, Stone NN, et al. Use of
[6] Sylvester J, Grimm P, Blasko J, et al. The role of
radioimmunoscintigraphy with indium-111-labeled
androgen ablation in patients with biochemical or
CYT-356 (ProstaScint) scan for evaluation of
local failure after definitive radiation therapy: a
patients for salvage brachytherapy. Tech Urol 2000;
survey of practice patterns of urologists and ra-
diation oncologists in the United States. Urology
[21] American Society of Therapeutic Radiology and
Oncology (ASTRO) Consensus Panel. Consensus
[7] Zlotta AR, Schulman CC. Neoadjuvant and adju-
statement: guidelines for PSA following radiation
vant hormone therapy for prostate cancer. World
therapy. Int J Radiat Oncol Biol Phys 1997;37:1035.
[22] Taylor JM, Griffith KA, Sandler HM. Definitions
[8] van den Ouden D, Hop WC, Schroder FH. Pro-
of biochemical failure in prostate cancer following
gression in and survival of patients with locally
radiation therapy. Int J Radiat Oncol Biol Phys
advanced prostate cancer (T3) treated with radical
prostatectomy as monotherapy. J Urol 1998;160:1392.
[23] Parker CC, Dearnaley DP. The management of
[9] Grossfeld GD, Steir DM, Flanders SC, et al. Use
PSA failure after radical radiotherapy for localized
of second treatment following definitive local ther-
prostate cancer. Radiother Oncol 1998;49:103.
apy for prostate cancer: data from the CAPSURE
[24] Corral DA, Pisters LL, von Eschenbach AC.
Treatment options for localized recurrence of pros-
[10] Moul JW. Rising PSA after local therapy failure:
tate cancer following radiation therapy. Urol Clin
immediate vs. deferred treatment. Oncology (Hun-
[25] Schellhammer PF, Kuban DA, el-Mahdi AM.
[11] Parker C, Warde P, Catton C. Salvage radiother-
Treatment of clinical local failure after radiation
apy for PSA failure after radical prostatectomy.
therapy for prostate carcinoma. J Urol 1993;150:
[12] Egawa S, Ohori M, Iwamura M, et al. Efficacy and
[26] Vaidya A, Soloway MS. Salvage radical prostatec-
limitations of delayed/salvage radiation therapy
tomy for radiorecurrent prostate cancer: morbidity
after radical prostatectomy. BJU Int 1999;84:815.
N.B. Davis et al / Urol Clin N Am 30 (2003) 403–414
[27] Russo P. Salvage radical prostatectomy after radi-
[43] Messing EM, Manola J, Sarosdy M, et al. Immediate
ation therapy and brachytherapy. J Endourol 2000;
hormonal therapy compared with observation after
radical prostatectomy and pelvic lymphadenectomy
[28] Bochner BH, Figueroa AJ, Skinner EC, et al.
in men with node-positive prostate cancer. N Engl
Salvage radical cytoprostatectomy and orthotopic
urinary diversion following radiation failure. J Urol
[44] Kuyu H, Lee WR, Bare R, et al. Recent advances in the
treatment of prostate cancer. Ann Oncol 1999;10:891.
[29] Pontes JE, Montie J, Klein E, et al. Salvage surgery
[45] Bolla M, Gonzalez D, Warde P, et al. Improved
for radiation failure in prostate cancer. Cancer
survival in patients with locally advanced prostate
cancer treated with radiotherapy and goserelin.
[30] Stein A, Smith RB, deKernion JB. Salvage radical
prostatectomy after failure of curative radiother-
[46] The Medical Research Council Prostate Cancer
apy for adenocarcinoma of prostate. Urology 1992;
Working Party Investigators Group. Immediate ver-
sus deferred treatment for advanced prostate cancer:
[31] Zincke H. Radical prostatectomy and exenterative
initial results of the Medical Research Council trial.
procedures for local failure after radiotherapy with
curative intent: comparison of outcomes. J Urol
[47] Roberts SG, Blute ML, Bergstralh EJ, et al. PSA
doubling time as a predictor of clinical progression
[32] Rainwater LM, Zincke H. Radical prostatectomy
after biochemical failure following radical prosta-
after radiation therapy for cancer of the prostate:
tectomy for prostate cancer. Mayo Clin Proc 76:
feasibility and prognosis. J Urol 1988;140:1455.
[33] Grado GL, Collins JM, Kriegshauser JS, et al.
[48] McLeod DG, Vogelzang NJ. Androgen blockade:
Salvage brachytherapy for localized prostate cancer
monotherapy and quality-of-life issues. In: Vogel-
after radiotherapy failure. Urology 1999;53:2.
zang NJ, Scardino PT, Shipley WU, et al, editors.
[34] Beyer DC. Permanent brachytherapy as salvage
Comprehensive textbook of genitourinary oncol-
treatment for recurrent prostate cancer. Urology
ogy. 2nd edition. Philadelphia: Lippincott Williams
[35] Chin JL, Pautler SE, Mouraviev V, et al. Results of
[49] Bishop MC. Experience with low-dose oestrogen in
salvage cryoablation of the prostate after radiation:
the treatment of advanced prostate cancer: a per-
identifying predictors of treatment failure and
complications. J Urol 2001;165:1937.
[50] Eulau SM, Tate DJ, Stamey TA, et al. Effect of
[36] Izawa JI, Perrotte P, Greene GF, et al. Local tumor
combined transient androgen deprivation and irra-
control with salvage cryotherapy for locally re-
diation following radical prostatectomy for prostatic
current prostate cancer after external beam radio-
cancer. Int J Radiat Oncol Biol Phys 1998;41:735.
[51] The Leuprolide Study Group. Leuprolide vs. di-
[37] de la Taille A, Hayek O, Benson MC, et al. Salvage
ethylstilbestrol for metastatic prostate cancer. N
cryotherapy for recurrent prostate cancer after ra-
diation therapy: the Columbia experience. Urology
[52] Scher HI, Liebertz C, Kelly WK, et al. Bicalutamide
for advanced prostate cancer: the natural versus
[38] Pisters LL, Perrotte P, Scott SM, et al. Patient
treated history of disease. J Clin Oncol 1997;15:2928.
selection for salvage cryotherapy for locally recur-
[53] Dawson NA, Conaway M, Halabi S, et al. A
rent prostate cancer after radiation therapy. J Clin
randomized study comparing standard versus mod-
erately high dose megestrol acetate for patients with
[39] Brenner PC, Russo P, Wood DP, et al. Salvage
advanced prostate carcinoma: Cancer and Leuke-
radical prostatectomy in the management of locally
mia Group B Study 9181. Cancer 2000;88:825.
recurrent prostate cancer after 1251 implantation.
[54] Joyce R, Fenton MA, Rode P, et al. High dose bi-
calutamide for androgen independent prostate can-
[40] Schroder FH, van den Ouden D. Management of
cer: effect of prior hormonal therapy. J Urol 1998;
locally advanced prostate cancer. 2. Radiotherapy,
neoadjuvant endocrine treatment, update 1997–
[55] Moul JW. Prostate specific antigen only progression
of prostate cancer. J Urol 2000;163:1632.
[41] Grossfeld GD, Small EJ, Lubeck DP, et al. Androgen
[56] Ornstein DK, Rao GS, Johnson B, et al. Combined
deprivation therapy for patients with clinically
finasteride and flutamide therapy in men with
localized (stages T1 to T3) prostate cancer and for
advanced prostate cancer. Urology 1996;48:901.
patients with biochemical recurrence after radical
[57] Bubley GJ, Carducci M, Dahut W, et al. Eligibility
and response guidelines for phase II clinical trials in
[42] Fichtner J. The management of prostate cancer in
androgen-independent prostate cancer: recommen-
patients with a rising prostate-specific antigen level.
dations from the prostate-specific antigen working
N.B. Davis et al / Urol Clin N Am 30 (2003) 403–414
[58] Eisenberger MA, Blumenstein BA, Crawford ED,
[65] Sciarra A, DiChiro C, DiSilverio F. Intermittent
et al. A comparison of bilateral orchiectomy with
androgen deprivation (IAD) in patients with bio-
or without flutamide in stage D2 prostate cancer.
chemical failure after radical retropubic prostatec-
tomy (RRP) for clinically localized prostate cancer.
[59] Schroder FH. Endocrine treatment of prostate
cancer-recent developments and the future. Part 1:
[66] Gleave ME, Bruchovsky N, Moore MJ, et al.
maximal androgen blockade, early vs. delayed endo-
Clinical basics: prostate cancer: 9. Treatment of
crine treatment and side-effects. BJU Int 1999;
advanced disease. Can Med Assoc J 1999;160:225.
[67] Taplin ME, Bubley GJ, Ko YJ, et al. Selection for
[60] Crawford ED, Eisenberger MA, McLeod DG, et al.
androgen receptor mutations in prostate cancers treated
A controlled trial of leuprolide with and without
with androgen antagonist. Cancer Res 1999;59:2511.
flutamide in prostatic carcinoma. N Engl J Med
[68] Garzotto M, Wajsman Z. Androgen deprivation with
salvage surgery for radiorecurrent prostate cancer:
[61] Denis LJ, Carneiro de Moura JL, Bono A, et al.
results at 5-year followup. J Urol 1998;159:950.
Goserelin acetate and flutamide versus bilateral
[69] Dawson NA, Vogelzang NJ. Prostate cancer. New
orchiectomy: a phase III EORTC trial (30853).
EORTC GU Group and EORTC Data Center.
[70] Kantoff PW, Halabi S, Conaway M, et al. Hydro-
cortisone with or without mitoxantrone in men with
[62] Dijkman GA, Janknegt RA, De Reijke TM, et al.
hormone-refractory prostate cancer: results of the
Long-term efficacy and safety of nilutamide plus
Cancer and Leukemia Group B 9182 study. J Clin
castration in advanced prostate cancer, and the
significance of early prostate specific antigen nor-
[71] Tannock IF, Osoba D, Stockler MR, et al.
Chemotherapy with mitoxantrone plus prednisone
[63] Gleave ME, Bianca SE, Goldenberg SL, et al.
or prednisone alone for symptomatic hormone-
Long-term neoadjuvant hormone therapy prior to
resistant prostate cancer: a Canadian randomized
radical prostatectomy: evaluation of risk for bio-
trial with palliative end points. J Clin Oncol 1996;
chemical recurrence at 5-year follow-up. Urology
[72] Savarese D, Halabi S, Hars V, et al. A phase II study
[64] Grossfeld GD, Chaudhary UB, Reese DM, et al.
of docetaxel, estramustine, and low dose hydrocor-
Intermittent androgen deprivation: update of cycling
tisone in men with hormone refractory prostate
characteristics in patients without clinically apparent
cancer: a final report of CALGB 9780. J Clin Oncol
metastatic prostate cancer. Urology 2001;58:240.
The Fluoride and Infertility Connection Where Do We Go From Here? By Heidi M. Jost RN, CCP IKH, CH Male and female infertility is increasing. The effects of fluoride on female and male fertility are and have been an area of growing concern. Our environment has become a fluoride dumping ground. Fluoride is in our air (It is the number one pollutant.), water, soil, food,
Issue Date (11-28-01) Review Date (05-24-12) MSDS Information provided by London Resin Co LTD, Issued 11-28-01 and reviewed 2010. Section 1: Product and Company Identification Product Name: 18181, 18182 Benzoyl Peroxide Paste (Component of 18181, 18182 Kit) Synonym: None Company Name Ted Pella, Inc., P.O. Box 492477, Redding, CA 96049-2477 Domestic Phone (800) 237-3526 (Mon-T
 Nancy B. Davis, MDa, Ashesh B. Jani, MDb,
aDepartment of Medicine, Section of Hematology/Oncology, The University of Chicago Medical Center,
5841 South Maryland Avenue, MC2115, Chicago, IL 60637, USA
bDepartment of Radiation and Cellular Oncology, The University of Chicago Medical Center,
5841 South Maryland Avenue, MC 9006, Chicago, IL 60637, USA
cThe Ben May Institute for Cancer Research, The University of Chicago Cancer Research Center,
5841 South Maryland Avenue, MC 1140, Chicago, IL 60637, USA
Because of the widespread use of prostate-
Additionally, the PSA doubling time (PSADT)
specific antigen (PSA) for screening, most prostate
at the time of biochemical failure, with a cut-
cancers are now being detected in a localized stage;
off PSADT of less than 10 months, predicts for
therefore, most of the 190,000 men destined to be
the early development of distant metastasis and is
diagnosed with prostate cancer in 2002 are able to
predictive of death from prostate cancer [5,6].
Nancy B. Davis, MDa, Ashesh B. Jani, MDb,
aDepartment of Medicine, Section of Hematology/Oncology, The University of Chicago Medical Center,
5841 South Maryland Avenue, MC2115, Chicago, IL 60637, USA
bDepartment of Radiation and Cellular Oncology, The University of Chicago Medical Center,
5841 South Maryland Avenue, MC 9006, Chicago, IL 60637, USA
cThe Ben May Institute for Cancer Research, The University of Chicago Cancer Research Center,
5841 South Maryland Avenue, MC 1140, Chicago, IL 60637, USA
Because of the widespread use of prostate-
Additionally, the PSA doubling time (PSADT)
specific antigen (PSA) for screening, most prostate
at the time of biochemical failure, with a cut-
cancers are now being detected in a localized stage;
off PSADT of less than 10 months, predicts for
therefore, most of the 190,000 men destined to be
the early development of distant metastasis and is
diagnosed with prostate cancer in 2002 are able to
predictive of death from prostate cancer [5,6].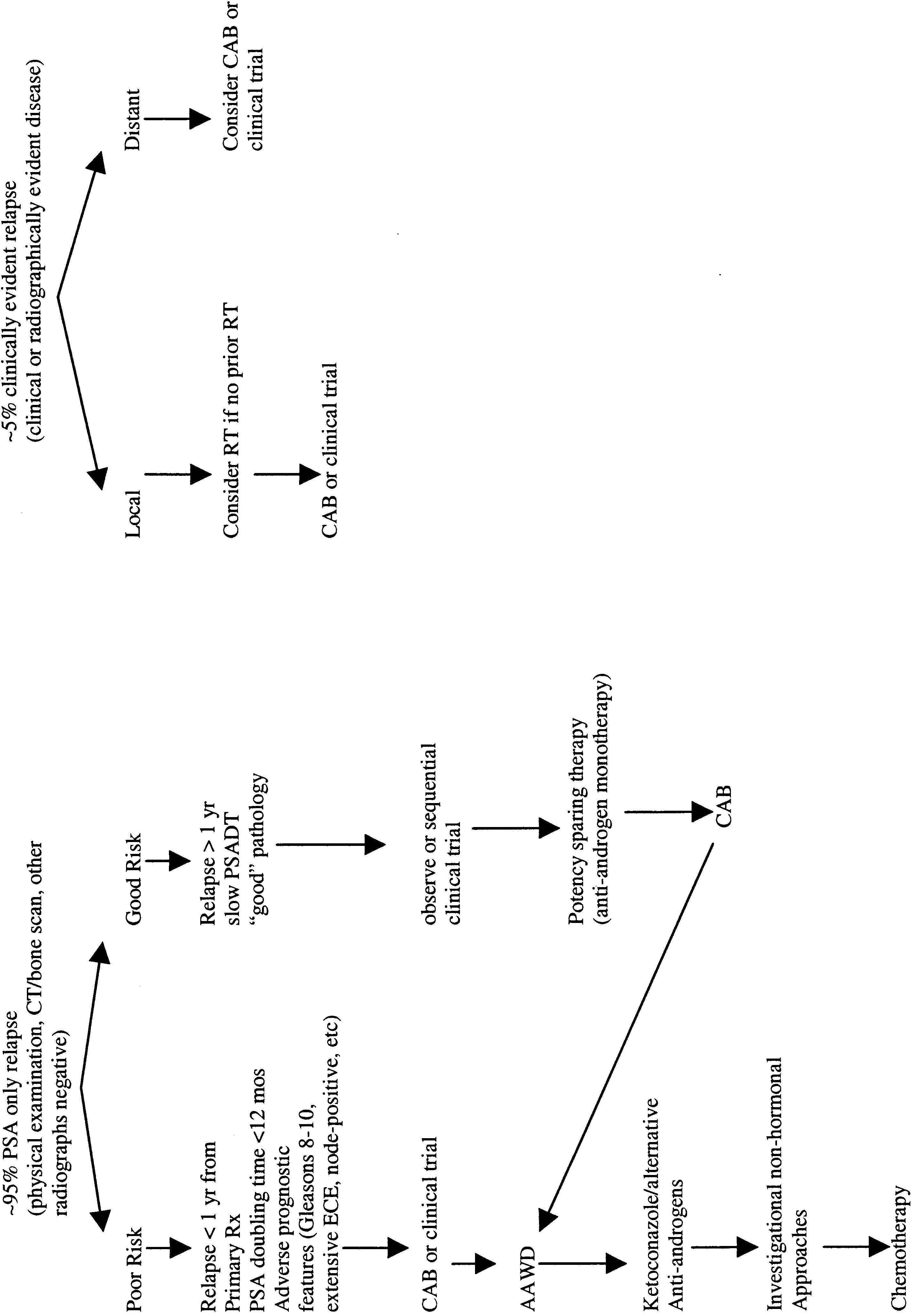 N.B. Davis et al / Urol Clin N Am 30 (2003) 403–414
N.B. Davis et al / Urol Clin N Am 30 (2003) 403–414
nature of a recurrence as well as in defining thetumor bed target for radiotherapy.
N.B. Davis et al / Urol Clin N Am 30 (2003) 403–414
N.B. Davis et al / Urol Clin N Am 30 (2003) 403–414
nature of a recurrence as well as in defining thetumor bed target for radiotherapy.