TREATMENT OF PHIMOSIS WITH TOPICAL STEROIDS
Vol. 31 (4): 370-374, July - August, 2005
Official Journal of the Brazilian Society of Urology
TREATMENT OF PHIMOSIS WITH TOPICAL STEROIDS AND FORESKIN
TATIANA C. MARQUES, FRANCISCO J.B. SAMPAIO, LUCIANO A. FAVORITO
Urogenital Research Unit, State University of Rio de Janeiro, Rio de Janeiro, RJ, BrazilABSTRACT
Objectives: To correlate topical steroidal treatment of stenosed foreskin with the different
degrees of glans exposure and the length of time the ointment is applied.
Materials and Methods: We studied 95 patients with phimosis, divided according to the
degree of foreskin retraction. Group A presented no foreskin retraction, group B presented exposureof only the urethral meatus, group C presented exposure of half of the glans, and group D presentedexposure of the glans, which was incomplete because of preputial adherences to the coronal sulcus. Patients were submitted to application of 0.05% betamethasone ointment on the distal aspect of theprepuce twice daily for a minimum of 30 days and a maximum of 4 months.
Results: Of 95 patients, 10 (10.52%) abandoned the treatment and 15 patients in groups C
and D were excluded from the study. Among the remaining 70 patients, only 4 patients (5.7%) ingroup A did not obtain adequate glans exposure after treatment. In group A (38 patients), fully retract-able foreskins were obtained in 19 patients (50%) after 1 month of treatment. In group B (28 patients),fully retractable foreskins were obtained in 18 patients (64.2%) after 1 month.
Conclusions: Treatment was successful in 94.2% of patients, irrespective of the type of fore-
skin anatomy. The improvement may require several months of treatment. Patients with impossibilityof urethral meatus exposure present around 10% treatment failure. Key words: penis; phimosis; anatomy; steroids; circumcision Int Braz J Urol. 2005; 31: 370-4 INTRODUCTION
ally transmitted diseases and, in adults, carcinoma ofthe penis (2).
Circumcision is frequently performed in the
The correction of phimosis in infancy is per-
United States and Canada, although in a variety of
formed with general anesthesia, a procedure that is
locations around the world, such as Europe and South
not without risks, with a complication rate that may
America, this procedure is not done on a routine ba-
reach 34% (3). The main complications following
sis. When it is not done routinely, the incidence of
circumcision are hemorrhage, stenosis of the urethral
pathological phimosis is increased (1). Pathological
meatus and the foreskin ring, and even amputation of
phimosis results when there are adherences to the fi-
the glans (4). In addition, this procedure presents con-
brotic foreskin ring that make it impossible to expose
the penis glans (1). This situation hinders adequate
Recently, clinical treatment of phimosis us-
penis hygiene, which favors the occurrence of fore-
ing topical corticosteroids has been proposed as an
skin infections, repeated urinary tract infections, sexu-
alternative to surgery with good results (6-8). Regard-
TREATMENT OF PHIMOSIS WITH TOPICAL STEROIDS
less of the patient’s age, the results are encouraging,
The patients were divided into groups accord-
with success rates ranging from 67 to 95% of cases
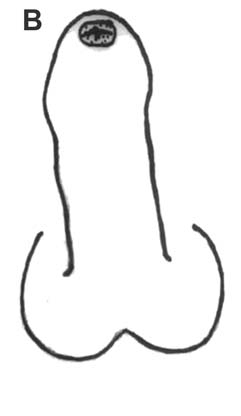
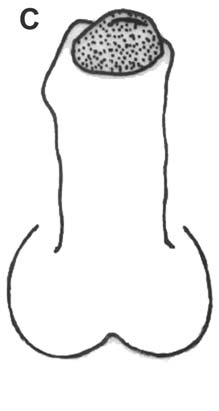
ing to the degree of foreskin retraction (11) (Figure-
1). Group A consisted of patients who presented no
There are several classifications for the posi-
foreskin retraction, group B presented exposure of
tion of the phimotic ring (1,2,9,10), although only
the urethral meatus only, group C presented expo-
Kayaba et al. (11) demonstrated the form and degree
sure of half of the glans, and group D presented in-
of retractability of the prepuce. Studies that correlate
complete exposure of the glans due to preputial ad-
foreskin anatomy with topical treatment using corti-
costeroids in patients with phimosis are rare, or even
After classification into one of the groups,
the patients were submitted to application of 0.05%
The objective of this work is to correlate topi-
betamethasone ointment on the phimotic ring (distal
cal treatment of 0.05% betamethasone in the stenosed
aspect of the prepuce). Parents were instructed to
foreskin with the different degrees of exposure of the
gently apply traction to the foreskin until the ring
glans and the length of application needed for the
appeared, applying a thin layer of cream twice daily
foreskin to become fully retractable.
for a minimum of 30 days and a maximum of 4months, in association with correct hygiene of the
MATERIALS AND METHODS
penis. These children were followed every month inour outpatient service.
Between January 2001 and October 2003, we
Therapy was considered successful when the
evaluated 95 patients with phimosis for possible
prepuce was fully retractable with total glans expo-
circumcision. The patients ranged in age from 19
sure. Failure was considered when it was impossible
months to 14 years (mean age 7.7 years). The Human
to achieve glans exposure, when there was no alter-
Research Committee at our institution approved the
ation in the degree of stenosis after more than 4
investigation. An informed consent form was obtained
months, and if there was infection during the treat-
from the parents (mother or father) of each patient.
ment. In such cases, circumcision would be indicated. Figure 1 – Diagram based on the work by Kayaba et al. (11) showing the 4 types of foreskin according to the position of the phimotic ring and the retraction ability, as well as the incidence found in the present study. Group A - no foreskin retraction, group B - exposure of the urethral meatus, group C - exposure of half of the glans, and group D - incomplete exposure of the glans due to preputial adherences to the coronal sulcus.
TREATMENT OF PHIMOSIS WITH TOPICAL STEROIDS
For statistical analysis, we used the chi-
In group A, 8 patients (21%) were ≤ 3 years
squared test. P < 0.05 indicates statistically signifi-
old and 30 patients (79%) were > 3 year old. Of the
patients who responded to treatment in group A (38of 42 patients - 90.4%), fully retractable foreskins
were obtained in 19 patients (50%) after 1 month oftreatment, in 5 patients (13.1%) after 2 months, in 9
The type of foreskin anatomy found in the
patients (21.6%) after 3 months, and in 5 patients
95 children is shown in Table-1. There was a pre-
dominance of group A (43 children - 45.2%) and group
In group B (28 patients), 4 patients (14.2%)
B (34 - 35.7%). Groups C (6 - 6.3%) and D (12 -
were ≤ 3 years old and 24 patients (86%) were > 3
12.6%) presented a lower incidence. Of the 95 pa-
year old. All patients in group B responded to treat-
tients, 10 (10.52%) abandoned the treatment and 15
ment and fully retractable foreskins were obtained in
patients in groups C and D were excluded from the
18 patients (64.2%) after 1 month, in 6 patients
study because they were not strictly considered as
(21.4%) after 2 months, in 1 patient (3.5%) after 3
having phimosis. Among the patients who abandoned
months, and in 3 patients (10.7%) after 4 months.
treatment, one presented the foreskin anatomy of
Independently of the group they were classi-
group A, 6 of group B and 3 of group D. Among the
fied, 37 of the patients (56%) achieved glans expo-
remaining 70 patients, only 4 patients (5.7%) in group
sure within 30 days of treatment. Only 8 patients
A did not obtain adequate exposure of the glans after
(12.1%) required 4 months of treatment to obtain a
fully retractable prepuce. No adverse side effects were
Of the 66 patients (94.2%) who did obtain
observed from the topical betamethasone treatment.
adequate exposure of the glans after treatment (fully
There was no statistically significant difference in
retractable prepuce), 38 (57.5%) were in group A and
satisfactory response to treatment over the course of
28 (42.5%) were in group B. The response to topical
treatment for the groups studied in relation to thelength of time the ointment was used is shown in
COMMENTS
Physiological phimosis affects 96% of new-
borns and its incidence diminishes with age. At 3 years
Table 1 – Incidence of the different types of foreskin
old, 10% of boys present phimosis and by the age of
anatomy found in the present study.
14 years, this incidence decreases to 1% (13). Foreskin Anatomy Patients %
In Australia at the beginning of the 1990s,
Kikiros et al. (10) attested to the efficacy of topical corti-
costeroids in the treatment of preputial stenosis. Since
then, several authors have shown satisfactory results
(67% to 95%) with the topical use of betamethasone,
clobetasol, sodium diclofenac, 0.05% mometasone
furoate and triamcinolone acetonide (8-10). Table 2 – Therapeutic success rate for groups A and B in relation to the length of time the ointment was applied.
TREATMENT OF PHIMOSIS WITH TOPICAL STEROIDS
Betamethasone is one of the steroids that
to have foreskin retraction (group A), which was the
present the best improvement rates (13,14), and this
most frequent situation among our patients (incidence
was the reason the drug was used in this study. Corti-
of 45%). Patients with foreskin anatomy in groups B
costeroids act by reducing the arachidonic and
presented a high chance of obtaining the desired result
hydroxyeicosatetraenoic acids in proliferative inflam-
with treatment duration of less than 60 days.
matory disease of the skin, thereby inhibiting pros-
In conclusion, topical treatment of phimosis
taglandin release and increasing the activity of
using 0.05% betamethasone ointment presented a
dismutase superoxide. Additionally, they have the
success rate of 94.2%, regardless of the form and
potential to release antioxidants (13). Collateral ef-
degree of foreskin retraction. Most previous reports
fects may occur, such as the suppression of the hypo-
have described one month of treatment; nevertheless,
thalamus-hypophysis-adrenal axis or cutaneous atro-
we found that the desired improvement might take
phy. However, the doses utilized in topical treatment
of phimosis are not large enough to lead to these typesof complications (1). In our study, we did not observe
REFERENCES
any adverse effects in our patients.
Orsola A, Caffaratti J, Garat JM: Conservative treat-
ment of phimosis in children using a topical steroid.
the treatment with 0.05% betamethasone ointment,
which is similar to what has been found in recent stud-
Elmore JM, Baker LA, Snodgrass WT: Topical ste-
ies in the literature (1,2,13,15-18). All patients were
roid therapy as an alternative to circumcision for phi-
advised to continue retracting the foreskin to main-
mosis in boys younger than 3 years. J Urol. 2002; 168:
tain penile hygiene. We observed parent satisfaction
when the decision to pursue conservative treatment
Chu CC, Chen KC, Diau GY: Topical steroid treat-
was made. Topical treatment using corticosteroids has
ment of phimosis in boys. J Urol. 1999; 162: 861-3.
been shown to have low risk with an absence of side
Ozkan S, Gurpinar T: A serious circumcision compli-
effects and good adherence to treatment when those
cation: penile shaft amputation and a new reattachment
responsible for the child have been well briefed.
technique with a successful outcome. J Urol. 1997;
Berdeu D, Sauze L, Ha-Vinh P, Blum-Boisgard C:
evolution of the phimotic ring has been shown to be
Cost-effectiveness analysis of treatments for phimo-
fundamental in the assessment of the time at which
sis: a comparison of surgical and medicinal approaches
the therapy utilized is having its effect, or whether it
and their economic effect. BJU Int. 2001; 87: 239-44.
is ineffective. Therapy can be stopped at any time
Gulobovic Z, Milanovic D, Vukadinovic V, Rakie I,
Perovic S: The conservative treatment of phimosis in
improvement after using the ointment and required a
Wright JE: The treatment of childhood phimosis with
surgical procedure were in group A. Among the
topical steroid. Aust N Z J Surg. 1994; 64: 327-8. Er-
patients in group A who responded to topical
ratum in: Aust N Z J Surg. 1995; 65: 698.
treatment, 35% obtained the desired result only after
Jorgensen ET, Svensson A: The treatment of phimosis
3 or 4 months of treatment. The patients without any
in boys, with a potent topical steroid (clobetasol pro-
foreskin retraction (group A) presented an
pionate 0.05%) cream. Acta Derm Venereol. 1993; 73:55-6.
approximately 10% chance of not benefiting from
Atilla MK, Dundaroz R, Odabas O, Ozturk H, Akin R,
clinical treatment, even after a long period of ointment
Gokcay E: A non-surgical approach to the treatment
use, and such patients will require circumcision. In
of phimosis: local non-steroidal anti-inflammatory
group B, 70% of the patients showed the desired result
ointment application. J Urol. 1997; 158: 196-7.
within the first two months of ointment application.
10. Kikiros CS, Beasley SW, Woodward AA. The response
These results are very significant at the time of
of phimosis to local steroid application. Pediatr Surg.
indicating the treatment, especially for patients unable
TREATMENT OF PHIMOSIS WITH TOPICAL STEROIDS
11. Kayaba H, Tamura H, Kitajima S, Fujiwara Y, Kato T,
prospective, randomized, double-blind study. Scand J
Kato T: Analysis of shape and retractability of the pre-
puce in 603 Japanese boys. J Urol. 1996; 156: 1813-5.
16. Lee KS, Koizumi T, Nakatsuji H, Kojima K, Yamamoto
12. Sokol RR, Rohlf FJ: Biometry, 3rd (ed.), New York,
A, Kavanishi Y, et al.: Treatment of phimosis with
betamethasone ointment in children. Nippon Hinyokika
13. Shankar KR, Rickwood AM: The incidence of phimo-
sis in boys. BJU Int. 1999; 84: 101-2.
17. Monsour MA, Rabinovitch HH, Dean GE: Medi-
14. Marzaro M, Carmignola G, Zoppellaro F, Schiavon G,
cal management of phimosis in children: our ex-
Ferro M, Fusaro F, et al.: Phimosis: when does it re-
perience with topical steroids. J Urol. 1995; 162:
quire surgical intervention? Minerva Pediatr. 1997; 49:
18. Ashfield JE, Nickel KR, Siemens DR, MacNeily AE,
15. Lund L, Wai KH, Mul LM, Yeung CK: Effect of topi-
Nickel JC: Treatment of phimosis with topical steroids
cal steroid on non-retractile pre-pubertal foreskin by a
in 194 children. J Urol. 2003; 169: 1106-8. Accepted after revision: June 20, 2005Correspondence address: Dr. Luciano Alves Favorito Urogenital Research Unit - UERJ Av. 28 de Setembro, No. 87, fundos Rio de Janeiro, RJ, 20551-030, Brazil Fax: + 55 21 2587-6121 E-mail: [email protected] EDITORIAL COMMENT
the results in this study, this would seem the best
treatment of phimosis in children with betamethasone
treatment for phimosis causing ballooning of the
ointment as has been shown in other studies. In
prepuce with voiding and/or when phimosis is thought
addition, they have demonstrated success with lower
to be causing recurrent infections. These authors do
dose betamethasone ointment (0.05% instead of 0.1%)
not note that any of these boys had symptoms. While
and that only one month treatment is needed in about
these authors and others have shown resolution of
half of the cases. However, they do not report on long
phimosis with steroid ointment, they have not
term follow-up to determine if recurrence is a
demonstrated that treating asymptomatic phimosis in
problem. Ashfield et al. (Reference 18 in article) also
pre-pubertal boys has any medical benefit.
did not report long term follow-up but they examinedpatients six weeks following cessation of treatment,
Dr. Jean G Hollowell
which should have at least detected early recurrences. Children’s Hospital of the King’s Daughters
The more important point on this topic to
and Eastern Virginia Medical School
consider is when this treatment is indicated. From
Methylphenidate and Dextroamphetamine Abuse Methylphenidate and Dextroamphetamine Abuse in Substance-Abusing Robert J. Williams, PhD1; Leslie A. Goodale, RN2; Michele A. Shay-Fiddler, MSW2; Susan P. Gloster, BN3; Samuel Y. Chang, MD2 1. Addiction Counselling Program; School of Health Sciences; University of Lethbridge 2. Addiction Centre; Foothills Medical Centre; Calgary, Alberta 3. Lethbri
Subdirección General de Atención al Ciudadano y Asistencia a las Víctimas del Terrorismo LEY 10/1990 TÍTULO IX DE LA LEY 10/1990, DE 15 DE OCTUBRE, DEL DEPORTE (en su redacción dada por el artículo 115 de la Ley 53/2002, de 30 de diciembre) PREVENCIÓN DE LA VIOLENCIA EN LOS ESPECTÁCULOS DEPORTIVOS Artículo 60 1. Se crea la Comisión Nacional contra la Violencia en los Espec

 TREATMENT OF PHIMOSIS WITH TOPICAL STEROIDS
less of the patient’s age, the results are encouraging,
The patients were divided into groups accord-
with success rates ranging from 67 to 95% of cases
ing to the degree of foreskin retraction (11) (Figure-
1). Group A consisted of patients who presented no
There are several classifications for the posi-
foreskin retraction, group B presented exposure of
tion of the phimotic ring (1,2,9,10), although only
the urethral meatus only, group C presented expo-
Kayaba et al. (11) demonstrated the form and degree
sure of half of the glans, and group D presented in-
of retractability of the prepuce. Studies that correlate
complete exposure of the glans due to preputial ad-
foreskin anatomy with topical treatment using corti-
costeroids in patients with phimosis are rare, or even
After classification into one of the groups,
the patients were submitted to application of 0.05%
The objective of this work is to correlate topi-
betamethasone ointment on the phimotic ring (distal
cal treatment of 0.05% betamethasone in the stenosed
aspect of the prepuce). Parents were instructed to
foreskin with the different degrees of exposure of the
gently apply traction to the foreskin until the ring
glans and the length of application needed for the
appeared, applying a thin layer of cream twice daily
foreskin to become fully retractable.
TREATMENT OF PHIMOSIS WITH TOPICAL STEROIDS
less of the patient’s age, the results are encouraging,
The patients were divided into groups accord-
with success rates ranging from 67 to 95% of cases
ing to the degree of foreskin retraction (11) (Figure-
1). Group A consisted of patients who presented no
There are several classifications for the posi-
foreskin retraction, group B presented exposure of
tion of the phimotic ring (1,2,9,10), although only
the urethral meatus only, group C presented expo-
Kayaba et al. (11) demonstrated the form and degree
sure of half of the glans, and group D presented in-
of retractability of the prepuce. Studies that correlate
complete exposure of the glans due to preputial ad-
foreskin anatomy with topical treatment using corti-
costeroids in patients with phimosis are rare, or even
After classification into one of the groups,
the patients were submitted to application of 0.05%
The objective of this work is to correlate topi-
betamethasone ointment on the phimotic ring (distal
cal treatment of 0.05% betamethasone in the stenosed
aspect of the prepuce). Parents were instructed to
foreskin with the different degrees of exposure of the
gently apply traction to the foreskin until the ring
glans and the length of application needed for the
appeared, applying a thin layer of cream twice daily
foreskin to become fully retractable.