Acta Neurochir (2013) 155:75–76DOI 10.1007/s00701-012-1532-9
Vestibular schwannoma presenting with psychosis
Received: 8 October 2012 / Accepted: 12 October 2012 / Published online: 14 November 2012
nursing on a secure psychiatric unit. Electroencephalographic
We describe an unusual case of vestibular schwannoma
(EEG) examination did not reveal any epileptiform activity.
presenting with psychotic symptoms, which resolved with
The lesion was removed via a retrosigmoid approach. A
remnant of the tumour was left at the internal auditory
A 22-year-old right-handed female presented with a 1-
meatus. Histological examination demonstrated a WHO
day history of abnormal behaviour. She was disorientated,
grade I vestibular schwannoma. She had complete sensori-
confused and claimed that the people around her were an
neural hearing loss in the left ear.
illusion. Over the preceding month she had become intro-
Following surgery the patient made a steady recovery.
verted, slept longer hours and stopped going out. She no-
Her visual and auditory symptoms receded and she stopped
ticed decreased hearing in the left ear and had been treated
risperidone 6 weeks postoperatively. At outpatient review at
for ear wax. On the day of presentation she reported that she
3 months she was entirely well and had applied to restart an
saw unusual shapes that made her feel like she was in
undergraduate course of study. Postoperative imaging
‘another world’. She shouted ‘I want God’ repeatedly and
revealed encephalomalacia in the left middle cerebellar pe-
then just ‘god’. At times she was unresponsive with rapid
duncle, consistent with prior compression (Fig. ).
eye movements. She became calmer following sedation and
This patient’s presentation is unusual for vestibular
explained that her imagination frightened her and that chant-
schwannoma, which commonly presents with hearing and
balance loss. Peduncular hallucinosis (PH) is a syndrome
There was no history of drug or alcohol abuse, and no
that combines hallucinations (‘sensory perception in the
previous medical or family history of note.
absence of external stimuli’) with brainstem symptoms. First
Imaging showed a large tumour in the left cerebellopon-
described by L’hermitte in 1922 it is associated with
tine angle with associated obstructive hydrocephalus
intrinsic brainstem lesions, subarachnoid haemorrhage and
(Fig. ). She was commenced on dexamethasone and un-
surgical trauma in the posterior fossa However there is
derwent insertion of a ventriculoperitoneal shunt.
no description of a vestibular schwannoma that presented
The patient’s psychosis was treated with risperidone. Further
with PH and resolved with resection. It was postulated that
review revealed auditory and visual hallucinations. She de-
our patient’s auditory hallucinations were linked to hearing
scribed ringing in the left ear interspersed with voices saying
loss and tinnitus in the left ear, following a ‘disinhibition’
‘I hate you’. She was unable to describe her visual hallucina-
model ]. It is not clear that this is the case, however.
tions other than reporting they were on the ceiling. Her psy-
Psychosis was not related solely to auditory symptoms, and
chosis and agitation worsened, which required intensive
her symptoms persisted for weeks following resection of thelesion and complete loss of hearing on the left side.
The psychosis of PH consists of visual hallucinations,
associated with hypersomnolence and oculomotor distur-
Department of Neurosurgery, National Hospital for
bance. Causative lesions are usually located in the rostral
brainstem but are also found in the thalamus and basal
ganglia It is unusual for extrinsic brainstem compres-
London WC1N 3BG, UKe-mail: [email protected]
Fig. 1 a T2-weighted MRIshowing a left cerebellopontineangle space-occupying lesion(arrow). b T2-weighted post-
operative MRI that showsencephalomalacia (arrow) inthe left middle cerebellarpeduncle
Transient PH has been described secondary to extrinisic
compression of the brainstem by a cystic craniopharyng-ioma []. In this case the symptoms also resolved with relief
1. David AS (1999) Auditory hallucinations: phenomenology, neuro-
of the compression. Posterior compression of the brainstem
psychology and neuroimaging update. Acta Psychiatr Scand 99
by medulloblastoma has also been shown to cause halluci-
2. Demetriades AK, Bhangoo RS (2009) Peduncular hallucinosis and
nosis that resolved with excision Large posterior fossa
cerebellar cognitive affective syndrome: Letter to the editor. Acta
meningiomas have been associated with psychotic symp-
toms, which resolved within days of excision ]. The
3. Dunn DW, Weisberg LA, Nadell J (1983) Peduncular hallucinations
pathophysiological mechanism is unclear. There are numer-
caused by brainstem compression. Neurology 33(10):1360–1361
4. Maiuri F, Iaconetta G, Sardo L, Buonamassa S (2002) Peduncular
ous publications describing lesions around the limbic sys-
hallucinations associated with large posterior fossa meningiomas.
tem that present with psychotic symptoms []. The role of
the cerebellum in cognitive and emotional activity is less
5. Manford M, Andermann F (1998) Complex visual hallucinations.
documented, but may be implicated via influence on dopa-
6. Miyazawa T, Ito M, Yasumoto Y (2009) Peduncular hallucinosis
following microvascular decompression for trigeminal neuralgia
Our report confirms the possibility that compression of
without direct brainstem injury: case report. Acta Neurochir
the brainstem by an extra-axial posterior fossa tumour can
present with psychosis. Psychiatric symptoms resolved with
7. Nadvi SS, van Dellen JR (1994) Transient peduncular hallucina-
tions secondary to brain stem compression by a medulloblastoma.
8. Ouma JR (2004) Psychotic manifestations in brain tumour patients: 2
case reports from South Africa. Afr Health Sci 4(3):189–193
9. Pollak L, Klein C, Rabey JM, Schiffer J (1996) Posterior fossa
Contributors RM and NK jointly conceived and wrote this report.
lesions associated with neuropsychiatric symptomatology. Int JNeurosci 87(3–4):119–126
10. Reeves RRR, Torres RAR (2003) Exacerbation of psychosis by
misinterpretation of physical symptoms. South Med J 96(7):702–704
that one treatment per week will be appropriate for most patients, however prescribers may exercise their clinical judgement should a patient request more than this. Drugs for ED may have a street value and the issue of diversion should be borne in mind when considering prescription quantities. February 2009 OSTEOPOROSIS GUIDELINES: Alendronate is the drug of first choice on DRUG
What is Thrush? Thrush/nipple yeast and vaginal yeast are caused by the one-celled organism, Candida albicans. It is a fungus that thrives in moist, dark environments (like the nipples, milk ducts, mother's vagina, baby's mouth and/or baby's diaper area). The use of antibiotics by mom or baby is a con-tributing factor in the occurrence of yeast. A cracked or sore nipple can also contribute to
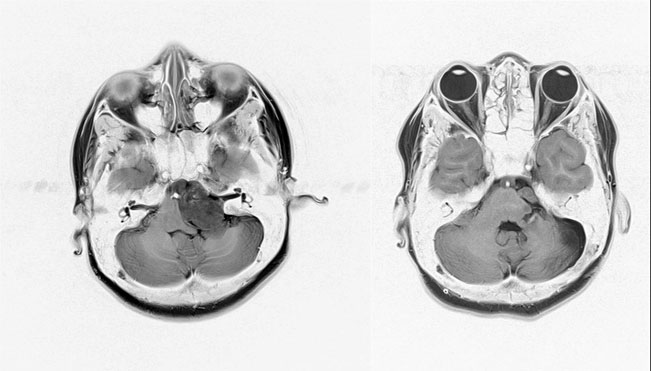 Fig. 1 a T2-weighted MRIshowing a left cerebellopontineangle space-occupying lesion(arrow). b T2-weighted post-
operative MRI that showsencephalomalacia (arrow) inthe left middle cerebellarpeduncle
Transient PH has been described secondary to extrinisic
compression of the brainstem by a cystic craniopharyng-ioma []. In this case the symptoms also resolved with relief
1. David AS (1999) Auditory hallucinations: phenomenology, neuro-
of the compression. Posterior compression of the brainstem
psychology and neuroimaging update. Acta Psychiatr Scand 99
by medulloblastoma has also been shown to cause halluci-
2. Demetriades AK, Bhangoo RS (2009) Peduncular hallucinosis and
nosis that resolved with excision Large posterior fossa
cerebellar cognitive affective syndrome: Letter to the editor. Acta
meningiomas have been associated with psychotic symp-
toms, which resolved within days of excision ]. The
3. Dunn DW, Weisberg LA, Nadell J (1983) Peduncular hallucinations
pathophysiological mechanism is unclear. There are numer-
caused by brainstem compression. Neurology 33(10):1360–1361
4. Maiuri F, Iaconetta G, Sardo L, Buonamassa S (2002) Peduncular
ous publications describing lesions around the limbic sys-
hallucinations associated with large posterior fossa meningiomas.
Fig. 1 a T2-weighted MRIshowing a left cerebellopontineangle space-occupying lesion(arrow). b T2-weighted post-
operative MRI that showsencephalomalacia (arrow) inthe left middle cerebellarpeduncle
Transient PH has been described secondary to extrinisic
compression of the brainstem by a cystic craniopharyng-ioma []. In this case the symptoms also resolved with relief
1. David AS (1999) Auditory hallucinations: phenomenology, neuro-
of the compression. Posterior compression of the brainstem
psychology and neuroimaging update. Acta Psychiatr Scand 99
by medulloblastoma has also been shown to cause halluci-
2. Demetriades AK, Bhangoo RS (2009) Peduncular hallucinosis and
nosis that resolved with excision Large posterior fossa
cerebellar cognitive affective syndrome: Letter to the editor. Acta
meningiomas have been associated with psychotic symp-
toms, which resolved within days of excision ]. The
3. Dunn DW, Weisberg LA, Nadell J (1983) Peduncular hallucinations
pathophysiological mechanism is unclear. There are numer-
caused by brainstem compression. Neurology 33(10):1360–1361
4. Maiuri F, Iaconetta G, Sardo L, Buonamassa S (2002) Peduncular
ous publications describing lesions around the limbic sys-
hallucinations associated with large posterior fossa meningiomas.