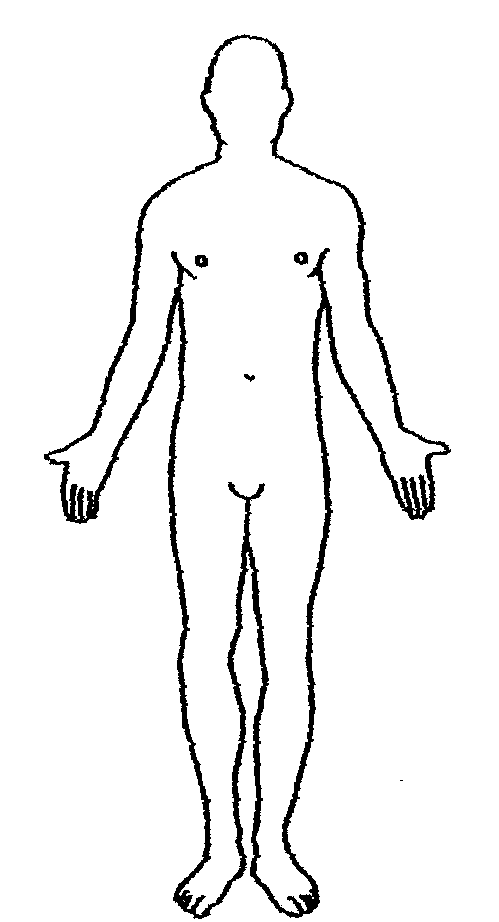
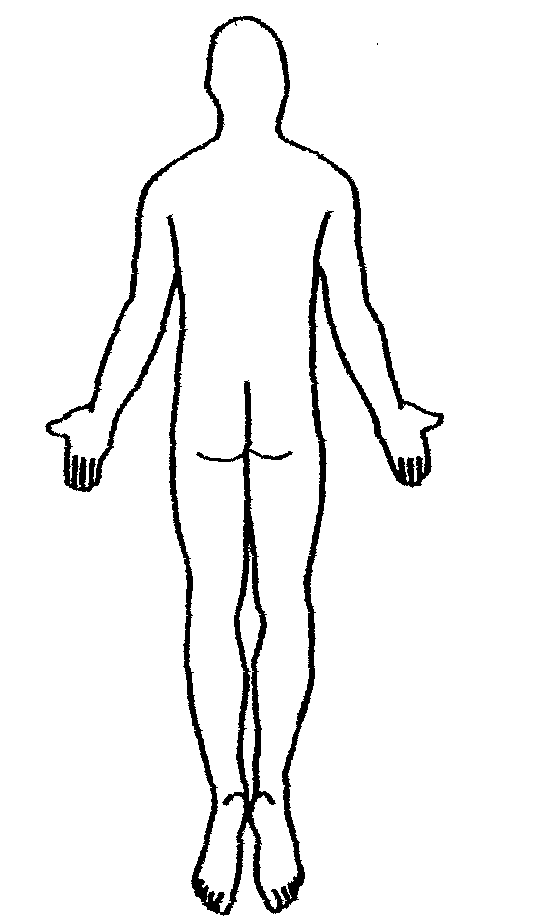
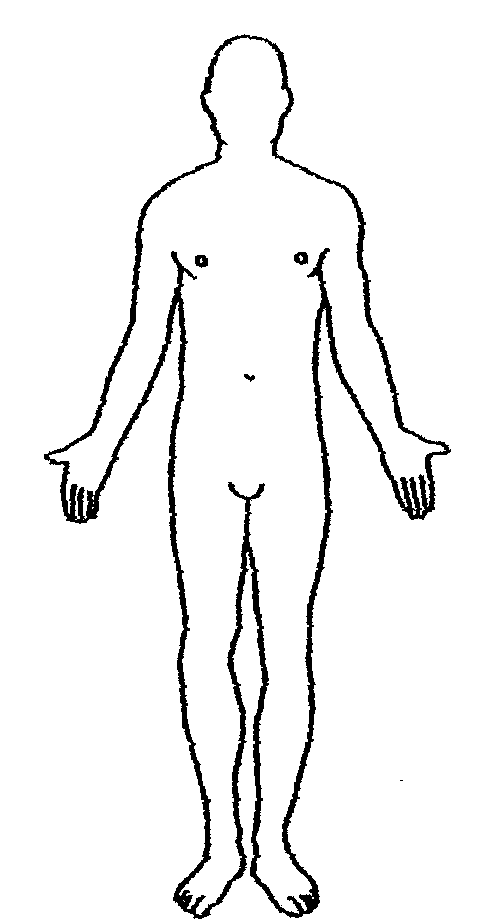
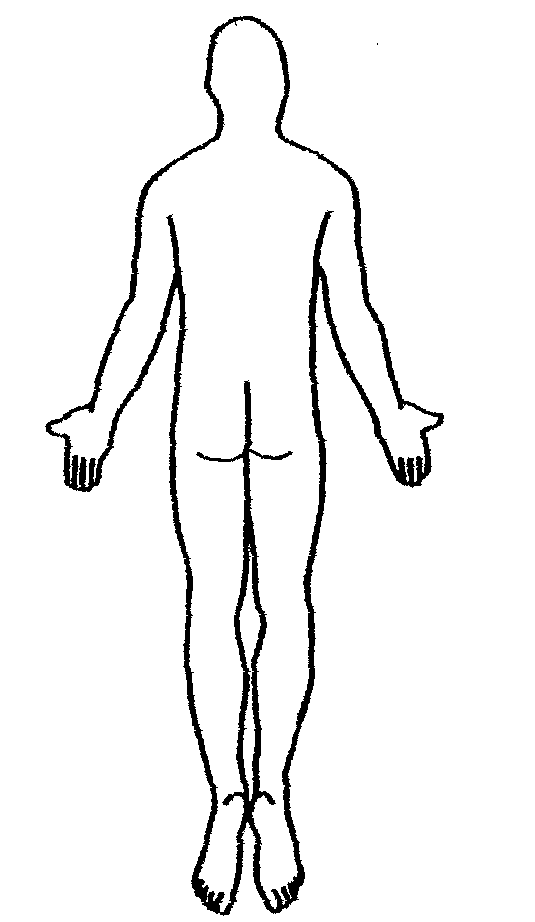
Patient Name: ______________________________ DOB: _________________ Date: _______________________ Sex: ______________ Weight: _____________________ Injury Information: Work Automobile Fall Other Date of injury: __________________________ Draw where you are experiencing your symptoms: Describe your symptoms/injury/reason for procedure: List any previous exams related to the body part being scanned today:
Is there any chance you might be pregnant? Y N
N/A Date of last period: ____________________________
Are you breastfeeding? Y N N/A Are you allergic to anything? Y N If yes, please list: _____________________________________________________
Medications you are currently taking: _____________________________________________________________________
____________________________________________________________________________________________________
Have you ever had an allergic reaction to MRI/CT contrast/dye? Yes No
If yes, please explain: ___________________________________________________________________________
List previous surgeries: _________________________________________________________________________________
CT Examinations Only: Not applicable Are you taking Glucophage, Glucovance, Avandemet, Metaglip or Fortamet? Have you ever had any history of the following? MRI Examinations Only: Not Applicable Do you have any of the following?
Metal in eye? Including metal shavings? If yes, explain: ________________________________________
Metal mesh implants/wire sutures/internal electrodes/wire staples? If yes, explain: ____________________
Gunshot wounds/shrapnel/BBs? If yes, explain: ________________________________________________
Any electrical, mechanical, or magnetic implants? If yes, explain: _________________________________
Implanted drug infusion pump/insulin pump? If yes, explain: _____________________________________
Dentures, partials, or dental implants? If yes, explain: ___________________________________________
Tattoos/permanent makeup/body piercings? If yes, explain: ______________________________________
Shunts/stents/intravascular coil? If yes, explain: _______________________________________________
Implanted cardiac stimulator? If yes, explain: _________________________________________________
Pacing wires/ Swann GANZ catheter? If yes, explain: ___________________________________________
Orthopedic pins, screws or rods? If yes, explain: ______________________________________________
Neurostimulator/biostimulator? If yes, explain: ________________________________________________
Heart surgery/Heart valve/pacemaker? If yes, explain: __________________________________________
Yes No Brain surgery/brain aneurysm clips? If yes, explain: ____________________________________________ Yes No
Eye surgery/implants? If yes, explain: _______________________________________________________
Ear surgery/Cochlear implants? If yes, explain: _______________________________________________
Do you have diabetes? If yes, explain: _______________________________________________________
History of cancer or tumors? If yes, explain: __________________________________________________
Previous back surgery? If yes, explain: _______________________________________________________
Do you have multiple myeloma? If yes, explain: _______________________________________________
Are you on renal dialysis? If yes, explain: _____________________________________________________
Do you have renal or kidney disease? If yes, explain: ___________________________________________
Do you have liver disease? If yes, explain: ____________________________________________________
Have you had a liver transplant? If yes, explain: _______________________________________________
Do you have hypertension? If yes, explain: ___________________________________________________
Do you have a blood disorder or sickle cell? If yes, explain: ______________________________________
I hereby consent to the performance of this procedure selected by my doctor, with whatever medication or treatment is necessary for the safe completion of this procedure. I authorize Southwest Diagnostic Centers to do whatever may be necessary in the event any unforeseen conditions arise during the course of this procedure. A small percentage of MRI patients may experience transient skin irritation from radio frequency of the MRI. A small percentage of CT patients may experience allergic reaction to the IV contrast administered with some CT exams. I agree the above information is correct to the best of my knowledge. I have read and understood the entire contents of this form and I have had the opportunity to ask any questions regarding information on this form. Patient Signature ________________________________________________________________ Date: ______________________ Technologist Signature ___________________________________________________________ Date: ______________________
For Office Use Only:
BUN ________________ Creatinine _________________ N/A
Contrast Administration: ________________CC of _________________________ with a ________________________ @ ___________________ Amount
X ________ in ____________________________________ Lot # ___________________ Expiration Date: _____________ # of punctures
Physician covering contrast: _____________________________________ By ____________________________________
Power injector: Yes No Rate: _______________cc per _____________seconds Contrast reaction? Yes No Explain: _________________________________________________________________
Datalogger T-PRINT is designed for logging temperature from one external probe into its internal memory. Datalogger T-PRINT-2 logs temperature from two external probes. Anytime it is possible to print out the record on the built in needle printer. The result is a hardcopy on the strip of paper of 58mm width. Format is numerical with date, time, place of measurement (vehicle, cold store). It
 MRI/CT SCREENING
MRI/CT SCREENING