Depletion of Mitochondrial DNA in Liver Under
Antiretroviral Therapy With Didanosine, Stavudine,
Ulrich A. Walker,1 Jochen B¨auerle,1 Montse Laguno,2 Javier Murillas,2 Stefan Mauss,3 G ¨unther Schmutz,3
Bernhard Setzer,1 Rosa Miquel,2 Jos´e M. Gatell,2 and Josep Mallolas2
The “D drug” HIV reverse-transcriptase inhibitors zalcitabine, didanosine, and stavudine are relatively strong inhibitors of polymerase-gamma compared with the “non–D drugs” zidovudine, lamivudine, and abacavir. D drugs deplete mitochondrial DNA (mtDNA) in cultured hepatocytes. This mtDNA depletion is associated with an increased in vitro pro- duction of lactate. To investigate the origin of hyperlactatemia in HIV-infected patients and the effects of antiretroviral therapy on liver mtDNA, we biopsied liver tissue from 94 individuals with chronic hepatitis C virus (HCV) infection. Eighty subjects were coinfected with HIV. Serum lactate was measured at the time of biopsy. Hepatic mtDNA and liver histology were centrally assessed. Liver mtDNA content of HIV-infected patients receiving D drugs at the time of biopsy (n ؍ 34) was decreased by 47% (P<.0001) compared with those without D drugs (n ؍ 35). Aside from a possible association between HCV genotype I status and mtDNA depletion in multivariate analysis, there were no other virologic, immunologic, histologic, demographic or treatment-related variables that could explain the mtDNA de- pletion. Lactate was above the upper limit of normal in only three patients, all of whom were treated with D drugs. The mtDNA in each of them was lower than in any non–D drug patient and significantly (P ؍ .017) depleted compared with D drug patients with normal lactate. In conclusion, D drug treatment is associated with decreased hepatic mtDNA in HIV-infected patients with chronic HCV infection. Moderate mtDNA depletion in liver does not neces- sarily lead to hyperlactatemia, but more pronounced decreases in hepatic mtDNA may be an important contributor to lactate elevation. (HEPATOLOGY 2004;39:311–317.)
Antiretroviraltherapy(ART)hassignificantlyde- tease inhibitors (PIs) or a nonnucleoside reverse
creased the HIV-associated morbidity and mor-
transcriptase inhibitor (NNRTI), or of three NRTIs.2
tality in industrialized countries.1 ART usually
With prolonged exposure to antiretroviral drugs, clini-
consists of a combination of two nucleoside analogue re-
cians became aware of long-term side effects of individual
verse transcriptase inhibitors (NRTIs) with either pro-
ART components. Many adverse effects of the NRTIclass of anti-HIV drugs are now related to the fact thatNRTIs undergo intracellular triphosphorylation, then in-
Abbreviations: ART, antiretroviral therapy; NRTI, nucleoside analogue reversetranscriptase inhibitor; PI, protease inhibitor; NNRTI, nonnucleoside reverse tran-
hibit the replication of mitochondrial DNA (mtDNA) by
scriptase inhibitor; mtDNA, mitochondrial DNA; ddC, zalcitabine; ddI, di-
interacting with gamma-polymerase.3 In vitro studies
danosine; d4T, stavudine; HCV, hepatitis C virus; nDNA, nuclear DNA; ULN,
point toward differences between the potencies of the
upper limit of normal; ALT, alanine aminotranferase.From 1Medizinische Universita¨tsklinik, Department of Clinical Immunology,
individual NRTIs in depleting mtDNA, with the so-
Freiburg, Germany; 2Hospital Clinı´c, Barcelona, Spain; and the 3Center for HIV
called “D drugs” zalcitabine (ddC), didanosine (ddI), and
and Hepatogastroenterology, Du¨sseldorf, Germany.
stavudine (d4T) being relatively strong inhibitors of poly-
Received August 22, 2003; accepted November 24, 2003. This work was supported by the BMBF, Kompetenznetz HIV/AIDS (grant num-
merase-gamma compared with the other currently li-
censed nucleoside analogues (so-called “non–D drugs”).4,5
Address reprint requests to: Ulrich A. Walker, M.D., Medizinische Universi-
Studies performed in vitro and in animals suggest that
ta¨tsklinik, Department of Clinical Immunology, Hugstetterstr. 55, D-79106Freiburg, Germany. E-mail: [email protected]; fax:
depletion of mtDNA may represent an underlying mech-
anism of NRTI-related hepatic side effects in HIV pa-
Copyright 2004 by the American Association for the Study of Liver Diseases.
tients.5–7 Cell models and animal data, however, have
Published online in Wiley InterScience (www.interscience.wiley.com). DOI 10.1002/hep.20074
limitations in predicting clinical toxicities, partly because
of pharmacokinetic differences between species and partly
controlled diabetes mellitus, end-stage renal disease, or
because of variations in the uptake and phosphorylation
severe respiratory disease. Group 1 was subdivided into
of nucleosides into tissues, cells, and mitochondria. To
three subgroups based on the antiretroviral regimen at the
date, only limited observational mtDNA data of HIV
time of biopsy: patients receiving no antiretroviral ther-
patients receiving ART are available,8,9 and a systematic
apy (subgroup 1A), no D drug at all (subgroup 1B), or at
study has not been conducted. Furthermore, the available
data conflict with regard to zidovudine, because mtDNA
Group 2 subjects had to meet all the entry criteria of
depletion has also been observed despite the fact that this
group 1, except for the fact that they were HIV-negative.
NRTI is not a strong inhibitor of gamma-polymerase at
They were recruited to assess possible unspecific effects of
HIV infection on mtDNA levels in liver.
Slight and asymptomatic elevations of lactate are fre-
Liver Histology. Percutaneous liver biopsies were per-
quently associated with the prolonged use of NRTIs and
formed using a Mengini (16-gauge) needle. The largest
may also be related to mtDNA depletion in tissues.3,10
aliquot of each biopsy cylinder (Ն20 mm) was embedded
Such mild hyperlactatemia has to be distinguished from
in paraffin and centrally assessed by a single pathologist,
lactic acidosis or symptomatic hyperlactatemia, which
who was blinded to the clinical and laboratory informa-
have been reported in association with liver pathology.11
tion. The degrees of liver fibrosis and necroinflammatory
The contribution of liver impairment (particularly of he-
activity were scored on Haematoxilin-Eosin and Masson’s
patic mtDNA depletion) to both forms of lactate eleva-
trichrome stains according to Scheuer’s classification.13
tion is not clear, although results from an exogenous
The percentage of hepatocytes displaying signs of macro-
lactate challenge test have suggested that asymptomatic
or microvesicular steatosis was also scored.
hyperlactatemia may result from a loss of lactate clearance
Quantification of mtDNA. The second aliquot of
(which is likely to involve the liver) and increased lactate
the liver biopsy (4 mm) was immediately frozen and
stored at Ϫ70° C until shipment on dry ice for centralized
Our aim was to investigate if NRTIs and especially D
and blinded mtDNA measurements by quantitative
drugs deplete mtDNA in hepatic tissue of HIV patients
Southern blot analysis as described previously.5,14,15
and if there is a link between mtDNA depletion in liver
mtDNA was probed with a 12.9-kb pair, random-prime
and lactate elevation. Because of ethical difficulties in ob-
digoxigenin-labeled fragment, spanning nucleotide posi-
taining repeat liver biopsies, we chose a cross-sectional
tions 3470 and 16379 of human mtDNA; nuclear DNA
design and selected HIV patients with chronic hepatitis C
(nDNA) was simultaneously detected with a second
virus (HCV) coinfection as the principal study popula-
probe, directed against the multicopy 18S ribosomal
DNA gene. The intensities of the mtDNA and nDNAsignals were densitometrically quantified using Scion-im-
Experimental Procedures
age (Scion Corporation, Frederick, MD), and mtDNAwas normalized for nDNA-content by calculating the
Human Subjects. After ethics committee approval,
mtDNA/nDNA ratio. Two DNA standards extracted
patients were recruited in the Hospital Clinı´c, Barcelona,
from HepG2 hepatoma cells (ATCC HB-8065) and hu-
and the HIV Centre, Du¨sseldorf, from February 2001
man fibroblasts were run in parallel on every blot to assess
until October 2002. Consecutive patients were enrolled if
assay variations. The mtDNA/nDNA measurements
they granted informed consent and met the inclusion and
were reliable with an interrun variation of 20%; large
exclusion criteria for one of the following study groups.
variations in the amount of DNA loaded onto the gel do
Group 1 consisted of HIV-1 patients with chronic
not influence the result.14,15 Southern blot analysis was
HCV coinfection, as confirmed by a positive HCV-anti-
also used to screen for large-scale mtDNA deletions.
body ELISA and positive HCV-RNA measurements
Other Measurements. At the time of liver biopsy, a
(Ͼ500 IU/mL). Patients in this group had to meet further
forearm vein was cannulated. After at least one hour,
inclusion criteria such as no interferon and ribavirin pre-
blood was drawn from rested patients without the use of a
treatment and absence of HbsAg and other liver diseases
tourniquet. Patients were instructed to avoid fist clench-
(e.g., autoimmune hepatitis, primary biliary cirrhosis, al-
ing and hand pumping. Blood was collected in sodium
pha-1 antitrypsin deficiency, hepatocellular carcinoma,
fluoride/potassium oxalate tubes and placed on ice. Lac-
haemochromatosis, and Wilson’s disease). Pregnant or
tate was immediately tested enzymatically in an auto-
lactating females were excluded, as were patients who con-
mated analyzer (Roche/Hitachi 917; Roche, Basel,
sumed intravenous or inhaled drugs, drank alcohol exces-
Switzerland) according to the manufacturer’s instruc-
sively (Ͼ80 g ethanol/d), or suffered from poorly
tions. Both laboratories’ normal reference range was 50 to
220 mg/L. Values were calculated as the upper limit of
those not given D drugs (14.5 vs. 18.1 years P ϭ .04) and
a slightly lower percentage of undetectable HIV-RNA
Further evaluation included quantification of serum
(71% vs. 94%, P ϭ .03). Both antiretrovirally treated
alanine aminotranferase (ALT), HCV, and HIV viral
groups did not differ with respect to NNRTI or current
loads (COBAS AMPLICOR HCV-MONITOR version
PI use; however, patients on D drugs had a longer cumu-
2.0 and COBAS AMPLICOR HIV-MONITOR version
lative exposure to total ART and to PIs than their non–D
1.5, Roche Diagnostics, Basel, Switzerland) and of CD4
lymphocyte counts at the time of biopsy. HCV genotype
The mean age (43.7 Ϯ 10.8 years) and sex (79% male)
of group 2 did not statistically differ from group 1. Statistics. The laboratory results and demographic Liver mtDNA. For easier comparison of the quanti-
and clinical parameters among groups were univariately
tative mtDNA results, the mean mtDNA/nDNA ratio of
compared using 2 tests or Fisher exact tests for categori-
group 1A was set as 100%. mtDNA levels (Fig. 1) among
cal variables and unpaired t-tests, Wilcoxon Mann-Whit-
HIV-negative patients with chronic HCV infection
ney tests or Kruskal-Wallis ANOVA on the ranks for
(group 2: mean mtDNA/nDNA ratio ϭ 114% Ϯ 54%)
continuous variables, as appropriate. Those statistical
did not differ from group 1A, as did those of HIV-in-
analyses were performed using the Sigma Stat for Win-
fected patients receiving ART without D drugs (group
dows software version 1.0 (Jandel Corporation, San
1B: mean mtDNA/nDNA ratio ϭ 114% Ϯ 46%). How-
Rafael, CA). Both univariate and multivariate linear re-
ever, when D drugs were used as part of the antiretroviral
gression analyses were done using SPSS for Windows soft-
treatment, mtDNA levels were reduced by 47% com-
ware Release 11.0.0 (SPSS Inc., Chicago, IL). Trends in
pared with biopsies from individuals treated without D
mtDNA over time on therapy were estimated using an
drugs (group 1C: mean mtDNA/nDNA ratio ϭ 60% Ϯ
exponential model that allows variation in the rate of
27%, P Ͻ .0001) and reduced by 40% when compared
initial decline and subsequent long-term level (asymp-
tote). The nonlinear model was fitted by least-squares in
The comparison of mtDNA levels among individual
SPSS. The flexibility in the rate of decline allows an ap-
NRTIs (Table 2) revealed reduced amounts of mtDNA in
proximately linear trend should the data suggest this.
livers of patients receiving stavudine, didanosine, or zal-citabine (mtDNA/nDNA ratios of 62%, P ϭ .0004;
44%, P Ͻ .0001 and 51%, P ϭ .04 of group 1A-levels,respectively). In contrast, mtDNA levels among patients
Demographics, Virology, and Immunology. Out of
receiving zidovudine, lamivudine, or abacavir were not
a total of 94 patients biopsied, 80 subjects had HIV and
reduced (mean mtDNA/nDNA ratios of 111%, P ϭ .79;
chronic HCV infection (group 1) and 14 patients had
96%, P ϭ .41; 77%, P ϭ .07, respectively). There was no
chronic HCV infection but no HIV infection (group 2).
statistical association between the use or nonuse of PIs or
Eleven patients had no antiretroviral therapy at the time
NNRTIs (at the time of biopsy, or ever) and mtDNA
of biopsy (group 1A). Within group 1A, nine patients
depletion. Furthermore, there were no significant corre-
were naı¨ve to antiretroviral treatment, one female had a
lations of mtDNA levels with total or current time on
3-month exposure to zidovudine during pregnancy 18
months prior to biopsy, and one male had interrupted a
Six patients were treated with two D drugs at the time
PI-containing first line therapy of 42 months duration for
of biopsy; all were receiving the combination of stavudine
reasons of revised treatment guidelines; his treatment was
and didanosine (Fig. 1). The mean mtDNA/n-DNA ratio
in these patients was only 41% Ϯ 10%, which represents
The remaining 69 HIV- and HCV-coinfected patients
36% of the ratio in D drug–negative patients (P Ͻ
had uninterrupted antiretroviral therapy. At the time of
.0001). Compared with the 24 patients receiving stavu-
biopsy, 35 were treated without D drugs with various
dine as the only D drug, the mean mtDNA/nDNA ratio
combinations of zidovudine, lamivudine, and abacavir
among subjects receiving a combination of stavudine and
(group 1B) and 34 were treated with one or two D drugs
didanosine was decreased by 53% (P Ͻ .0001).
(i.e., zalcitabine, didanosine, and stavudine) (group 1C).
To further characterize treatment and disease-related
There were no statistical differences between the group
factors that may influence mtDNA levels in patients re-
1 subgroups with respect to age, sex, HCV genotype,
ceiving treatment (group 1B and 1C, n ϭ 69), multivar-
HCV viral load, time of known HIV infection, and CD4
iate regression analyses were performed in which mtDNA
count (Table 1). The D drug–treated individuals had a
levels were considered as the dependent variable. Each of
slightly shorter mean time of known HCV infection than
the factors presented in Table 1 was considered as a co-
Table 1. Demographic, Virologic, and Immunologic Characteristics Among Patients With HIV/HCV Coinfection P Value HIV and HCV Coinfection (no ART; n ؍ 11) (D drug–negative; n ؍ 35) (D drug–positive; n ؍ 34) Demographics, virology, and immunology
mtDNA/nDNA ratio (mean of group 1A: 100%)
Group variability is calculated as standard deviation. Abbreviations: NS, not significant; NA, not applicable. *Two patients had received ART prior to but not at the time of biopsy. Their treatment is discussed in the text.
variate in both univariate and multivariate regressionanalyses. Current use of D drugs was significantly associ-ated with mtDNA levels in a univariate analysis (P Ͻ.001), while no significant associations were detected foruse or duration of current PI therapy (P ϭ .41, P ϭ .47)or NNRTI therapy (P ϭ .12, P ϭ .12). In addition, theeffect of D drug treatment on mtDNA levels was inde-pendent of the duration of current ART (P ϭ .72). Fur-thermore, neither the cumulative time on ART (P ϭ .24)nor the cumulative time on PI (P ϭ .20) or NNRTI (P ϭ.55) had any influence. With regard to demographic andHIV disease-related effects, no significant associationswere detected between mtDNA levels and age (P ϭ .49),gender (P ϭ .73), CD4 T cell count (P ϭ .62), or unde-tectable HIV viral load (P ϭ .60). Similarly, HCV viralload (P ϭ .96), duration of HCV infection (P ϭ .72),evidence of hepatic inflammatory activity (P ϭ .11), andfibrosis (P ϭ .46) were not significantly associated withmtDNA levels. However, there was a trend toward anassociation between HCV genotype 1 and mtDNA levels(P ϭ .09) that was found to be significant after adjustingfor the effect of D drug use in multivariate regressionanalysis (P ϭ .04). Further assessment of D drug use and
Fig. 1. mtDNA/nDNA ratio in liver among all subjects (mean of group
HCV genotype status in a general linear model analysis
1A: 100%). The horizontal bar represents group means. The patients withlactate above or equal to the ULN are marked with a star.
revealed no evidence for an interaction between these
Table 2. Characteristics of Patients With HIV/HCV Coinfection With Regard to the Use of Particular NRTIs at the Time of Biopsy Zidovudine Lamivudine Abacavir Stavudine Didanosine P HIV and HCV Coinfection
Group variability is calculated as standard deviation. Patients receiving zalcitabine (n ϭ 2) are discussed in the text. Abbreviation: NS, not significant. *The “no NRTI” group was excluded in the statistical comparison (Kruskal-Wallis ANOVA on the ranks). †Two patients had received ART prior to but not at the time of biopsy. Their treatment is discussed in the text.
variables (P ϭ .71), suggesting that these factors contrib-
ULN Ϯ 0.16). Lactate was higher in both treatment
ute independently to mtDNA depletion in the liver. No
groups (i.e., in patients receiving D drugs and in patients
other tested variable contributed significantly to mtDNA
without D drugs) compared with subjects without ART
depletion in multivariate regression analyses, while the
at the time of biopsy (P ϭ .019 and P ϭ .042, respec-
association between use of D drugs and mtDNA levels
tively). However, there was no statistical difference of
remained highly significant after adjusting for all covari-
lactate with respect to the D drug status in patients on
antiretroviral treatment. The lactate of HIV-negative pa-
We found a significant decline in mtDNA over time on
current treatment with D drugs (Fig. 2), dropping froman initial mean of 99.4% (SE, 8.0; group 1A mean,100%) to a long-term value estimated as 57.5 % (SE, 5.3;P Ͻ .000004). However, most of this decline occurs inthe first 6 to 7 months, with no evidence of decline be-yond this time (P ϭ .86).
Qualitative mtDNA alterations (e.g., mtDNA dele-
Serum Lactate. Only three individuals had a serum
lactate above or equal to the ULN. Among the three sub-groups of HIV/HCV coinfection, lactate was highest un-der D drug treatment (group 1C: 0.60ϫ ULN Ϯ 0.28),followed by D drug–negative subjects (group 1B: 0.50ϫULN Ϯ 0.19) and by patients without antiretroviral
Fig. 2. Trends in mtDNA/nDNA ratio over time on D drug therapy
treatment at the time of biopsy (group 1A: 0.35ϫ
tients with chronic HCV infection (group 2: 0.43ϫ
ration of the treatment in groups 1B and 1C. However, if we
ULN Ϯ 0.12) did not statistically differ from its HIV
had excluded the two patients with prior ART from group
1A, the significance levels of our results would not have
Compared with patients without ART, the mean lac-
changed, and the association between mtDNA depletion
tate was elevated in subjects using didanosine (0.71ϫ
and D drug treatment at the time of biopsy in particular
ULN, P ϭ .016) and stavudine (0.59ϫ ULN, P ϭ .027),
would have still been detectable (P ϭ .0001).
but also in those receiving zidovudine (0.50ϫ ULN, P ϭ
We detected a trend (P ϭ .09) toward an association
.04), lamivudine (0.52ϫ ULN, P ϭ .02) and abacavir
between HCV genotype I for mtDNA depletion that was
(0.56ϫ ULN, P ϭ .046). In summary, lactate levels
found to be significant after adjusting for the effects of D
tended to be elevated among subjects receiving D drugs,
drug use. Interestingly, a similar association has been docu-
but this was not statistically significant (Table 2).
mented previously with HCV genotype Ib.17 Such HCV-
There was no correlation between mtDNA levels and
associated mitochondrial injury could be explained by
lactate in the group of all 94 HCV-infected individuals or
increased oxidative stress or by several other mecha-
its subgroups. Stratification of the mtDNA measure-
ments into quartiles revealed only a nonsignificant trend
No further virologic, immunologic, histologic, demo-
toward lactate elevation with mtDNA depletion among
graphic, or treatment-related variables contributed signif-
patients coinfected with HCV and HIV.
icantly to mtDNA depletion in the multivariate analysis.
The subjects with lactate above or equal to the ULN
The conclusions with regard to the association between
were all HIV-positive and treated with stavudine at the
the use of individual D drugs and mtDNA depletion are
time of biopsy; two of the three were given additional
limited by the cross-sectional design of the study, in
didanosine. The mean mtDNA/nDNA ratio in the liver
which the treatment with individual NRTIs is not inde-
of these three patients was 38% Ϯ 11% of untreated
pendent from each other and is not randomized. This
HIV- and HCV-coinfected controls (P ϭ .003). Com-
may be illustrated by the fact that most patients treated
pared with the remaining patients on D drugs (67% Ϯ
with didanosine were also receiving stavudine. However,
28%), mtDNA levels were significantly diminished (P ϭ
the higher mtDNA levels in individuals receiving stavu-
.017). Furthermore, the mtDNA/nDNA values of pa-
dine as the only D drug, compared with those receiving
tients with serum lactate above or equal to the ULN
stavudine plus didanosine, supports an independent ef-
(range: 25%– 47%) were outside the range of mtDNA
fect of didanosine. The coadministration of two NRTIs
measurements in individuals without antiretroviral ther-
was previously observed to have additive or synergistic
apy (group 1A range: 49%–150%) or D drugs (group 1B
Our model of mtDNA trends over time (Fig. 2) sug-
Other Measurements. Between the subgroups of
gests an mtDNA decline during the initial 6 months of D
group 1 (groups 1A, 1B, and 1C), there were no differ-
drug therapy, with no further decline beyond this time.
ences with regard to the histologic degrees of liver fibrosis,
The kinetics of mtDNA loss are initially influenced by the
inflammatory activity, macro- or microvesicular steatosis,
degree of gamma-polymerase inhibition and presumably
or the serum levels of ALT (not shown). There was also no
also by the rates of cell division and mtDNA turnover.5
association between macro- or microvesicular steatosis
Eventually, stable mtDNA levels arise in accordance with
The mean mtDNA/nDNA ratio in the D drug–treated
Discussion
HIV patients was 53% lower, compared with patients receiv-
This study analyzed the hepatic mtDNA content in
ing anti-HIV treatment without D drugs. The question then
patients with chronic HIV and HCV coinfection. The
arises as to whether or not this relatively moderate mtDNA
HIV patients were divided into three subgroups accord-
depletion may be functionally relevant, given the fact that
ing to their antiretroviral regimen at the time of biopsy.
wild type mtDNA levels in the order of 20% can maintain
The major finding is that antiviral therapy with at least
almost normal cell function in vitro.19 Several observations
one of the D drugs (didanosine, stavudine, and zalcita-
indicate that the in vitro threshold of mtDNA levels within
bine) is associated with mtDNA depletion in liver,
cells may differ from the in vivo situation in a tissue. For
whereas no such relation was detected between mtDNA
example, anaerobic ATP production by ample glucose sup-
levels and treatment with other antiretroviral drugs.
ply in the medium may allow a relatively long cell survival in
Two individuals within group 1A were not naı¨ve to anti-
vitro despite severe mtDNA depletion. Fibrotic tissue may
retroviral treatment. We chose to include these patients in
also be more resistant to mtDNA depletion and thus main-
our analysis because we also did not select for a specific du-
tain some residual mtDNA. Indeed, in situ hybridization
studies in patients with proven mitochondrial cytopathies
5. Walker UA, Setzer B, Venhoff N. Increased long-term mitochondrial tox-
failed to establish an in vivo threshold necessary for mtDNA
icity in combinations of nucleoside analogue reverse-transcriptase inhibi-tors. AIDS 2002;16:2165–2173.
mutations to trigger a biochemical dysfunction in clinically
6. Gaou I, Malliti M, Guimont MC, Letteron P, Demeilliers C, Peytavin I,
affected tissue.20 It is also interesting to note that the magni-
Degott C, et al. Effect of stavudine on mitochondrial genome and fatty
tude of mtDNA depression was similar in adipose tissue of
acid oxidation in lean and obese mice. J Pharmacol Exp Ther 2001;297:516 –523.
patients suffering from HIV-associated lipoatrophy14 and in
7. Gerschenson M, Nguyen VT, St Claire MC, Harbaugh SW, Harbaugh
hepatic tissue of inherited mtDNA replication defects with
JW, Proia LA, Poirier MC. Chronic stavudine exposure induces hepatic
mitochondrial toxicity in adult Erythrocebus patas monkeys. J Hum Virol
Our investigations do not demonstrate a clear relation-
8. Brivet FG, Nion I, Megarbane B, Slama A, Brivet M, Rustin P, Munnich
ship between mtDNA depletion in hepatic tissue and an
A. Fatal lactic acidosis and liver steatosis associated with didanosine and
increase in serum lactate, but it is important to note that
stavudine treatment: a respiratory chain dysfunction? J Hepatol 2000;32:
lactate levels were normal in virtually all patients. In contrast
9. Chariot P, Drogou I, de Lacroix-Szmania I, Eliezer-Vanerot MC, Chazaud
to previous reports,22 there was no lactate elevation in indi-
B, Lombes A, Schaeffer A, et al. Zidovudine-induced mitochondrial dis-
viduals receiving stavudine compared with zidovudine, al-
order with massive liver steatosis, myopathy, lactic acidosis, and mitochon-
though lactate was somewhat higher with D drug treatment
drial DNA depletion. J Hepatol 1999;30:156 –160.
in our study. We are unable to determine the exact reasons
10. Gerard Y, Maulin L, Yazdanpanah Y, Tribonniere X, Amiel C, Maurage
CA, Robin S, et al. Symptomatic hyperlactataemia: an emerging compli-
for this discrepancy, but possible explanations include the
cation of antiretroviral therapy. AIDS 2000;14:2723–2730.
HCV status of our principal study population,17 effects on
11. John M, Mallal S. Hyperlactatemia syndromes in people with HIV infec-
mitochondria or hepatic tissue unrelated to mtDNA deple-
tion. Curr Opin Infect Dis 2002;15:23–29.
12. Leclercq P, Roth H, Bosseray A, Leverve X. Investigating lactate metabo-
tion (as demonstrated for zidovudine4,5,23), and additional
lism to estimate mitochondrial status. Antivir Ther 2003;6(Suppl. 4):16.
mitochondrial toxicity in extra-hepatic tissues.9,24 Our study
13. Scheuer PJ. Classification of chronic viral hepatitis: a need for reassess-
was also not powered to examine associations between hy-
perlactatemia and NRTI therapy. The findings therefore do
14. Walker UA, Bickel M, Lu¨tke Volksbeck SI, Ketelsen UP, Schofer H, Setzer
B, Venhoff N, et al. Evidence of nucleoside analogue reverse transcriptase
not exclude an important contribution of mtDNA levels in
inhibitor-associated genetic and structural defects of mitochondria in adi-
liver on serum lactate. This is also supported by the observation
pose tissue of HIV-infected patients. J Acquir Immune Defic Syndr 2002;
that among the D drug–treated subjects, those with a serum
15. Hammond EL, Sayer D, Nolan D, Walker UA, Ronde A, Montaner JS,
lactate above or equal to the ULN had a significant mtDNA
Cote HC, et al. Assessment of precision and concordance of quantitative
depletion compared with those with a normal lactate.
mitochondrial DNA assays: a collaborative international quality assurance
We found that antiviral treatment with D drugs— but
study. J Clin Virol 2003;27:97–110.
not with non–D drugs—is associated with hepatic mtDNA
16. Thiers V, Jaffredo F, Tuveri R, Chodan N, Brechot C. Development of a
simple restriction fragment length polymorphism (RFLP) based assay for
depletion in HCV- and HIV-coinfected subjects. We have
HCV genotyping and comparative analysis with genotyping and serotyp-
evidence that a moderate mtDNA depletion in hepatic tissue
ing tests. J Virol Methods 1997;65:9 –17.
alone is not sufficient to cause mild hyperlactataemia, but
17. Barbaro G, Di Lorenzo G, Asti A, Ribersani M, Belloni G, Grisorio B,
Filice G, et al. Hepatocellular mitochondrial alterations in patients with
that more pronounced mtDNA depletion may represent an
chronic hepatitis C: ultrastructural and biochemical findings. Am J Gas-
important factor contributing to lactic acidosis.
18. Rust C, Gores GJ. Does hepatitis C cause liver injury by pathways associated
with mitochondrial dysfunction? Am J Gastroenterol 1999;94:2003–2005.
BMBF, Kompetenznetz HIV/AIDS (grant number:
19. Attardi G, Yoneda M, Chomyn A. Complementation and segregation
behavior of disease-causing mitochondrial DNA mutations in cellularmodel systems. Biochim Biophys Acta 1995;1271:241–248. References
20. Moraes CT, Ricci E, Petruzzella V, Shanske S, DiMauro S, Schon EA,
Bonilla E. Molecular analysis of the muscle pathology associated with
1. Palella FJ Jr, Delaney KM, Moorman AC, Loveless MO, Fuhrer J, Satten
mitochondrial DNA deletions. Nature Genet 1992;1:359 –367.
GA, Aschman DJ, et al. Declining morbidity and mortality among patients
21. Mandel H, Hartman C, Berkowitz D, Elpeleg ON, Manov I, Iancu TC.
with advanced human immunodeficiency virus infection. HIV Outpatient
The hepatic mitochondrial DNA depletion syndrome: ultrastructural
Study Investigators. N Engl J Med 1998;338:853– 860.
changes in liver biopsies. HEPATOLOGY 2001;34:776 –784.
2. Yeni PG, Hammer SM, Carpenter CC, Cooper DA, Fischl MA, Gatell
22. John M, Moore CB, James IR, Nolan D, Upton RP, McKinnon EJ, Mallal
JM, Gazzard BG, et al. Antiretroviral treatment for adult HIV infection in
SA. Chronic hyperlactatemia in HIV-infected patients taking antiretrovi-
2002: updated recommendations of the International AIDS Society–USA
ral therapy. AIDS 2001;15:717–723.
23. Olano JP, Borucki MJ, Wen JW, Haque AK. Massive hepatic steatosis and
3. Brinkman K, Smeitink JA, Romijn JA, Reiss P. Mitochondrial toxicity
lactic acidosis in a patient with AIDS who was receiving zidovudine. Clin
induced by nucleoside-analogue reverse-transcriptase inhibitors is a key
factor in the pathogenesis of antiretroviral-therapy-related lipodystrophy.
24. Vittecoq D, Jardel C, Barthelemy C, Escaut L, Cheminot N, Chapin S,
Sternberg D, et al. Mitochondrial damage associated with long-term anti-
4. Kakuda TN. Pharmacology of nucleoside and nucleotide reverse transcriptase
retroviral treatment: associated alteration or causal disorder? J Acquir Im-
inhibitor-induced mitochondrial toxicity. Clin Ther 2000;22:685–708.
mune Defic Syndr 2002;31:299 –308.
THE HUMBLE PRUNE ACHIEVES SUPERFRUIT STATUS From today, the prune can shake off any old fashioned associations and claim its rightful position as a modern day ‘Superfood’, following an announcement from nutritional consultant and Health Journalist of the Year, Michael van Straten – who originally coined the term ‘Superfood’ in the lates Compelling and conclusive scientific
CASE STUDIES: PSYCHIATRIC ASSESSMENT OF ROAD TRAFFIC ACCIDENT CLAIMANTS Dr Lana Kossoff Consultant Psychiatrist November 2007 Tel: (02) 9252 4007 Fax: (02) 9252 4766 email: [email protected] CASE STUDY 1 Mr Brian SMITH Date of Accident: 11 July 2003 Mr Brian Smith is a 38 year old former truck driver who was involved in a road traffic acciden
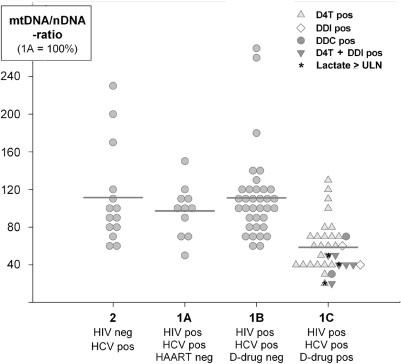 Table 1. Demographic, Virologic, and Immunologic Characteristics Among Patients With HIV/HCV Coinfection
Table 1. Demographic, Virologic, and Immunologic Characteristics Among Patients With HIV/HCV Coinfection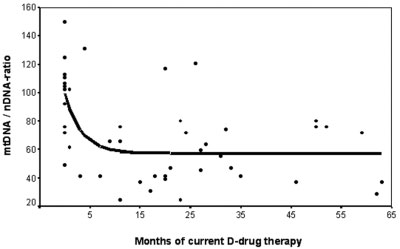 Table 2. Characteristics of Patients With HIV/HCV Coinfection With Regard to the Use of Particular NRTIs
Table 2. Characteristics of Patients With HIV/HCV Coinfection With Regard to the Use of Particular NRTIs