Copyright 2006 by the American Psychological Association
Heart Rate Increase to Alcohol Administration and Video Lottery Terminal
Play Among Probable Pathological Gamblers and
Pamela Collins, Shondalee Eisnor, and Michael Ellery
The authors examined heart-rate responses to alcohol consumption and video lottery terminal (VLT)play. Regular VLT players (30 probable pathological gamblers [PPGs]; 30 nonpathological gamblers[NPGs]) were randomized to an alcohol (mean postdrinking blood alcohol concentration ϭ 0.056%) orplacebo condition. Heart rate was recorded at pre- and postdrinking baselines and during VLT play. Consistent with an earlier study (S. H. Stewart, P. Collins, J. R. Blackburn, M. Ellery, & R. Klein, 2005),alcohol-condition participants displayed elevated heart rates relative to placebo-condition participantsonly at postdrinking and VLT play. Moreover, alcohol-condition participants showed a greater heart rateincrease to VLT play than did placebo-condition participants. However, PPGs were not more susceptibleto alcohol- and/or VLT play-induced heart rate accelerations than were NPGs. Implications for gambling/alcohol-disorder comorbidity are discussed. Keywords: heart rate, alcohol, gambling, video lottery terminals, comorbidity
Many studies suggest elevated rates of alcohol use disorders
(VLT) play condition chose to purchase alcoholic beverages dur-
among those with pathological gambling disorders and vice versa
ing play as compared with only 40% of those regular gamblers
(Crockford & el-Guebaly, 1998; Stewart & Kushner, 2003). For
assigned to a control activity (Stewart et al., 2002). There are
example, Kausch (2003) found that 66% of those with disordered
several possible explanations for this high rate of co-occurrence.
gambling reported a lifetime history of substance use disorder,
First, heavy drinking might cause gambling problems (e.g., Ellery,
with alcohol being the most commonly abused substance in this
Stewart, & Loba, 2005). Second, gambling problems might cause
clinical sample. This rate is substantially elevated relative to life-
heavy drinking. Or, finally, some third variable might cause both
time prevalence in the general population (Robins, Locke, &
alcohol use disorders and pathological gambling (Grant, Kushner,
Regier, 1991). The overlap of alcohol and gambling occurs not
& Kim, 2002; Stewart & Kushner, 2003).
only at the diagnostic level but also at the behavioral level (i.e.,
Researchers have begun to explore what types of third variables
frequent combining of these two activities). This behavioral over-
might help explain the high comorbidity between alcohol use and
lap is evidenced in both survey (e.g., Focal Research, 1998) and
gambling disorders. For example, recent evidence suggests a com-
behavioral observation studies (e.g., Stewart, McWilliams, Black-
mon genetic vulnerability for pathological gambling and alcohol-
burn, & Klein, 2002). For example, in a lab-based experimental
use disorders (Slutske et al., 2000). Others (e.g., Comings et al.,
study, 73% of regular gamblers assigned to a video lottery terminal
1996; Potenza, 2001) have suggested that both disorders mayinvolve dysregulation of dopaminergic brain circuitry. This dys-regulation may be genetically mediated or environmentally medi-ated (e.g., as a consequence of chronic stress; Lin, Bruijnzeel,
Sherry H. Stewart, Pamela Collins, Shondalee Eisnor, and Michael
Schmidt, & Markou, 2002) and is thought to result in increased
Ellery, Department of Psychology, Dalhousie University, Halifax, Nova
susceptibility to incentive reward motivation.
Scotia, Canada; Jordan B. Peterson, Department of Psychology, Universityof Toronto, Toronto, Ontario, Canada.
Research over the last few decades has suggested that heart rate
Shondalee Eisnor is now at the Maritime School of Social Work,
increase may constitute a psychophysiological marker of incentive
reward motivation susceptibility, at least under some conditions
Sherry H. Stewart is now at the Departments of Psychiatry and Psy-
(Fowles, 1980; Fowles, Fisher, & Tranel, 1982), as the cardiovas-
cular system steps up its output to prepare the body for motivated,
This research was supported by a generous grant from the Nova Scotia
goal-directed action (Wright, Killebrew, & Pimpalapure, 2002).
Gaming Foundation. Sherry H. Stewart is supported through an Investiga-
Under conditions of high expectancy of eventual reward, this
tor Award from the Canadian Institutes of Health Research.
increase appears particularly evident (Ladouceur, Sevigny, Blaszc-
Correspondence concerning this article should be addressed to Sherry H.
Stewart, Department of Psychology, Dalhousie University, Halifax, Nova
zynski, O’Connor, & Lavoie, 2003). Incentive reward (i.e., tech-
Scotia B3H 4J1, Canada. E-mail: [email protected]
nically, response to a cue for consummatory reward or to novelty;
STEWART, PETERSON, COLLINS, EISNOR, AND ELLERY
Gray, 1982) appears mediated primarily by the dopaminergic
Until recently, however, no research had examined heart-rate
reward systems (Gray, 1982; Panksepp, 1999) originating in the
responses to alcohol and gambling in the same individuals within
ventral tegmental area, and involving the extended amygdala, the
the same study. Stewart, Collins, Blackburn, Ellery, and Klein
nucleus accumbens, and the orbital frontal cortex (Blackburn,
(2005) examined heart rate responses to VLT play and alcohol
Pfaus, & Phillips, 1992) and/or anterior cingulate cortex (Kalivas
consumption, alone and in combination. Forty-four regular VLT
& McFarland, 2003). Activation of this system has been hypoth-
players (i.e., a group including both probable pathological and
esized as the primary commonality linking drugs of abuse in
nonpathological gamblers) were randomly assigned to a moder-
ately intoxicating dose of alcohol or a control (mix only) beverage
Some have argued that heart-rate increases in response to alco-
condition. Heart rate was recorded at three times: at a predrinking
hol intake in the resting state reflect a psychomotor stimulant-like
baseline, at a postdrinking baseline, and during VLT play. Through
response to alcohol (similar to that observed for established stim-
comparison of degree of increases from pre- to postdrinking base-
ulant drugs like cocaine; e.g., Peterson et al., 1996). Peterson, Pihl,
line among gamblers assigned to the alcohol and control beverage
Seguin, Finn, and Stewart (1993) hypothesized that the alcohol-
conditions, the results confirmed previous findings that alcohol
induced baseline resting heart rate increase characteristic of sons
consumption alone increased heart rate (cf. Peterson et al., 1993,
of multigenerational alcoholics was a consequence of an enhanced
1996; Stewart et al., 1992). The study also demonstrated that VLT
psychomotor stimulant response to alcohol. Among animal re-
play alone increased heart rate, like other forms of gambling (cf.
searchers, it has been long known that alcohol is capable of
Coventry & Hudson, 2001; Griffiths, 1993; Leary & Dickerson,
directly activating the dopamine reward system (e.g., Deminiere,
1985), among players in the control beverage condition, and that
Piazza, LeMoal, & Simon, 1989; McBride, Murphy, Lumeng, &
the combination of VLT play and alcohol-intensified heart rate
Li, 1990). Further evidence for baseline heart rate increase as an
increase, relative to either condition alone. Given the evidence
index of the reward properties of alcohol intake comes from a
suggesting that baseline heart rate increases might index the in-
variety of sources. For example, baseline heart rate increases to
centive reward characteristics of certain forms of addictive activ-
alcohol have been associated with increased alcohol use (Peterson
ity, it appears that the combination of VLT play and alcohol use
et al., 1993), alcoholic family history (Stewart, Finn, & Pihl,
1992), and increases in positive mood states (Conrod, Peterson, &
The current study was designed to replicate and extend Stewart
Pihl, 2001). Furthermore, Boileau et al. (2003) recently directly
et al. (2005). We, therefore, investigated heart-rate responses to a
demonstrated that dopamine was in fact released in the ventral
moderately intoxicating dose of alcohol, to VLT play, and to their
striatum and nucleus accumbens as a consequence of alcohol
combination, among a sample of regular VLT players. We also
intake in humans (using [11C]raclopride positron-emission tomog-
made a number of methodological improvements. First, because it
raphy scans), and that such release did correlate both with alcohol-
was not designed to examine expectancy effects, our earlier study
induced baseline heart-rate increase and impulsiveness. Such re-
used a mix-only beverage rather than a placebo beverage in the
lease may be a direct or first order consequence of alcohol’s effect
control beverage condition. To control for expectancy effects, we
on the dopaminergic systems; alternatively, at least in some cases,
used a placebo-beverage condition in the present study. Second,
it might also be mediated indirectly via alcohol’s stimulation of
during our original study, participants played a video poker game
endogenous opiate release (Peterson et al., 1996), as alcohol-
on the VLT machines. In the present study we had participants
induced baseline heart-rate increase can be reduced to zero as a
play a “spinning reels” game, which is a video-simulated slot
consequence of the coadministration of naltrexone, an opiate an-
machine game. This particular game is popular with most VLT
tagonist (Peterson, Conrod, Vassileva, Gianoulakis, & Pihl, in
players (Focal Research, 1998). Finally, the previous study did not
press). Although opiates are primarily regarded as analgesics,
include a sufficient sample size to test whether the heart-rate
cocaine also has potent analgesic properties, and opiates have
increases to alcohol, VLT play, and their combination were dif-
powerful psychomotor stimulant effects (Gianoulakis, 1996; Gray,
ferent among probable pathological gamblers (PPGs) and non-
pathological gambler controls (NPGs). Brunelle, Assaad, Pihl,
Incentive reward activation also appears to mediate at least
Tremblay, and Vitaro (2003) have recently demonstrated that
some of the pleasurable and addictive aspects of gambling. Grif-
elevated scores on a measure of gambling problems (the South
fiths (1991) has contended that pathological gamblers engage in
Oaks Gambling Screen [SOGS]; Lesieur & Blume, 1987) were in
gambling for its euphoric, arousal-enhancing consequences. In
fact associated with greater sensitivity to alcohol-induced heart
indirect keeping with such a hypothesis, Zack and Poulos (2004)
rate increases. In the present study, we increased our sample size
have recently demonstrated that amphetamine, a potent dopamine
so that we could determine whether PPGs, as identified on the
agonist, primes motivation to gamble in problem gamblers. Fur-
SOGS, might show comparatively increased heart rate to VLT
thermore, heart-rate increase characterizes regular gamblers during
play, alcohol, and/or their combination, relative to NPGs.
gambling bouts (Coventry & Hudson, 2001; Griffiths, 1993) and
In the present study, we used a 2 ϫ 2 ϫ 3 (Gambler Group ϫ
appears related to the excitement generated by the possibility of
Beverage Condition ϫ Testing Time) mixed-model design with
winning money (Ladouceur et al., 2003) and to the similarity of the
two between- and one within-subjects factor. We divided regular
testing situation to the real-world gambling context (Diskin, Hod-
VLT players into probable pathological versus nonpathological
gins, & Skitch, 2003). Taken together, such findings suggest the
gambler groups on the basis of scores on the SOGS (Lesieur &
possibility that heart-rate increase may represent a common psy-
Blume, 1987). Participants in each gambler group were randomly
chophysiological marker of susceptibility to reward from both
assigned to an alcohol or a placebo– control beverage condition.
drinking and gambling and, thus, susceptibility to developing
Heart rate was measured at three testing times: predrinking base-
line, postdrinking baseline, and during VLT play. We tested sev-
eral hypotheses that follow from the idea that enhanced dopamine/
photoplethysmograph was attached to the middle finger of the nondomi-
incentive–reward sensitivity underlies alcohol abuse/pathological
nant hand. Mean heart rate was calculated via the ProCompϩ/Biograph
program first as the average interbeat interval (IBI) at each testing phase,
First, we expected a two-way Beverage Condition ϫ Testing
across the entire recording interval. IBI was then converted to beats perminute (bpm). Participants gambled on VLTs that were identical in all
Time interaction, consisting of the following three effects: (a) heart
respects to commercial VLTs appearing in licensed establishments in the
rate increase to alcohol consumption alone, evidenced by an in-
province of Nova Scotia (Stewart, Blackburn, & Klein, 2000). VLTs are
crease in heart rate from pre- to postdrinking baseline in the
similar to slot machines in that both are electronic gaming machines that
alcohol beverage condition (with no change in the placebo bever-
operate using random number generators. Both VLTs and slot machines
age condition) and by a greater heart rate in the alcohol beverage
can be used to play spinning reels-type games. However, VLTs do not
condition relative to the placebo beverage condition at postdrink-
contain mechanical reels but rather use video-simulated reels.
ing baseline (but no difference between beverage conditions atpredrinking baseline); (b) heart-rate increases to VLT play alone,
evidenced by an increase in heart rate from postdrinking baselineto the VLT play phase in both the alcohol and placebo beverage
For the purposes of telephone screening, we developed a standard
conditions and by an increase in heart rate from predrinking
telephone script incorporating the scorable items from the SOGS (Lesieur
baseline in the placebo beverage condition; and (c) heart rate
& Blume, 1987) to appropriately assign the participant to a condition
increase to the combination of alcohol intake and VLT play,
within the 2 ϫ 2 design. PPGs were overrecruited (i.e., actively sought as
relative to either activity alone, evidenced by a greater heart rate in
potential participants on the basis of the results of telephone screening) to
the alcohol beverage condition relative to the placebo beverage
equate the n in each cell of the 2 ϫ 2 (Beverage Condition ϫ Gambler
condition at VLT play (but no difference between beverage con-
Group) between-subjects design. This was accomplished by continuing torecruit PPGs into the study after the two cells (i.e., alcohol and placebo) of
ditions at predrinking baseline) and by a greater heart rate increase
NPGs had been filled. Within each gambler group, random assignment to
to VLT play from predrinking baseline in those who had consumed
one of the two beverage conditions was accomplished via lottery at the
alcohol relative to those who had consumed placebo. Second, we
time of participant screening. Eligible individuals were instructed to fast
expected a three-way Gambler Group ϫ Beverage Condition ϫ
for 4 hr and to abstain from alcohol and drugs for 24 hr prior to testing (cf.
Time interaction, such that all the effects listed above would be
Testing occurred during the afternoon in a laboratory modified to re-
semble a bar. The “bar-lab” contained a bar and two VLTs. Consent wasobtained, fasting was verified verbally, and participants were weighed to
determine alcohol dose. BAC was taken to verify abstinence from alcohol
and to provide a predrinking baseline measure. Participants were provided$80 (Canadian) compensation. Questionnaires were administered. The
Sixty regular VLT players were recruited via newspaper and local cable
photoplethysmograph was attached and an 8-min habituation period fol-
TV advertisement.1 Half were PPGs, according to their SOGS scores; the
lowed. Predrinking baseline heart rate was continuously recorded for 5
other half were NPGs. To be eligible for participation, respondents had to
min3 followed by administration of a demographics questionnaire.
play VLTs at least once a month, be familiar with a spinning reels game,
Participants were provided with their assigned beverage (alcohol or
and consume alcohol at least once a month. These were the same inclusion
placebo) in 3– 4 glasses, depending on total volume. Because this study
criteria used for our last study (Stewart et al., 2005). Because the study
was also designed to test expectancy effects, all participants were informed
involved alcohol administration, those scoring Ն6 on the Brief Michigan
that they would be receiving a moderate dose of alcohol, consisting of the
Alcoholism Screening Test (Pokorny, Miller, & Kaplan, 1972), indicative
equivalent of 3– 4 mixed bar drinks. For those in the alcohol condition, the
of possible problem-drinker status, were excluded (Stewart et al., 2005).
alcohol dose was 1.55 mL 50% United States Pharmacopeia units of
Those with medical contraindications to alcohol consumption were ex-cluded (Stewart et al., 2005).
We compared our sample with 711 regular VLT players in Nova Scotia
1 Eighty-three people responded to recruitment advertisements. Of these,
on demographics and addictive behaviors (Focal Research, 1998). Our
67 met study inclusion criteria. Reasons for exclusion included possible
sample appeared representative of regular players, except that our partic-
problem drinker status (i.e., scoring above the cutoff-point on the Brief
ipants were less likely to be married or cohabiting (29% vs. 57%), had
Michigan Alcoholism Screening Test), medical contraindications to alco-
played VLTs for longer (Ms ϭ 6.8 vs. 3.6 years), and were more likely to
hol ingestion, and lack of familiarity with the spinning reels game. Of the
be probable pathological gamblers (50% vs. 16%).2
67 eligible individuals who initially agreed to participate, 60 appeared asscheduled; the rest were no-shows or cancellations.
The Focal Research (1998) report did not include measures of vari-
ability to permit direct statistical comparisons with the present results. It
Information on demographic characteristics and addictive behaviors was
should also be noted that PPGs were defined differently in the two studies.
obtained via author-compiled questionnaires. Subjective intoxication was
In the present study, PPGs were defined by SOGS scores (Lesieur &
measured using a 100-mm visual analog scale (VAS). Gambler group
Blume, 1987), whereas a more stringent measure, developed by the au-
membership was determined by screening scores on the SOGS—a reliable
thors, was used in the Focal Research study. Moreover, as noted in the
and valid screen for problem gambling. Those scoring Ն5 on the SOGS
procedure section, probable pathological gamblers were purposely overre-
were assigned to the PPG group and all others to the NPG group (cf.
cruited in the present study to equate cell n in the 2 ϫ 2 (Gambler Group ϫ
Lesieur & Blume, 1987). Blood alcohol concentrations (BACs) were
Beverage Condition) between-subjects design.
measured using an Alcosensor III (Intoximeters, St. Louis, Missouri).
3 The length of the heart-rate recording interval at each of the two
Heart rate was collected with a photoplethysmograph via the ProCompϩ/
baseline phases was increased from 90 s in our original study to 5 min in
Biograph psychophysiological data acquisition system (Thought Technol-
the present study to allow for collection of a potentially more representa-
ogy, Montreal, Quebec, Canada). So as not to interfere with VLT play, the
tive sample of heart rate within each baseline phase.
STEWART, PETERSON, COLLINS, EISNOR, AND ELLERY
alcohol/kg body weight for men (1.29 mL/kg for women), mixed 1:4 parts
Post hoc tests revealed that relative to predrinking, BACs were
alcohol to cranberry juice. The dose targeted a peak BAC of 0.055%
elevated at postdrinking, t(29) ϭ 24.83, p Ͻ .01, 2 ϭ .955, and
(Stewart et al., 2005). Placebo drinks (cranberry juice only) were matched
post-VLT play, t(29) ϭ 31.29, p Ͻ .01, 2 ϭ .971. BACs at
for volume with the alcohol drinks. To provide taste and smell cues of
postdrinking and post-VLT play also differed, t(29) ϭ 2.71, p Ͻ
alcohol for the placebo participants, we spread a small amount of vodka
.05, 2 ϭ .140, with BACs falling slightly between the postdrink-
around the rim of each glass and a few drops of vodka were placed on thetop surface of each drink (cf. MacDonald, Stewart, Hutson, Rhyno, &
ing assessment and the assessment following the completion of
Loughlin, 2001). No additional visual cues were provided, as recom-
VLT play. These results suggested that the experimental procedure
mended by Ross and Pihl (1989), to avoid excessive experimental demand
was quite successful in targeting the desired BAC of 0.055% at
characteristics. As in Stewart et al. (2005), beverages were consumed
postdrinking, and at keeping this BAC elevated close to the target
steadily over 20 –25 min, depending on volume. Participants then rested for
20 –25 min to permit alcohol absorption. A postdrinking baseline heart rate
A 2 ϫ 2 ϫ 2 (Gambler Group ϫ Beverage Condition ϫ Testing
was continuously recorded for 5 min (see Footnote 3). Participants thenprovided a postdrinking BAC reading and were asked to rate their subjec-
Time) mixed-model ANOVA was conducted on VAS scores at
tive level of intoxication on the VAS scale.
postdrinking and post-VLT play. Again, gambler group was in-
Participants were invited to use their own money to play the spinning
cluded as a variable to ensure that groups did not differ in subjec-
reels game on one of two VLTs for up to 15 min.4 They were informed that
tive intoxication levels. The ANOVA revealed only a testing time
the odds of winning or losing were exactly the same as on any machine
main effect, F(1, 56) ϭ 24.91, p Ͻ .01, 2 ϭ .948 (M ϭ 31.80,
they had played on previously in the province. They were told that they
SD ϭ 23.31, vs. M ϭ 22.47, SD ϭ 19.22, for postdrinking and
could gamble as little or as much money as they wanted (up to a maximum
post-VLT play assessment times, respectively). The fact that there
of the $80, which they had been provided at the onset of the study). Thismaximum was set to ensure that participants did not spend money out of
were no beverage-condition effects on VAS scores supports the
their own pockets to play the VLTs in the lab. Participants were informed
supposition that the placebo manipulation was successful. Further-
that they would not be reimbursed for any money they lost while gambling.
more, although subjective intoxication scores decreased somewhat
Similarly, they were informed that they could keep or continue to play with
from postdrinking to post-VLT play, t tests indicated that average
any winnings.5 Heart rate was continuously recorded during this time.
subjective intoxication was Ͼ0 at both testing points, t(59) ϭ
Consistent with Stewart et al. (2005), 30 min after the beginning of the
10.57, p Ͻ .01, 2 ϭ .654, and t(59) ϭ 9.06, p Ͻ .01, 2 ϭ .582,
VLT play session, participants provided a post-VLT play BAC reading and
completed a second VAS subjective intoxication measure. Smoking wasnot permitted during testing. Participants were debriefed about their bev-
We conducted a 2 ϫ 2 ϫ 3 (Gambler Group ϫ Beverage
erage condition status, including an explanation to placebo participants as
Condition ϫ Testing Time) mixed-model ANOVA on heart rate at
to the nature and necessity of the placebo deception (cf. MacDonald et al.,
the predrinking and postdrinking baseline measurement periods
2001). If a participant was in the placebo condition, any winnings were
and during VLT play. A testing time effect, F(2, 112) ϭ 4.76, p ϭ
paid out and he or she was sent home. Alcohol participants remained until
.01, 2 ϭ .078, emerged, along with the predicted Beverage
BAC reached 0.04%. Taxi chits were available for transportation home if
Condition ϫ Testing Time interaction, F(2, 112) ϭ 3.92, p Ͻ .05,
a ride had not been previously arranged.
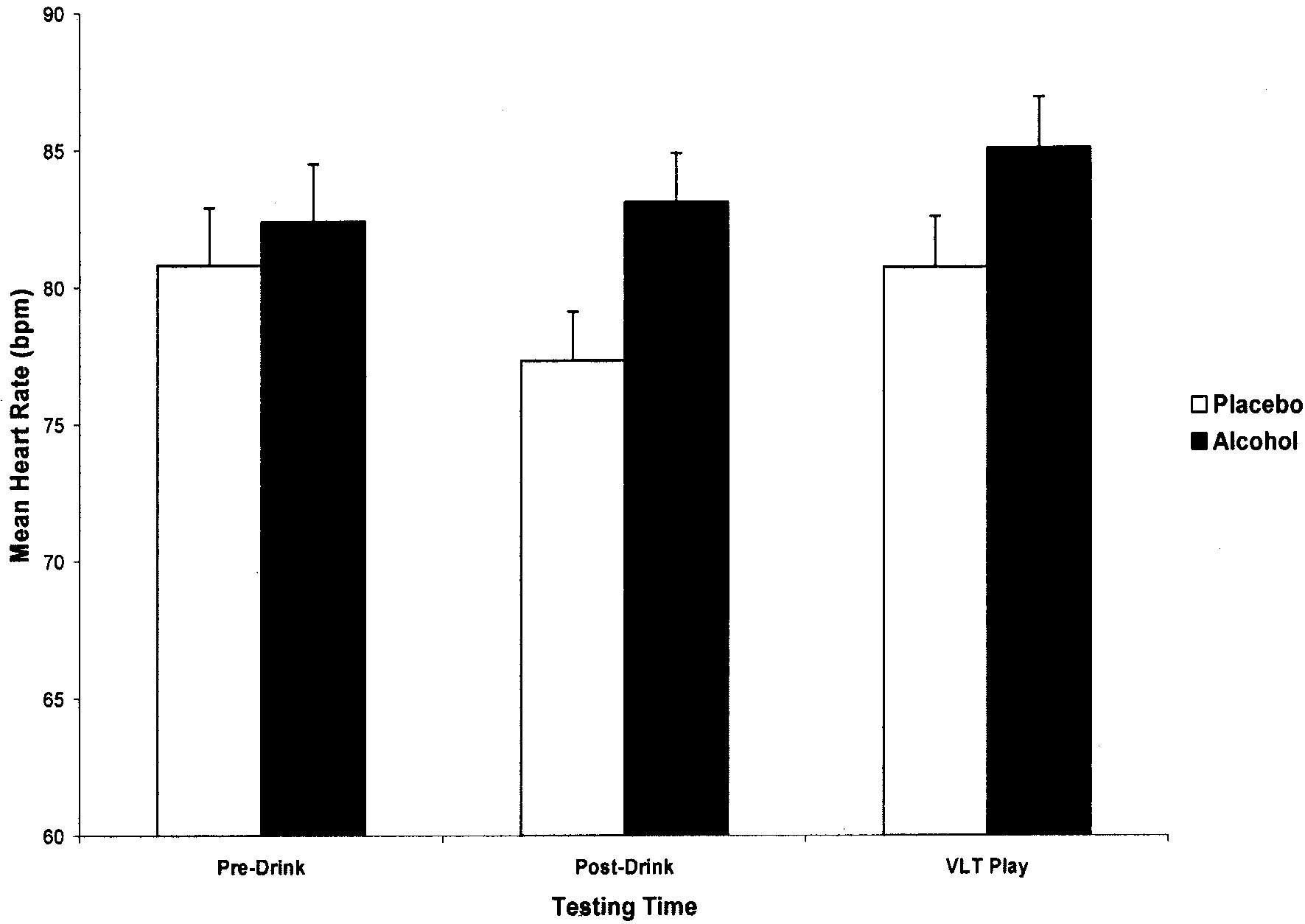
2 ϭ .065. Means and standard deviations for the hypothesizedBeverage Condition ϫ Testing Time interaction are illustrated in
Figure 1. No other effects were revealed. In particular, the ex-pected three-way interaction was nonsignificant, F(2, 112) ϭ 1.21,
Demographic characteristics and addictive behavior measure
ns, 2 ϭ .021, providing no evidence for our hypothesis that
scores were examined in a set of 2 ϫ 2 (Beverage Condition ϫGambler Group) analyses of variance (ANOVAs) and chi-square
heart-rate increases to alcohol, VLT play, and their combination
(2) analyses to ensure that random assignment to beverage con-
dition was effective in balancing groups on potentially confound-ing variables. Analyses revealed no significant main or interactiveeffect of beverage condition and gambler group on age, gender,marital status, educational history, annual income, years playingVLTs, or number of drinks per week. As expected, a significantmain effect of gambler group was found for SOGS total score, with
4 The length of the VLT play session and associated heart-rate recording
those in the PPG group scoring significantly higher than those in
interval was decreased from 30 min in our original study to 15 min in the
the NPG group (Ms ϭ 8.8 vs. 1.6, respectively): F(3, 56) ϭ
present study for several reasons. First, we felt a shorter heart rate record-
150.43, p Ͻ .01. No other significant effects were revealed. Table
ing interval would be more comparable to the 5 min intervals used at the
1 contains means and standard deviations on demographic and
two baseline phases (see Footnote 3). Second, when offered the opportu-
addictive behavior variables as a function of Gambler Group ϫ
nity to play for up to 30 min in our previous study (Stewart et al., 2005),only half of the regular gambler participants chose to play for the full
allotted time (range ϭ 18 –30 min). To maintain ecological validity, we
A 2 ϫ 3 (Gambler Group ϫ Testing Time) mixed-model
still allowed participants to self-select length of VLT play but shortened the
ANOVA was performed on alcohol condition participants’ BACs.
maximal interval to 15 min to reduce variability in length of the VLT play
Gambler group was included as a factor to ensure that the groups
section. All but 2 of our 60 participants chose to play for the full 15 min
did not differ in objective intoxication levels. The ANOVA re-
vealed only a testing time effect, F(2, 56) ϭ 510.04, p Ͻ .01, 2 ϭ
5 Although participants were informed at study outset that large wins
.948 (predrinking, M ϭ .000%, SD ϭ .000; postdrinking, M ϭ
(e.g., more than $250) would be paid via check rather than cash, no such
.056%, SD ϭ .012; and post-VLT play, M ϭ .051%, SD ϭ .009).
large wins occurred during the course of the study.
Table 1Means and Standard Deviations on Demographic and Addictive Behavior Variables as aFunction of Beverage Condition and Gambler Group
Placebo (n ϭ 15) Alcohol (n ϭ 15) Placebo (n ϭ 15) Alcohol (n ϭ 15)
NPG ϭ nonpathological gamblers; PPG ϭ probable pathological gamblers; SOGS ϭ South Oaks
Gambling Screen; VLT ϭ video lottery terminal.
The significant two-way interaction was followed up with sim-
higher than at postdrinking baseline, t(29) ϭ 3.05, p Ͻ .01, 2 ϭ
ple effects analyses and post hoc tests6 to test the three specific
.243. However, inconsistent with expectation, in the placebo
hypotheses regarding the effects of alcohol, VLT play, and their
group, heart rates at VLT play were not higher than at predrinking
combination on heart rate. Analyses of the simple effects of
baseline, t(29) ϭ 0.54, ns, 2 ϭ .010. For alcohol-condition
beverage condition at each testing time revealed that alcohol-
participants, contrary to the hypothesis involving alcohol-induced
condition participants displayed elevated heart rates, relative to
heart rate increases, post hoc tests indicated that heart rates were
placebo participants, at postdrinking, F(1, 58) ϭ 5.22, p Ͻ .05,
not elevated at post relative to predrinking, t(29) ϭ Ϫ0.61, ns,
2 ϭ .083, and during VLT play, F(1, 58) ϭ 4.14, p Ͻ .05, 2 ϭ
2 ϭ .013. However, consistent with the hypothesis involving
.067, but not at the predrinking baseline, F(1, 58) ϭ 0.28, ns, 2 ϭ
VLT play-induced heart-rate increases, in the alcohol condition,
.005, consistent with our hypotheses of heart-rate increases to
heart rate was elevated at VLT play relative to both predrinking,
alcohol alone, and to the combination of alcohol intake and VLT
t(29) ϭ 2.80, p Ͻ .01, 2 ϭ .213, and postdrinking, t(29) ϭ 2.03,
play, respectively. Although significant simple effects of testing
p Ͻ .05, 2 ϭ .125, baselines.
time were revealed both in the alcohol, F(2, 58) ϭ 3.98, p Ͻ .05,
To determine whether heart rate increases to VLT play varied by
.121, and placebo, F(2, 58) ϭ 4.74, p Ͻ .05, 2 ϭ .140,
beverage condition (i.e., to further test the hypothesis that heart
conditions, the pattern of heart-rate changes over testing timesvaried by beverage condition. For placebo participants, contrary to
rate increases to the combination of VLT play and alcohol intake
our prediction that there would be no change in heart rate follow-
would be greater than those to either activity alone), we submitted
ing placebo beverage ingestion, post hoc tests indicated that heartrates were significantly lower at postdrinking than at predrinking
6 Because this study is relatively exploratory (i.e., the first study to
baseline, t(29) ϭ Ϫ2.81, p Ͻ .01, 2 ϭ .214. As covered more
examine, within the same study, potential differences between PPGs and
extensively in the Discussion, this effect may reflect an antago-
NPGs in their relative sensitivity to heart-rate increases to alcohol, VLT
nistic placebo response that can occur when the participant is
play, and their combination), we made an a priori decision not to adjust ␣
expecting but does not receive alcohol (see Newlin, 1985). Par-
levels in our post hoc tests to maximize our chances of observing the
tially consistent with our expectation of heart rate increases to
hypothesized effects if they do exist. Nonetheless, as covered in the
VLT play alone, in the placebo group, heart rates at VLT play were
Discussion, this decision increases the probability of Type I error.
STEWART, PETERSON, COLLINS, EISNOR, AND ELLERY
Mean heart rate in beats per minute (bpm) as a function of beverage condition and testing time.
VLT ϭ video lottery terminal. Error bars represent standard deviations.
heart rate change scores (i.e., heart rate at VLT play minus heart
regular gamblers identified as PPGs would show greater heart-rate
rate at predrinking baseline) to a 2 ϫ 2 (Gambler Group ϫ
increases in response to alcohol and/or gambling. We hypothesized
Beverage Condition) between-subjects ANOVA. The analysis re-
that alcohol would lead to increases in heart rate relative to both
vealed only a beverage condition effect, F(1, 56) ϭ 4.55, p Ͻ .05,
heart rate at the predrinking baseline and heart rate in the group
2 ϭ .075. As hypothesized, alcohol participants showed a greater
administered placebo. We also hypothesized that VLT play would
magnitude heart-rate increase to VLT play than did placebo con-
increase heart rate relative to pre- and postdrinking baselines even
trols (M ϭ 2.99 bpm, SD ϭ 5.85, vs. M ϭ Ϫ0.75 bpm, SD ϭ 7.62,
among those consuming placebo and that the combination of VLT
respectively). Again, the predicted Beverage Condition ϫ Gam-
play and alcohol intake would result in further heart rate increases
bler Group interaction was nonsignificant, F(1, 56) ϭ 2.01, ns,
relative to either activity alone. Finally, we hypothesized that the
2 ϭ .035, providing no evidence that heart-rate increases to the
above effects would prove stronger among PPGs relative to NPGs.
combination of VLT play and alcohol intake would be greater
In the current study we were able to partially replicate Stewart
et al. (2005) with respect to the effects of alcohol. Previousresearch shows that alcohol consumption increases heart rate rel-
ative to placebo (cf. Peterson et al., 1993, 1996; Stewart et al.,
The present study was designed to investigate the existence of a
1992) and we expected to see heart rate elevations in those ad-
potential common reward mechanism that may underlie the rein-
ministered alcohol relative to those administered placebo in the
forcing effects of drinking and gambling behavior among regular
present study at postdrinking baseline. This hypothesis was sup-
VLT players. In effect, we set out to replicate and extend our
ported in that participants in the alcohol condition displayed ele-
earlier study on this issue (i.e., Stewart et al., 2005) by investigat-
vated heart rate relative to participants in the placebo condition at
ing heart-rate responses to a moderately intoxicating dose of
postdrinking but not at the predrinking baseline.
alcohol, to VLT play, and to their combination, among a sample of
We were also able to partially replicate Stewart et al. (2005)
regular VLT players, half of whom were given alcohol and half of
with respect to the effects of VLT play, extending our previous
whom received a mix-only control beverage. The two main
findings of heart rate increase with a video poker game to the more
changes from our original study were the use of a placebo bever-
popular type of spinning reels VLT game. All players, regardless
age to control for expectancy effects in the present study and the
of beverage condition, showed elevated heart rates at VLT play,
use of a larger sample size that allowed us to investigate whether
relative to postdrinking baseline. However, heart rates were ele-
vated during VLT play relative to predrinking baseline only among
susceptible to heart rate increases to gambling (and/or alcohol)
those administered alcohol, suggesting that the effects of gambling
because of their high-risk status, washing out any between-groups
on heart rate interacted with beverage condition. We examined this
differences. A second explanation pertains to the measurement
interactive effect of drinking and VLT play more directly by
instrument used in the present study (i.e., the original SOGS;
comparing the degree of increase from predrinking baseline to
Lesieur & Blume, 1987). Given problems recently identified with
VLT play in each beverage condition in a supplementary set of
the original SOGS as a measure of gambling problems (Strong,
statistical analyses. As hypothesized, and consistent with our ear-
Lesieur, Breen, & Stinchfield, 2004), future research should use an
lier study (Stewart et al., 2005), we did see that the degree of
alternative method for identifying PPGs (e.g., Canadian Problem
increase from predrinking to VLT play was greater for those in the
Gambling Index, Ferris & Wynne, 2001; DSM–IV-based question-
alcohol condition. Thus, the combination of VLT play and alcohol
naire, Beaudoin & Cox, 1999) to ensure that our null findings are
consumption does appear to be linked to an additional heart-rate
not due to measurement problems. Third, given recent research on
increase, compared with the heart rate increase associated with
the validity of subtyping gamblers (e.g., Blaszczynski & Nower,
engaging in either addictive behavior alone, which may help
2002; Stewart, Wall, Loba, Stuart, & Ellery, 2004), it is possible
explain the frequent pairing of these two activities in both clinical
that certain subtypes of gamblers might be more or less sensitive
and nonclinical populations (Focal Research, 1998; Stewart &
to the heart rate effects of gambling and alcohol. In future research
Kushner, 2003; Stewart et al., 2002).
it would be interesting to determine whether enhancement-
Although most aspects of our original study (Stewart et al.,
motivated gamblers (a subtype who self-report gambling specifi-
2005) were replicated, there were some important differences as
cally to increase positive affect; Stewart et al., 2004) or impulsive
well. For example, contrary to hypothesis, alcohol participants
gamblers (a subtype with difficulties regulating behavior in the
showed no significant increase in heart rate from pre- to postdrink-
presence of cues for reward; Blaszczynski & Nower, 2002) show
ing baselines. This was surprising given that several studies (e.g.,
increased sensitivity to the positively reinforcing effects of gam-
Stewart et al., 1992, 2005) have shown that alcohol increases heart
bling (and/or alcohol) indexed by degree of heart rate response to
rate from resting baseline. We also found placebo participants
these addictive activities, relative to other gambler subtypes.
actually had higher heart rates at predrinking than at postdrinking
Fourth, the findings may indeed be valid in that there may be no
baseline. It appears most likely that this was a consequence of a
greater sensitivity to heart rate increases among PPGs. In fact, a
conditioned compensatory response. Newlin (1985) found an au-
similar lack of relation between heart rate response to gambling
tonomic response in placebo-condition participants that was op-
and severity of pathological gambling has been observed in pre-
posite in direction to the effects of alcohol among a sample of male
vious studies (e.g., Diskin & Hodgins, 2003; Meyer et al., 2000).
social drinkers. In effect, the cues associated with drinking alcohol
Finally, it is possible that the combination of VLT play and alcohol
(e.g., bar setting, smell of vodka) may have elicited a conditioned
intake might be particularly addicting to potential alcoholics who
compensatory response, causing heart rate to decrease in anticipa-
gamble (and therefore show an exceptionally enhanced heart rate
tion of receiving the beverage, resulting in heart rate deceleration
in the combined condition), rather than to potential problem gam-
in the placebo-condition participants from the pre- to the post-
drinking baseline. This conditioned compensatory response was
Several potential limitations to the current study should be
presumably not operative in our last study because we used a
noted. One possible limitation pertains to the heart rate recording
control beverage rather than a placebo beverage in the latter
equipment used. We used a photoplethysmograph attached to a
(Stewart et al., 2005). This explanation could also be used to
finger on the nondominant hand to collect IBI data that were later
account for the lack of change between pre- and postdrinking
converted to bpm values. Although some would argue that a more
baselines in the alcohol group in the present study. Specifically, a
appropriate method for heart rate recording would be through the
conditioned compensatory heart rate deceleration in the alcohol-
use of an electrocardiogram and electrodes placed on the chest
condition participants could have countered the expected stimulant
(e.g., Stewart et al., 1992), others have argued for the value of IBI
effects of alcohol, resulting in no net change from pre- to post-
measurements in studies on heart rate (e.g., Heslegrave, Ogilvie, &
drinking baseline in this beverage condition.
Furedy, 1979). Another possible limitation pertains to the possi-
Contrary to hypothesis, the present study also found no effects
bility that heart rate measures may have been influenced by minor
of gambler group on degree of heart rate response to gambling,
movement artifact, particularly during the VLT play phase, which
drinking, or their combination. The failure to observe between-
involved some small degree of movement. Nonetheless, studies
groups differences in heart rate increases to these addictive activ-
that have included a movement baseline control condition have
ities was not secondary to differences in heart rate at the predrink-
showed that heart rate increases to gambling are larger than those
ing resting baseline. This latter finding is in contrast to predictions
caused by the minimal movement involved in gambling activity
that would be made on the basis of Jacobs’s (1986) general theory
(Coventry & Norman, 1997) making this possible explanation of
of addictions in which he postulates that abnormalities in physio-
our findings unlikely. A further possible limitation was the rela-
logical resting state predispose people to persistent, uncontrolled
tively small sample size per group in the 2 ϫ 2 (Gambler Group ϫ
behavioral patterns involving both drinking and gambling. The
Beverage Condition) between-subjects design that may have pre-
failure to find the hypothesized gambler group differences in heart
cluded observation of the predicted interaction between these
rate reactivity to gambling, alcohol, or their combination could be
variables on heart rate. Nonetheless, observation of effect sizes
involved in the predicted interactions involving the gambler status
First, our control group consisted of regular gamblers who were
variable indicate that low power is unlikely to explain the absence
not preselected into groups at high or low risk for gambling
of differences in heart rate reactivity across the PPG versus NPG
problems. Thus, some of those in the control group may have been
groups. We should also caution that our choice not to adjust ␣ in
STEWART, PETERSON, COLLINS, EISNOR, AND ELLERY
our post hoc tests (see Footnote 6) may have resulted in an
imental approach to individual vulnerability to psychostimulant addic-
increased probability of Type I errors. Finally, the present inves-
tion. Neuroscience and Biobehavioral Review, 13, 141–147.
tigation was an analogue study that carries with it the usual
Diskin, K. M., & Hodgins, D. C. (2003). Psychophysiological and subjec-
tive arousal during gambling in pathological and non-pathological video
The present findings are consistent with the possibility that
lottery gamblers. International Gambling Studies, 3, 37–51.
Diskin, K. M., Hodgins, D. C., & Skitch, S. A. (2003). Psychophysiolog-
alcohol consumption and VLT gambling are associated with heart
ical and subjective responses of a community sample of video lottery
rate increases that might reflect activity of the incentive reward
gamblers in gambling venues and laboratory situations. International
system (Peterson et al., 1993). If future research were to establish
Gambling Studies, 3, 133–147.
the involvement of the dopamine reward system in the heart rate
Ellery, M., Stewart, S. H., & Loba, P. (2005). Alcohol’s effects on
response to these two addictive activities, the drug naltrexone (an
risk-taking during video lottery terminal (VLT) play among probable
opiate antagonist that inhibits dopamine release in the nucleus
pathological and non-pathological gamblers. Journal of Gambling Stud-
accumbens, O’Malley, 1996 and that reduces alcohol consumption
by making alcohol ingestion less pleasurable and rewarding, Gi-
Ferris, J., & Wynne, H. (2001). Canadian problem gambling index: Final
anoulakis, 1996) might prove useful in treating those with comor-
report. Toronto, Ontario, Canada: Centre for Addiction and Mental
bid alcohol and gambling disorders. It would be interesting to
replicate and extend the present study, with the addition of a
Focal Research. (1998). Nova Scotia Video Lottery Players’ Survey 1997/
naltrexone versus pill placebo manipulation (cf. Peterson et al., in
98. Halifax, Nova Scotia, Canada: Nova Scotia Department of Health,Problem Gambling Services.
press) to determine whether this drug would block the observed
Fowles, D. C. (1980). The three arousal model: Implications of Gray’s
heart-rate increases to alcohol, VLT play, and their combination
two-factor learning theory for heart rate electrodermal activity and
among regular gamblers. Additional research is also needed to
psychopathy. Psychophysiology, 17, 87–104.
identify which gamblers are most susceptible to heart rate in-
Fowles, D. C., Fisher, A. E., & Tranel, D. T. (1982). The heart beats to
creases to alcohol, gambling, and their combination, to allow for
reward: The effect of monetary incentive on heart-rate. Psychophysiol-
improvements in matching of treatment and prevention strategies
to those most likely to benefit (e.g., Conrod et al., 2000).
Gianoulakis, C. (1996). Implications of endogenous opioids and dopamine
in alcoholism: Human and basic science studies. Alcohol and Alcohol-ism, 31, 33– 42.
Grant, J., Kushner, M. G., & Kim, S. W. (2002). Pathological gambling and
alcohol use disorder. Alcohol Research and Health, 26, 143–150.
Beaudoin, C. M., & Cox, B. J. (1999). Characteristics of problem gambling
Gray, J. A. (1982). The neuropsychology of anxiety: An enquiry into the
in a Canadian context: A preliminary study using a DSM–IV-based
function of the septal-hippocampal system. Oxford, England: Oxford
questionnaire. Canadian Journal of Psychiatry, 44, 483– 487.
Blackburn, J. R., Pfaus, J. G., & Phillips, A. G. (1992). Dopamine func-
Griffiths, M. D. (1991). Psychobiology of the near-miss in fruit machine
tions in appetitive and defensive behaviors. Progress in Neurobiology,
gambling. Journal of Psychology: Interdisciplinary and Applied, 125,
Blaszczynski, A., & Nower, L. (2002). A pathways model of problem and
pathological gambling. Addiction, 97, 487– 499.
Griffiths, M. D. (1993). Tolerance in gambling: An objective measure
Boileau, I., Assaad, J. M., Pihl, R. O., Benkelfat, C., Leyton, M., Diksic,
using the psychophysiological analysis of male fruit machine gamblers.
M., et al. (2003). Alcohol promotes dopamine release in the human
Addictive Behaviors, 18, 365–372.
nucleus accumbens. Synapse, 49, 226 –231.
Heslegrave, R. J., Ogilvie, J. C., & Furedy, J. L. (1979). Measuring
Brunelle, C., Assaad, J. M., Pihl, R. O., Tremblay, R. E., & Vitaro, F.
baseline-treatment differences in heart rate variability: Variance versus
(2003). Exaggerated ethanol-induced cardiac reactivity as an indicator of
successive difference mean square and beats per minute versus interbeat
increased risk for gambling. Psychology of Addictive Behaviors, 17,
intervals. Psychophysiology, 16, 151–157.
Jacobs, D. F. (1986). A general theory of addictions: A new theoretical
Comings, D. E., Rosenthal, R. J., Lesieur, H. R., Rugle, L. J., Muhleman,
model. Journal of Gambling Behavior, 2, 15–31.
D., Chiu, C., et al. (1996). A study of the dopamine D2 receptor gene in
Kalivas, P. W., & McFarland, K. (2003). Brain circuitry and the reinstate-
pathological gambling. Pharmacogenetics, 6, 223–234.
ment of cocaine-seeking behavior. Psychopharmacology, 168, 44 –56.
Conrod, P. J., Peterson, J. B., & Pihl, R. O. (2001). Reliability and validity
Kausch, O. (2003). Patterns of substance abuse among treatment-seeking
of alcohol-induced heart rate increase as a measure of sensitivity to the
pathological gamblers. Journal of Substance Abuse Treatment, 25, 263–
stimulant properties of alcohol. Psychopharmacology, 157, 20 –30.
Conrod, P. J., Stewart, S. H., Pihl, R. O., Coˆte´, S., Fontaine, V., & Dongier,
Ladouceur, R., Sevigny, S., Blaszczynski, A., O’Connor, K., & Lavoie,
M. (2000). Efficacy of brief coping skills interventions that match
M. E. (2003). Video lottery: Winning expectancies and arousal. Addic-
different personality profiles of female substance abusers. Psychology ofAddictive Behaviors, 14, 231–242.
Leary, K., & Dickerson, M. (1985). Levels of arousal in high- and low-
Coventry, K. R., & Hudson, J. (2001). Gender differences, physiological
frequency gamblers. Behaviour Research and Therapy, 23, 635– 640.
arousal and the role of winning in fruit machine gamblers. Addiction, 96,
Lesieur, H. R., & Blume, S. B. (1987). The South Oaks Gambling Screen
(SOGS): A new instrument for the identification of pathological gam-
Coventry, K. R., & Norman, A. C. (1997). Arousal, sensation seeking and
blers. American Journal of Psychiatry, 144, 1184 –1188.
frequency of gambling in off-course horse racing bettors. British Journal
Lin, D., Bruijnzeel, A. W., Schmidt, P., & Markou, A. (2002). Exposure to
of Psychology, 88, 671– 681.
chronic mild stress alters thresholds for lateral hypothalamic stimulation
Crockford, D. N., & el-Guebaly, N. (1998). Psychiatric comorbidity in
reward and subsequent responsiveness to amphetamine. Neuroscience,
pathological gambling: A critical review. Canadian Journal of Psychi-
MacDonald, A. B., Stewart, S. H., Hutson, R., Rhyno, E., & Loughlin,
Deminiere, J. M., Piazza, P. V., LeMoal, M., & Simon, H. (1989). Exper-
H. L. (2001). The roles of alcohol and alcohol expectancy in the
dampening of responses to hyperventilation among high anxiety sensi-
gambling and alcohol dependence in men. Archives of General Psychi-
tive young adults. Addictive Behaviors, 26, 841– 867.
McBride, W. J., Murphy, J. M., Lumeng, L., & Li, T. K. (1990). Serotonin,
Stewart, S. H., Blackburn, J. R., & Klein, R. M. (2000). Against the odds:
dopamine, and GABA involvement in alcohol drinking of selectively
Establishment of a video lottery terminal research laboratory in a natu-
bred rats. Alcohol, 7, 199 –205.
ralistic setting. The Nova Scotia Psychologist, Spring, 3– 6.
Meyer, G., Hauffa, B. P., Schedlowski, M., Pawlak, C., Stadler, M. A., &
Stewart, S. H., Collins, P., Blackburn, J. R., Ellery, M., & Klein, R. (2005).
Exton, M. S. (2000). Casino gambling increases heart rate and salivary
Heart rate increase to alcohol administration and video lottery terminal
cortisol in regular gamblers. Society of Biological Psychiatry, 48, 948 –
(VLT) play among regular VLT players. Psychology of Addictive Be-
Newlin, D. B. (1985). The antagonistic placebo response to alcohol cues.
Stewart, S. H., Finn, P. R., & Pihl, R. O. (1992). The effects of alcohol on
Alcoholism: Clinical and Experimental Research, 9, 411– 416.
the cardiovascular stress response in men at high risk for alcoholism: A
O’Malley, S. S. (1996). Opioid antagonists in the treatment of alcohol
dose-response study. Journal of Studies on Alcohol, 53, 499 –506.
dependence: Clinical efficacy and prevention of relapse. Alcohol and
Stewart, S. H., & Kushner, M. G. (2003). Recent research on the co-
morbidity of alcoholism and pathological gambling. Alcoholism: Clini-
Panksepp, J. (1999). Affective neuroscience: The foundations of human andcal and Experimental Research, 27, 285–291. animal emotions. New York: Oxford University Press.
Stewart, S. H., McWilliams, L. A., Blackburn, J. R., & Klein, R. (2002). A
Peterson, J. B., Conrod, P., Vassileva, J., Gianoulakis, C., & Pihl, R. O. (in
laboratory-based investigation of the influence of video lottery terminal
press). Differential effects of naltrexone on cardiac, subjective, and
(VLT) play on mood and alcohol consumption among regular VLT
behavioural reactions to acute ethanol-intoxication. Journal of Psychi-
players. Addictive Behaviors, 27, 819 – 835.
Stewart, S. H., Wall, A.-M., Loba, P., Stuart, S., & Ellery, M. (2004, May).
Peterson, J. B., Pihl, R. O., Gianoulakis, C., Conrod, P., Finn, P. R.,
Subtypes of gamblers identified on the basis of gambling motives differ
Stewart, S. H., et al. (1996). Ethanol-induced change in cardiac and
in gambling outcome expectancies. Paper presented at the 3rd Annual
endogenous opiate function and risk for alcoholism. Alcoholism: Clini-
Alberta Conference on Gambling Research, Banff, Alberta, Canada. cal and Experimental Research, 20, 1542–1552.
Strong, D. R., Lesieur, H. R., Breen, R. B., & Stinchfield, R. (2004). Using
Peterson, J. B., Pihl, R. O., Seguin, J. R., Finn, P. R., & Stewart, S. H.
a Rasch model to examine the utility of the South Oaks Gambling Screen
(1993). Heart rate reactivity and alcohol consumption among sons of
across clinical and community samples. Addictive Behaviors, 29, 465–
male alcoholics and sons of non-alcoholics. Journal of Psychiatry andNeuroscience, 18, 190 –198.
Wise, R. A. (1988). Psychomotor stimulant properties of addictive drugs.
Pokorny, A. D., Miller, B. A., & Kaplan, H. B. (1972). The Brief MAST:
In P. W. Kalivas & C. B. Nemeroff (Eds.), Annals of the New York
A shortened version of the Michigan Alcoholism Screening Test. Amer-Academy of Sciences: Vol. 537, The mesocorticolimbic dopamine systemican Journal of Psychiatry, 129, 342–345.
(pp. 228 –234). New York: New York Academy of Sciences.
Potenza, M. N. (2001). The neurobiology of pathological gambling. Sem-
Wright, R. A., Killebrew, K., & Pimpalapure, D. (2002). Cardiovascular
inars in Clinical Neuropsychiatry, 6, 217–226.
incentive effects where a challenge is unfixed: Demonstrations involving
Robins, L. N., Locke, B. A., & Regier, D. A. (1991). An overview of
social evaluation, evaluator status and monetary reward. Psychophysi-
psychiatric disorders in America. In L. N. Robins & D. A. Regier (Eds.),
Psychiatric disorders in America: The epidemiologic catchment area
Zack, M., & Poulos, C. X. (2004). Amphetamine primes motivation to
study (pp. 53– 81). New York: Free Press.
gamble and gambling-related semantic networks in problem gamblers.
Ross, D. F., & Pihl, R. O. (1989). Modification of the balanced-placebo
Neuropsychopharmacology, 29, 195–207.
design for use at high blood alcohol levels. Addictive Behaviors, 14,91–97.
Slutske, W. S., Eisen, S., True, W. R., Lyons, M. J., Goldberg, J., &
Tsuang, M. (2000). Common genetic vulnerability for pathological
 STEWART, PETERSON, COLLINS, EISNOR, AND ELLERY
Mean heart rate in beats per minute (bpm) as a function of beverage condition and testing time.
STEWART, PETERSON, COLLINS, EISNOR, AND ELLERY
Mean heart rate in beats per minute (bpm) as a function of beverage condition and testing time.