Anaphylaxis to isosulfan blue and cross-reactivity to patent blue v
Case report Anaphylaxis to isosulfan blue and cross- reactivity to patent blue V: case report and review of the nomenclature of vital blue dyes Kathrin Scherer, MD*; Wolfgang Studer, MD†; Verena Figueiredo‡; and Andreas J. Bircher, MD* Background: Blue dyes used for lymphatic mapping in sentinel lymph node biopsy cause intraoperative anaphylactic
reactions in up to 2.7% of patients. With increasing implementation of this technique, the incidence of anaphylaxis to these dyescan be expected to increase. In the literature, the chemically often unrelated and inconsistently designated dyes have beenconfused, adding to other inconsistencies in the nomenclature. Objective: To demonstrate the nomenclature, chemical and physiologic differences, and allergenicity of the various blue dyes Methods: We describe a patient with an intraoperative grade IV anaphylactic reaction to isosulfan blue. Immediate-type
hypersensitivity was proved by positive skin test reactions and CD63 expression to isosulfan blue and cross-reactivity to patentblue V. Results: A review of the literature clarified the exact nomenclature of the blue dyes and the possible pitfalls of confusing
nomenclature in the context of structurally closely related dyes with different allergenic properties. For the detection of type Ihypersensitivity, intracutaneous tests are valuable tools. An IgE-mediated mechanism has been shown recently. In most cases,sensitization exists without known previous exposure in a medical context. This may be due to the widespread use of such dyesin objects of everyday life. Preoperative antiallergic medication use does not prevent anaphylactic reactions but apparentlyreduces their severity. Conclusion: For better comparison and precision, the Chemical Abstracts Service number of the respective dye should always Ann Allergy Asthma Immunol. 2006;96:497–500. INTRODUCTION
laxants and opiates, may cause anaphylactoid reactions owing
Anaphylactic and anaphylactoid reactions are rare events during
to their strong histamine-liberating capacity, in addition to the
anesthesia, although the true incidence of anaphylactic reactions
possibility of an IgE-mediated reaction. Skin tests, which are
and their morbidity and mortality remain poorly defined. These
usually a valuable diagnostic tool, may yield misleading
reactions may lead to death, even when appropriately treated,
results owing to uncertainties in distinguishing irritant from
with a mortality of 3.5% to 4.7%. Incidence rates are known to
allergic skin reactions. Blue dyes, used for lymphatic map-
be 0.5 to 1 in 10,000 (in Australia in 1993) to 1 in 13,000 (in
ping in the context of sentinel lymph node biopsy (SLNB) in
France in 1996)1,2 in countries with well-organized documenta-
cancer surgery, are rare causes of anaphylactic reactions.
tion systems. Of the drugs most liable for inducing anaphylac-
Because of the increasing implementation of this technique
toid or anaphylactic reactions during anesthesia, myorelaxants
for new indications, eg, melanoma, breast carcinoma, bladder
account for approximately 50%,3 followed by latex sensitization
cancer, and cervical and endometrial cancer, the incidence of
anaphylaxis to these blue dyes can be expected to increase.
Allergologic diagnostic approaches to these events are
By means of this case report of intraoperative anaphylaxis
challenging for multiple reasons.4 Usually more than 1 pos-
to isosulfan blue and an overview of the literature, we attempt
sible elicitor of anaphylaxis has been administered at the
to draw attention to this increasingly important group of dyes
same time. Some of the drugs in question, especially myore-
and its potential to cause intraoperative anaphylaxis. In ad-dition, often these dyes are not correctly designated, and evenfrom a chemical point of view misleading designations have
* Allergy Unit, Department of Dermatology, University Hospital, Basel,
been used, resulting in a mix up of the dyes in the literature.
Switzerland. † Department of Anesthesia, Kantonsspital, Liestal, Switzerland. CASE REPORT
‡ Institute of Hospital Pharmacy, University Hospital, Basel, Switzerland.
A 70-year-old woman was scheduled to undergo a lumpec-
Received for publication March 18, 2005. Accepted for publication in revised form July 26, 2005.
tomy of the left breast and SLNB for suspected breast cancer.
Hypertension was treated with enalapril. After the smooth
Both dyes were injected in the upper back at 1:10 and 1:100
induction of general anesthesia, the patient developed, shortly
dilutions. After 15 minutes, the resulting wheals were docu-
after the start of surgery, generalized erythema, tachycardia,
mented using a digital camera (Coolpix 5000; Nikon USA,
a decline in blood pressure to 80/50 mm Hg, and conjuncti-
Melville, NY) through an optical device with an integrated
vitis. After the administration of vasoactive substances and
scale. The wheal circumference was determined in triplicate,
glucocorticosteroids and substitution of volume, her circula-
and the area was then calculated using the freeware NIH
tion returned to a stable condition and her shock symptoms
Image/J software V 1.3Ø win32 (National Institutes of
regressed. The postoperative course was uneventful.
Health). By statistical analysis, compared with a negative
At the time of the anaphylactic reaction the patient had
control (0.9% sodium chloride), a threshold dilution for in-
previously received propofol, enflurane, and thiopental so-
tracutaneous tests of 1:100 of the stock solution for isosulfan
dium, as well as the muscle relaxant atracurium besylate for
blue and patent blue V was established, separating toxic-
the induction of anesthesia and cefazolin sodium (a first-
irritant reactions from true allergic reactions.
generation cephalosporin) as a prophylactic antibiotic. Mast
Specific IgE to isosulfan blue and patent blue V could not
cell tryptase levels were elevated immediately after the inci-
be detected using either ImmunoCAP (isosulfan blue) or
dent to 113 g/L (reference range, 1–13.5 g/L), indicating
radioallergosorbent test (patent blue V) techniques (Pharma-
an allergic reaction. At that point, an anaphylactic reaction
cia, Uppsala, Sweden). Investigation of specific IgE to iso-
grade IV to cefazolin, atracurium, thiopental, or latex was
sulfan blue using an enzyme-linked immunosorbent assay
according to a recent publication5 was also negative. Results
Results of skin prick and intracutaneous tests with propo-
of sulfidoleukotriene release tests (CAST, Bu¨hlmann Inc,
fol, thiopental, atracurium, benzylpenicillin, amoxicillin, and
Allschwil, Switzerland) were negative; however, CD63 ex-
cefazolin in several concentrations; skin prick tests with
pression (Flow-CAST Basophil Activation Test, Bu¨hlmann
latex-protein derivatives; and determination of specific IgE
Inc) was positive for both substances. Therefore, the final
against latex, penicillins, and aminopenicillins were negative.
diagnosis was an intraoperative anaphylactic reaction due to
A lymphocyte transformation test to benzylpenicillin, amoxi-
immediate-type hypersensitivity to isosulfan blue with cross-
cillin, and cefazolin did not show any stimulation. A serum
reactivity to patent blue V, possibly aggravated by enalapril.
sample from the patient was used for experimental determi-nation of specific IgE to thiopental, propofol, and cefaclor
(another first-generation cephalosporin), and the findings
The dyes commonly used for SLNB are isosulfan blue and
were negative. The basal mast cell tryptase concentration was
patent blue V, although other dyes, such as indocyanine green
elevated to 25.4 g/L, suggesting an increased mast cell
and fluorescein, have been investigated and are used in spe-
mass. However, no clinical symptoms of mastocytosis were
cial situations.5 The chemical systematics of the standard
present. The preliminary diagnosis was an anaphylactic reac-
dyes isosulfan blue and patent blue V are complicated, and
tion of unknown origin, possibly due to the suspected diag-
the situation is aggravated by a misleading nomenclature that
nosis of systemic mastocytosis. However, on repeated con-
is sometimes contradictory even in the chemical expert liter-
trols, serum mast cell tryptase levels ranged from 18 to 25
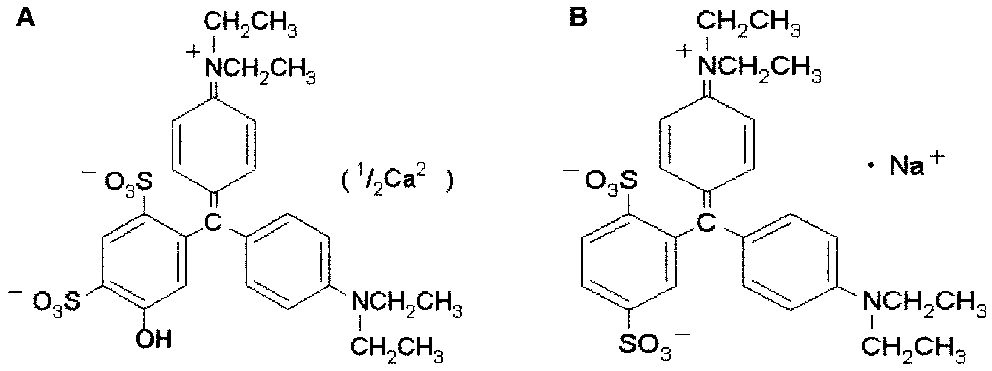
ature. Figure 1 shows the chemical structure of the 2 mole-
g/L, thereby not fulfilling the criterion for systemic masto-
cules, which differ in the position of the substituted sulfonate.
cytosis of being constantly greater than 20 g/L.
Both belong to the group of triarylmethane dyes and basically
A new careful study of the anesthesia protocol and the
share the same formula of C H N O S , with patent blue V
surgical report and repeated questioning of the anesthesiolo-
having an additional hydroxyl group.
gist revealed that immediately before the start of surgery the
The sodium salt of patent blue (Chemical Abstracts Service
patient was injected with several milliliters of isosulfan blue
[CAS] No. 129-17-9) is, among many other names, also
perilesionally as a marker for the lymphatic drainage system
called sulfan blue, food blue 3, patent blue VF, and acid blue
of the diseased tissue in preparation for the intended SLNB.
1. Isosulfan blue (CAS No. 68238-36-8) is the 2,5-disulfo-
Skin prick and intracutaneous tests were then performed
phenyl structural isomer of patent blue (not patent blue V)
with isosulfan blue and patent blue V (concentration forintracutaneous tests: 1:1 to 1:106 of stock solution [1%]) andmethylene blue (1:1 to 1:104 of stock solution [1%]). Meth-ylene blue results were negative for all the tests, whereasisosulfan blue and patent blue V results were positive up todilutions of 1:105 of the stock solution, positive being definedas a wheal larger than the negative control after 15 minutes.
Informed consent was obtained from 9 healthy individuals
who had never been exposed to isosulfan blue or patent blueV in a medical context and who served as controls for theintracutaneous tests. This testing was approved by the ethics
Figure 1. Chemical structure of patent blue V (A) and isosulfan blue
committee of the Medical Faculty of the University of Basel.
ANNALS OF ALLERGY, ASTHMA & IMMUNOLOGY
and is sold under the trade name Lymphazurine.6 Patent blue
after injection of the drug indicate as much. The cause of
V is predominantly provided as calcium-chelated dimer (CAS
biphasic reactions is not yet understood completely. Sampson
No. 3536-49-0) and can also be found under the name patent
et al15 and Lee and Greenes16 discuss in studies of children
blue violet, food blue 5, acid blue 3, and disulfine blue. It is
and adolescents a relatively long time between initial ana-
also known as E 131 and is still on the market as a food
phylaxis and the administration of epinephrine and its corre-
colorant, in contrast to the report by Quiliquini et al.7 Patent
lation with the occurrence of a second anaphylactic (biphasic)
blue V has a slightly different chemical structure containing
episode. In a study17 of 639 patients who underwent SLNB
an additional hydroxyl group at position 5.
for breast cancer using isosulfan blue, 7 anaphylactic reac-
Because of the close structural relationship of these vital
tions occurred, 2 of which were biphasic. The 2 patients had
dyes, cross-reactivity may be assumed and could be shown
recurrences during postoperative monitoring (6 and 8 hours
clinically and in the Flow-CAST in our patient. Recently,
after surgery) and again responded well to antiallergic treat-
flow cytometric quantification of CD63-positive basophils
ment.17 Quiliquini et al7 described a patient with a second
has been shown to be a useful tool in the diagnosis of type I
episode of severe anaphylaxis 3 hours after the first. In that
sensitization to patent blue V.8 For most patients, the mode of
case, patent blue V was the causative agent.
sensitization is not clear because almost all patients are ex-
Raut et al18 investigated the use of preoperative prophy-
posed only once to one of the dyes in the context of lym-
laxis with 100 mg of hydrocortisone (4 mg of dexametha-
phangiography or SLNB. Therefore, most patients have re-
sone), 50 mg of diphenhydramine, and 20 mg of famotidine
acted at their first known exposure to such a dye. An as-yet
in 448 patients with SLNB using isosulfan blue. They ob-
unproven hypothesis states that sensitization against the vital
served allergic reactions in 0.7% of these patients, all of them
dyes is facilitated by the common use of patent blue and other
grade I. No episodes of hypotension were noted. They con-
structurally closely related triarylmethane dyes in objects of
cluded that preoperative prophylaxis reduced the severity but
everyday life, such as color textiles, cosmetics, detergents,
not the overall incidence of adverse reactions to isosulfan
paints, inks, antifreeze, cold remedies, laxatives, and suppos-
blue.18 The complication rate regarding wound healing dou-
bled under this treatment, but it did not reach statistical
In addition to a variety of case reports11,12 there are several
significance. No biphasic anaphylaxis was seen with prophy-
retrospective and prospective studies of large numbers of
lactic therapy, perhaps because of the overall less severe
patients on the frequency of allergic reactions to isosulfan
reactions with prophylactic therapy. Severe reactions and
blue and patent blue V. Montgomery et al10 calculated in their
early onset after exposure to the allergen seem to be risk
meta-analysis of several single-institution series, including
their own of 2,392 patients, the incidence of allergic reactions
Several incidences have been reported of transient, false
to vital blue dyes in patients with breast cancer. For patent
lowering of pulse oximetry findings. Coleman et al19 postu-
blue, the incidence is 0.6% to 2.7%, with a mean of 1.8%. For
lated that the absorption maximum of isosulfan blue at 646
isosulfan blue, the incidence is 0.9% to 1.9%, with a mean of
nm interferes with measuring of the absorption of oxyhemo-
1.4%. The cumulative number of patients included in these
globin at 660 nm using conventional pulse oximeters, indi-
studies was 1,940 for patent blue and 4,247 for isosulfan blue.
Most of the patients reacted mildly, with anaphylactic reac-
Skin tests, especially intracutaneous tests, are valuable
tion grades I and II, with urticaria, blue hives, flush, and
tools for diagnosing type I sensitization to isosulfan blue and
pruritus; however, severe hypotensive reactions do occur.
patent blue V. We demonstrated that a 1:100 dilution of the
The reactions are generally reported to respond rapidly to
stock solution (1%) was not irritant after intracutaneous in-
jection in 9 healthy individuals. This is in analogy to studies
In our patient, the long-term use of the angiotensin-con-
by Laurie et al,20 who reported negative intradermal test
verting enzyme (ACE) inhibitor enalapril may have aggra-
results in 8 healthy individuals and 1 patient with breast
vated the situation. In a recent retrospective analysis of 1,149
cancer with 1:100 dilutions of the stock solution.
patients with anaphylaxis, Brown13 suggested that ACE in-
Woehrl et al21 recently demonstrated specific IgE antibod-
hibitors affect reaction severity, although it was not an inde-
ies against isosulfan blue in patients with previous anaphy-
pendent predictor of any severe reaction feature. Other re-
lactic reactions to isosulfan blue. However, they did not
searchers14 report that inhibition of the metabolism of
succeed with the serum of our patient. Despite this, an IgE-
angiotensin by ACE inhibitors and the following buildup of
mediated mechanism can be assumed, although older publi-
bradykinin and substance P might predispose some individ-
cations suggest pseudoallergic mechanisms.22 Given the rel-
uals to anaphylaxis and to being more refractory to treatment
atively small molecular weight of isosulfan blue, it is likely to
act as a hapten. Approximately 50% of the isosulfan blue in
Biphasic courses of the reaction have sometimes been
aqueous solutions is weakly bound to serum proteins, which
described. They may be attributed to the slow release of the
allows for its characteristic lymphatic tropism.19
dye from the subcutaneous tissue or the lymphatic tissue and
Methylene blue is sometimes mentioned as another dye
the half-life of the dye in the body of several hours. Blue or
successfully used for lymphatic mapping.8,23 The methylene
green serum, urine, or skin discoloration for up to 24 hours
blue known under CAS No. 61-73-4 (anhydrous methylene
blue) or CAS No. 7220-79-3 (methylene blue trihydrate), how-
blue [letter]. Dermatology. 1998;197:400.
ever, is only approved for intravenous administration for the
8. Ebo DG, Wets RD, Spiessens TK, Bridts CH, Stevens WJ.
treatment of methemoglobinemia and hemolysis because it may
Flow-assisted diagnosis of anaphylaxis to patent blue. Allergy.
cause necrosis on subcutaneous administration. It has the total
9. Leong SPL, Donegan E, Heffernon W, et al. Adverse reactions
formula C H ClN S and is the trihydrate of the 3,7-bis(dim-
to isosulfan blue during selective sentinel lymph node dissection
ethylamino) phenazathionium chloride. According to Tsopelas
in melanoma. Ann Surg Oncol. 2000;7:361–366.
and Sutton,24 methylene blue does not bind to plasma proteins,
10. Montgomery LL, Thorne AC, Van Zee KJ, et al. Isosulfan blue
having no sulfonic acid groups, and, therefore, is not taken up by
dye reactions during sentinel lymph node mapping for breast
lymph but diffuses directly into blood capillaries. Unfortunately,
cancer. Anesth Analg. 2002;95:385–388.
the exact name of the product used is not always given so that
11. Sprung J, Tully MJ, Ziser A. Anaphylactic reactions to isosulfan
the question of possibly another nomenclature problem cannot
blue dye during sentinel node lymphadenectomy for breast
be answered. However, methylene blue is structurally not related
cancer. Anesth Analg. 2003;96:1051–1053.
to isosulfan blue or patent blue V, and, therefore, cross-reactivity
12. Efron P, Knudsen E, Hirshorn S, Copeland EM III. Anaphylac-
tic reaction to isosulfan blue used for sentinel node biopsy: casereport and literature review. Breast J. 2002;8:396 –399.
13. Brown SGA. Clinical features and severity grading of anaphy-
CONCLUSION
laxis. J Allergy Clin Immunol. 2004;114:371–376.
Anaphylactic reactions are a dreaded intraoperative complica-
14. Ober AI, MacLean JA, Hannaway PJ. Life-threatening anaphy-
tion. As SLNBs are increasingly performed in patients with
laxis to venom immunotherapy in a patient taking an angioten-
various malignant tumors, the likelihood of anaphylactic reac-
sin-converting enzyme inhibitor. J Allergy Clin Immunol. 2003;
tions to vital blue dyes increases. Incidences of 0.6% to 2.7% for
anaphylactic reactions to either isosulfan blue or patent blue V
15. Sampson HA, Mendelson L, Rosen JP. Fatal and near-fatal
necessitate awareness of the risk on the part of the surgeon and
anaphylactic reactions to food in children and adolescents.
the anesthesiologist. Preoperative antiallergic prophylaxis appar-
N Engl J Med. 1992;327:380 –384.
ently reduces only the severity of the reactions and not the
16. Lee JM, Greenes DS. Biphasic anaphylactic reactions in pedi-
atrics. Pediatrics. 2000;106:762–766.
number of adverse events, with a consecutive increase in post-
17. Albo D, Wayne JD, Hunt KK, et al. Anaphylactic reactions to
operative wound problems. Preoperative intracutaneous testing,
isosulfan blue dye during sentinel lymph node biopsy for breast
which can easily be performed, should, therefore, be taken into
cancer. Am J Surg. 2001;182:393–398.
consideration as a potential diagnostic procedure.
18. Raut CP, Daley MD, Hunt KK, et al. Anaphylactoid reactions to
isosulfan blue dye during breast cancer lymphatic mapping in
ACKNOWLEDGMENTS
patients given preoperative prophylaxis. J Clin Oncol. 2004;22:
We thank Bu¨hlmann Inc, Allschwil, Switzerland, for per-
forming CAST and Flow-CAST; Pharmacia for investigating
19. Coleman RL, Whitten CW, O’Boyle J, Sidhu B. Unexplained
the serum for specific IgE to the dyes; Dr Focke-Tejkl (Vi-
decrease in measured oxygen saturation by pulse oximetry
enna, Austria) for attempting to detect specific IgE to isosul-
following injection of lymphazurin 1% (isosulfan blue) during alymphatic mapping procedure. J Surg Oncol. 1999;70:126 –129.
fan blue; and J. L. Gue´ant (Nancy, France) for determining
20. Laurie SA, Khan DA, Gruchalla RS, Peters G. Anaphylaxis to
specific IgE to thiopental, cefaclor, and propofol.
isosulfan blue. Ann Allergy Asthma Immunol. 2002;88:64 – 66.
21. Woehrl S, Focke M, Hinterhuber G, et al. Near fatal anaphylaxis
REFERENCES
to patent blue V. Br J Dermatol. 2004;150:1037–1038.
1. Currie M, Webb RK, Williamson JA, et al. The Australian Inci-
22. Longnecker SM, Guzzardo MM, Van Voris LP. Life threaten-
dence Monitoring Study: clinical anaphylaxis: an analysis of 2000
ing anaphylaxis following subcutaneous administration of iso-
incidence report. Anaesth Intensive Care. 1993;21:621– 625.
sulfan blue 1%. Clin Pharmacol. 1985;4:219 –221.
2. Mertes PM, Laxenaire MC. Allergy and anaphylaxis in anes-
23. Nour A. Efficacy of methylene blue dye in localization of sentinel
thesia. Minerva Anestesiol. 2004;70:285–291.
lymph node in breast cancer patients. Breast J. 2004;10:388 –391.
3. Mertes PM, Alla F, Laxenaire MC. Anaphylactic and anaphy-
24. Tsopelas C, Sutton R. Why certain dyes are useful for localizing
lactoid reactions occurring during anesthesia in France in
the sentinel lymph node. J Nucl Med. 2002;43:1377–1382.
1999 –2000. Anesthesiology. 2003;99:536 –545.
4. Lieberman P, Kemp SF, Oppenheimer J, et al. The diagnosis
and management of anaphylaxis: an updated practice parameter. Requests for reprints should be addressed to:J Allergy Clin Immunol. 2005;115:S483–S523.
5. Ikeda T, Jinno H, Fujii H, Kitajima M. Recent development of
sentinel lymph node biopsy for breast cancer in Japan. Asian
6. Correction for Tsopelas and Sutton [erratum]. J Nucl Med.
7. Quiliquini A, Hogendijk S, Hauser C. Anaphylaxis to patent
ANNALS OF ALLERGY, ASTHMA & IMMUNOLOGY
Early patient outcomes after primary and revision total knee arthroplasty A PROSPECTIVE STUDY R. C. Hartley, N. G. Barton-Hanson, R. Finley, R. W. Parkinson From Arrowe Park Hospital, Upton, England There has been speculation as to how the outcome those after primary TKA, varying between 37% and of revision total knee arthroplasty (TKA) 89%.1-30 Many of the series were retrospective,
 Hypertension was treated with enalapril. After the smooth
Both dyes were injected in the upper back at 1:10 and 1:100
induction of general anesthesia, the patient developed, shortly
dilutions. After 15 minutes, the resulting wheals were docu-
after the start of surgery, generalized erythema, tachycardia,
mented using a digital camera (Coolpix 5000; Nikon USA,
a decline in blood pressure to 80/50 mm Hg, and conjuncti-
Melville, NY) through an optical device with an integrated
vitis. After the administration of vasoactive substances and
scale. The wheal circumference was determined in triplicate,
glucocorticosteroids and substitution of volume, her circula-
and the area was then calculated using the freeware NIH
tion returned to a stable condition and her shock symptoms
Image/J software V 1.3Ø win32 (National Institutes of
regressed. The postoperative course was uneventful.
Hypertension was treated with enalapril. After the smooth
Both dyes were injected in the upper back at 1:10 and 1:100
induction of general anesthesia, the patient developed, shortly
dilutions. After 15 minutes, the resulting wheals were docu-
after the start of surgery, generalized erythema, tachycardia,
mented using a digital camera (Coolpix 5000; Nikon USA,
a decline in blood pressure to 80/50 mm Hg, and conjuncti-
Melville, NY) through an optical device with an integrated
vitis. After the administration of vasoactive substances and
scale. The wheal circumference was determined in triplicate,
glucocorticosteroids and substitution of volume, her circula-
and the area was then calculated using the freeware NIH
tion returned to a stable condition and her shock symptoms
Image/J software V 1.3Ø win32 (National Institutes of
regressed. The postoperative course was uneventful.