Microsoft word - condoms and viagra_jramakrishna.doc
Condoms and Viagra: An exploration of processes and forces that shape notions of sexuality and policies Jayashree Ramakrishna, PhD, MPH
National Institute of Mental Health & Neuro Sciences (NIMHANS)
Abstract
Examination of the development, propagation, acceptance and use of two sex-related products condoms and Viagra provides a keen heuristic devise for exploring contexts, processes and factors that shape sexuality and policies related to sexuality. Juxtaposing condoms and Viagra affords sharp contrasts that focus attention on perceptions of femininity and masculinity and changing cultural and societal norms in the context of hardening of national and other identities. This paper centres on the Indian experience; it attempts to tease out the cultural, social and economic processes and factors (including vacillations in international policies) that have inhibited the acceptance of condoms, the persistence of the ‘culture of silence’ with regard to sexuality, and the increasing intolerance of diversity. While condoms and sexual education have been part of public health and cultural discourse, Viagra has essentially remained confined to the medical arena. However, in a short time Viagra has become accessible (the process being eased by neo-liberal economy) and has gained acceptance. The juxtaposition of condoms and Viagra in the Indian milieu also highlights the tension between prevention and curative aspects of biomedicine and the privileging of the latter over the former. The differing standards used for approval of female condoms and the research pointing to the utility of Viagra for treating sexual dysfunction in women on antidepressant is telling. The paper ends with a brief discussion of innovative responses to disregard/violation of sexual rights, the effective use of media and community mobilisation (both traditional and internet based) to bring the issue to the national forefront. Examination of the development, propagation, acceptance and use of condoms and Viagra provides a keen heuristic devise for exploring contexts, processes and factors that shape sexuality and policies related to sexuality. Juxtaposing condoms and Viagra affords sharp contrasts, which focus attention on cultural and societal norms, religious injunctions, perceptions of femininity and masculinity, in the context of national identities and the neo- liberal economy. This understanding might help to better identify points and ways of influencing these processes. This paper centres on the Indian experience; it attempts to tease out the processes and factors that have inhibited the acceptance of condoms, the project to develop a homogenised consensual version of ‘Indian male and female sexuality. In this paper I shall first briefly discuss the devices under consideration. The concept of condom – a device to place on a man's erect penis and physically blocks ejaculated semen from entering the body of a sexual partner has been known for a long time. Historically ‘condoms’ were made from various substances ranging from horn/ animal skin to oiled silk. Modern condoms are usually made of latex or polyurethane, and are used as a contraceptive to prevent pregnancy and or to prevent the spread of sexually transmitted illnesses. This is the most commonly used barrier method contraceptive. The efficacy of condoms in preventing conception is well documented, and failure rate among those who use them correctly and consistently is very low. The active ingredient in Viagra is sildenafil citrate, an enzyme that regulates blood flow to the penis. This drug was being tested for treating angina pectoris a symptom of ischemic heart disease. While it was found that the drug has little effect in angina it induced penile erections. This fortuitous discovery led to the patent of this molecule in 1996, and in record time in 1998 the US Food and Drug Administration approved it as the first oral medicine for erectile dysfunction (inability to sustain a satisfactory erection to complete intercourse).
Sildenafil citrate also relaxes the arterial wall it is effective in a rare disease, pulmonary arterial hypertension (PAH) and improves symptoms of heart failure. After seven years Pfizer submitted an additional registration for sildenafil to the FDA for this indication. It is sold under the brand name Revatio and the 20 milligram tablets are white and round to differentiate it from the distinctive blue Viagra that are variously know as ‘bolt from the blue.’ Taking sildenafil with medications or other substances that contain nitrate causes in a serious decrease in blood pressure and results in fainting, stroke or heart attack. Nitrates are also found in recreational drugs such as amyl nitrate poppers. Sildenafil is contraindicated for persons who have heart disease, diabetes, high blood pressure, high cholesterol. Alpha beta blockers, antifugal medicine - azole, and rifampician are inadvisable. There is also an adverse reaction with antiretrovirals prescribed to those who have HIV infection. Some mention those who smoke or use alcohol or are over 50 years of age. However these interactions and contraindications are not highlighted, much of it only came to public notice after users complained about problems. In the rest of the paper I shall attempt to show how cultural notions, as well as larger macro processes affect the construction of sexuality and the course of action taken. The play of power be it between the genders, the majority and the minority, the state and the individual, global economy and local/regional economies, and the overarching trans-national global processes crucial to this understanding.
Concepts of masculinity, manhood and fertility in India
As in most patriarchal cultures, sexual prowess is associated with manhood, masculinity, strength, vigour and procreativity. In the Ayurvedic (Indian system of medicine) tradition semen is seen as one of the most important of the seven vital fluids of the body; harmony of all these fluids produces good health. Semen is precious because it takes 40 days for 40 drops of food to be converted into one drop of blood, 40 drops of blood is needed to make up one drop of bone marrow and it takes 40 drops of bone marrow to make one drop of semen. Thus it is understandable that men want to conserve this precious fluid, and put it to right use, i.e. for procreation.
Fertility in women is valued and the motherhood is hallowed. Marriage is almost universal. It is the most sacred duty of parents to arrange the marriage of their children, especially that of their daughters and free them from the confines of maidenhood. The woman’s status in society is affirmed when she has a child, particularly a son. Traditionally couples are expected to have children soon after marriage. Delaying pregnancy is not advised by elder, and young married women say that their doctors do not advice them to use contraceptives till after they have had their first child. Stories of couples who postponed pregnancy and could not conceive when they wanted to abound.
The stages of life (for men) are well laid out, childhood and youth (till 21 year of age) is for learning and developing, during that time excessive interest in sex is thought to be detrimental. Celibacy is advocated, conserving sexual energy is thought to increase physical strength and vigour as well as intellectual acumen, and spiritual quotient. For instance, wrestlers are followers of Hanuman and remain celibate to maximise their physical strength. Similarly men in the pursuit of knowledge or God do the same. The next stage, a period of another 21 years is that of the householder and it is time for having children and raising a family and fulfilling worldly duties. After that are the hermitage and sanyasi stages are supposed to be essentially celibate.
Alongside these views, there is an opposing notion that sexual release is important, without this the body heats up and a man looses mental balance. There is wide spread concern about nocturnal emissions, premature ejaculation and anxiety about sexual performance. One of the most common complaints in men is “weakness”. (Verma et al) “Quacks” and various types of sexual specialists from those who operate out of roadside shacks to sexologist in modern clinics cater to men who have these conditions.
Pleasure underlies all sexual discourse, it is seen as a potent force that can over take all other concerns and therefore needs to be regulated. Any form of interaction or even the intermingling of young men and women is frowned upon. Sexual attraction and desire are thought to be irresistible. The norm of early marriage is a tacit acknowledgment of sexual needs of both young men and women. There is a great concern is not ‘keeping’ a marriageable girl at home, this is seen as a great responsibility and burden a something untoward may happen. It is well acknowledged that men get easily aroused and find it difficult to control their desire, but there is some ambivalence of the sexual nature of women, it swings between the notions of women as devi who are put on a pedestal. They are essentially asexual and embody the virtues of motherhood, devotion, goodness, nobility and sacrifice for the larger good. And then there is the idea of women as temptress, with insatiable desire who entice ‘helpless’ men.
Condoms are seen as inhibiting sexual activity, it restricts intimacy and skin to skin contact. It interferes with spontaneity. More over the use of condoms which are seldom seen as contraceptives are perceived as a sign of distrust of the partner. This is especially true in a country where most women who have had two or three children opt for permanent tubaligation/tubectomy and there is no need for contraception. Couples in India, especially in crowded urban low income areas have little privacy and time for sexual intercourse let alone using condoms. Purchasing condoms is embarrassing and disposing off used condoms a challenge. Further, in many cases sex takes place in the context of alcohol use and violence where the woman has little power to negotiate condom use.
Sex and sexual issues is not part of the cultural or general discourse, the culture of silence pervades. For one there is no commonly understood language. The medical/health professional are comfortable talking in terms of sexual anatomy, physiology and disorders. There is a well developed literary language but very little in the local languages that are not euphemistic and vague or vulgar and crude. And more over, as a female participant in one of my early research who happened to be a sex worker, noted ‘good women do not talk about sex, we may have sex but we do not talk about it.” This idea is a widely prevalent even among the health sector. This coupled with the middle class reticence about all matter sexual there is little discussion.
Population Control Programme
I shall briefly discuss the Indian National Family planning programme because this historical perspective provides an understanding of the current attitudes towards condoms. This programme was seen as key to development, and it was one of the first proprammes to be instituted after Independence in 1947. It received funding and technical support from USAID and technical assistance from donors such as the Ford Foundation. This was essentially a top down programme; Indian policy makers gave priority to controlling population growth, but it was not the priority of the common man/woman, fertility and procreation was valued. Agrarian families with many children could better meet high labour needs. Children were also social insurance, male children were especially valued. Initially it was essentially a clinic based approach following the traditional notion that contraception is a woman’s responsibility. Intrauterine devices were preferred; it was semi permanent method, controlled by physicians who inserted the IUD and removed it. Health care workers minimised the complications and side effects - infection, pain, bleeding and or general malaise. Women complained about these but saw no other option. Condoms were associated with prevention of sexually transmitted diseases and to sex with casual partners, ‘illicit relationships’ and sex outside marriage. When it was found that this method was not effective in reducing the population growth, the emphasis shifted to vasectomies. This was the first time a male centred method was used. There was much apprehension – both men and women felt that it would weaken the man. Men saw it as an assault on their manhood. However, because relatively high incentives were provided in cash and kind, men especially the rural poor participated. Health care workers who had to meet targets persuaded /coerced men into having vasectomies. In 1975 government declared a national internal emergency and democratic civil rights including reproductive rights were suspended. In 1976 a National Population Policy was adopted and suitable legislature to make family planning compulsory for citizens to stop
child bearing after three children if the state so desires. Constitutional amendment was introduced to freeze representation to the parliament from each state to 1971 level till 2001, thus providing no incentive to states to increase their population size. Quantum and magnitude of incentive were reduced. Government functionaries were forced to recruit stipulated numbers for vasectomy in their areas on the fear of punishment. Vasectomy camps (often in none too hygienic conditions) were held from 1975 to 1977, 8.26 million vasectomies were conducted. These coercive policies had a serious backlash when democracy was restored in April 1977; government was soundly defeated in the elections. New governments were apprehensive, and family planning took a backseat. The Family Planning Programme was renamed Family Welfare Programme, targets for sterilisation were changed, and education and motivation became the key strategy. One wonders whether a government would be toppled because of female oriented family planning programme. Condoms in the Indian Context
Condoms were only recognised with the threat of AIDS. In the early days, when there were no drugs for HIV treatment, the focus was firmly on prevention; the condom was the method of choice. With the encouragement of donor agencies condoms were promoted aggressively to a diverse audience and often with little sensitivity or recognition of cultural mores. Voices that spoke of the need for more culturally appropriate options, a wider array of choices such as delayed debut, were not heeded. For the first time there were public advertisement of condoms, some political figures endorsed condoms and won the approval of visiting donor representatives. In meetings the Thailand experience with condoms was highlighted, the skills of the Thai sex workers in motivating and convincing men to use condoms lauded. There was little attention to the difference in the sex work scenario in India and Thailand nor to the commitment of the Indian government to bring about similar changes. In addition to the advertisements, the government programme for the first time had counsellors who could promote condoms to individuals, and condom demonstration became a part of the HIV counsellors’ responsibilities. Unfortunately, even though the condom was to be used by the man, it became woman’s responsibility to motivate, cajole and entice the man to use the condom. Responsibility was given to the partner who had the least power and the least ability to respond.
Estimations made by international agencies showed that India would have larger number of people with HIV than South Africa and urged the Indian government to take swift and decisive action. The National AIDS Control Organisation protested that these numbers were inflated, but was disregarded. However, re-estimation using different more accurate parameters a couple of year later showed that the figures were closer to NACOs estimations, lower than what had been predicted.
In the ensuring years three events occurred that again turned the focus away from condoms. The US Bush administration strongly advocated abstinence only, or the ABC strategy - Abstinence, Be Faithful and Condom method, where the emphasis was on the first two options and condoms would be only a third option. Organisations that received President’s Emergency Plan for AIDS Relief (PEPFAR) funds were required to sign bonds they do not support prostitution or abortion services. They were also requested to report how many people they had counselled on abstinence and faithfulness. Those who had been championing for a wider range of options felt vindicated. This proposition also resonated with the conservative elements of all the religions, and condoms were again marginalised. Decisions
taken by powerful countries do not remain confined to their programmes but soon find there way into other international and national programmes. NACO too subscribed to this ideology and included this language in its policy and programme documents.
With the advent of antiretroviral therapy (ART) for HIV, especially of HAART, there was shift to providing treatment along with care. Understandably those who were infected wanted to access to these drugs, WHO set up an ambitious programme, and concerted effort was made to make affordable generic drugs available. This brought HIV firmly back into the biomedical domain. Increasing the focus shifted to testing and treatment and counselling and prevention services for general population was again deemphasised.
Condoms have been part of the Indian population control arsenal from the beginning of the family planning programme in the 1950s. In the early days condoms were purchased from the US as a part of the USAID programmes and then condom manufacturing began in India. Condoms have been associated with sex outside marriage, for prevention of sexually transmitted diseases. Condoms that were initially available in the government system were not of good quality, there were reports of breakage and damage. Early condoms were not lubricated. The new lubricated condoms did not have enough lubrication or were too oily. Storage of latex condoms in hot and humid climate was a challenge. This coupled with the disdain of all free things provided by government gave condoms a poor image. Considering the high demand for condoms the Indian government set up public sector unit – Hindustan Latex Limited (HLL) over 30 years ago. This company aims to make quality contraceptives available at affordable prices at ‘an arms length of desire.’ It is the largest condom manufacturer in the world producing 1316 million pieces. Condoms are subsidised by the government and marketed under name Nirodh (prevention), this is the local name for condom. These condoms are distributed free of cost through the government health care system. Apart from the varieties of Nirodh (deluxe, ultra deluxe, new lubricated) HLL also produces an array of –ultra thin, dotted, flavoured -premium Moods condoms. HLL also has a social marketing division aimed at those who can afford to pay only part of the commercial price. Social marketing of condoms have been taken up by NGOs, here the government or other subsidised condoms are packaged and sold at nominal costs at accessible locations. More upmarket coloured, flavoured, slickly packaged condoms, with erotic graphics (and advertisements) produced by the private and marketed under exciting brand names such as Kama Sutra, Trojan etc. In March 2007 HLL released a new product a premium condom with a vibrating ring called Crezendo. In mid May a state banned this condom stating that it was a sex toy and against Indian culture. "And sex toys," noted a minister, "can have serious repercussions on the Indian way of life." This action triggered an impassioned debate about the relationship between Indian culture and sexual pleasure. As common in these debates reference was made to Vatsyayana’s Kama Sutra, and the erotic imagery of the Khajuraho and Konark temples. In a newspaper article, Sen (2007) points out that ‘reducing the place of sex in India to these iconic works of art and literature is to make a mockery of Hindu traditions.’ He goes on to quote Nandi ‘erotic imagery is very much a part of Hindu texts and paintings.’ In the Hindu mystic bhakti tradition the devotee often views the divine as a beloved. Interestingly the soul, even of male saints is conceptualised as an ardent women, awaiting her beloved, and sexual fulfilment and pleasure are very much a part of the sacred domain. In another article Ghosh (2007) quotes Ram Nath Jha, who teaches in Special Centre for Sanskrit Studies, JNU, who observes that even ancient philosophical treatises talk of sex as a pleasure provider. Roy a
professor of ancient India adds that this was mainly directed towards men of the dominant elite groups. In response the Health minister noted that the ‘vibrating condom’ was just a variety of condom and it was developed by HLL to compete with private companies. He also stated that 50,000 condom vending machines had been installed at bus stops, washrooms, petrol pumps and dhabas (road side eateries) and there were plans to increase it to 100,000. He said that Crezendo would not be marketed in states that did not want it. The HLL spoke person also said the product would be withdrawn if asked to do so as they did not ‘want to create any controversy.’ even though 130,000 pieces had been sold since launch and no complaints had been received from users or the government. (Sinha) Female condoms Female condoms are described as a ‘travelling technology’, an interaction of technology, diffusion and donor agencies, possibility of greater women’s empowerment and sexual autonomy. Female condoms made of latex (FC1) were first developed in 1993. The second generation FC2, made polyurethane or nitrile polymer are thinner softer and quieter. These condoms conduct heat and preserve more sensation, they do not require special storage as they are unaffected by heat and moisture. Further they can be used with oil based lubricants though some do not recommend this. In 2007 in India HLL launched first female condom called Confidom. More than 0.5 million pieces have been sold and NACO hopes to increase it to 1.5 million by 2015. FDA classifies male condoms as class 2 devices that need to pass tests only for leakage and breakage; however it places female condoms as class 3 device in the same category as pacemakers, heart valve and silicone breast implants and needs to pass more stringent clinical tests. Some in FDA question whether further clinical trials are necessary to determine how FC2 prevents pregnancy. The Female Health Company FHC) did not think this necessary as the product has been used by 12 million in 77 countries and 3.47 million FC have sold in 2008. The FDA has cleared FC2 and it can be distributed by USAID. It still leaves the questions- Is it good or bad to have separate standards for male and female condoms? Does regulation this protect the safety of women? If so what about all the women in developing countries who have been using such female condoms for more than ten years, have they been guinea pigs? Or are American women losing out? Talking about sexuality and sexual issues To make informed decisions about sexual issues there needs to be a climate that allows dissemination of accurate and relevant scientific information and a space for diverging opinions and views. I shall now discuss some salient data regarding the need for sexual education. A survey of 1566 peri-urban (60 kilometres from Bangalore) students in Karnataka (NIMHANS and Belaku 2006) revealed the need for sex education that considers gender differences. When questioned about sources of reproductive and sexual health information, most girls cited female family members (mother 42%, older sister 24%) and friends 22%, teachers 14%. The picture was different for boys- friends 50%, relatives/neighbours 30% and teachers 20%. Media was cited as a source of information by many more boys. Television (boys 46%, girls 31%, science programmes (boys 27% and girls 15%) Action television (boys 18%, girls 3%), sex books (16% vs. 2.6%), sex films (12 vs.
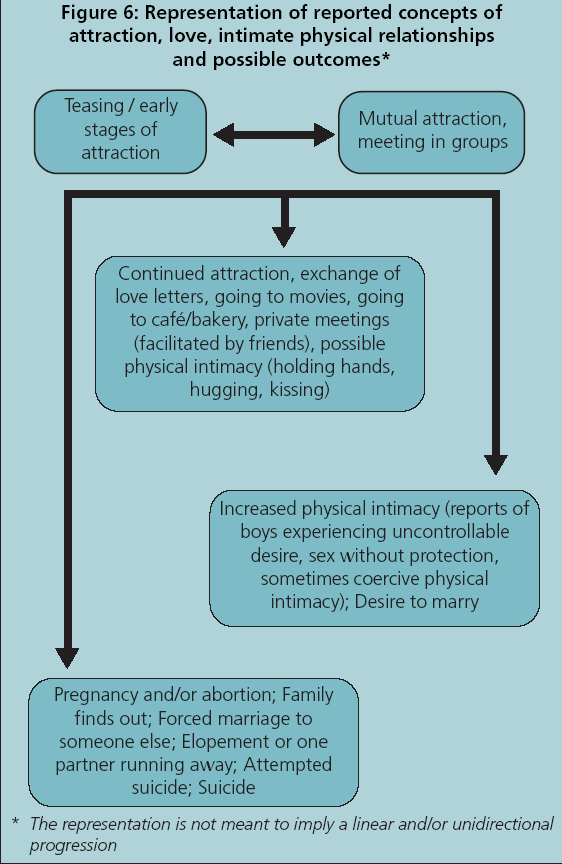
1%), posters (12 vs. 0.6 %) are mentioned by boys. Sex books may be cheap local language pornographic materials often with western graphic materials. We also found a range of grey literature, pseudo-scientific literature some written by bona fide medical specialists and others by self styled ‘sexologists.’ They contained Q & A on many sexual issues including many on premature ejaculation, masturbation, loss of strength. This was interspersed with titillating case studies. These magazines were not available in book stores but sold on pavements, streets, bus stands and railway stations. Often they had titles like “Ideal Husband and Wife.” Other favoured magazines such as Police News contained highly graphic descriptions of murder and rape. Sex films could be blue films or low budget films with high sexual content and violence. These media tended to reinforce boys anxieties and legitimise use of coercion and like coercion to pleasure. Key informants felt that in the three years that cable television had become available the students had become ‘fast.’ English language television had become accessible especially to boys; they reported watching a programme called Silk Stalking on AXN which had an opening shot of a woman putting on stocking. They also watched fashion TV. It is interesting that both key informants and boys find western television programmes and film ‘sexy’. There is little mention of the local language movies which have highly sexually suggestive dances. When questioned about their knowledge of pregnancy 73% girls and 50 % boys said they did not know. Of those who knew, boys commonly cite condoms (23%), followed by oral contraceptives (8%), abstinence and abortion (6%), and operation 4%. Girls had less knowledge about all methods except oral contraceptive (13%). Only 5% mentioned condoms, abortion and operation 3%, and abstinence 2%. Fourteen percent of boys and 2% o girls thought premarital sex was acceptable if the girl does not get pregnant. Analysis showed that the common sources of information had low association with accurate information about contraception. The sex educational programmes in schools do not consider this gender variation in the source of information among students. This finding also brings into question the acceptability of teachers conducting sex education programmes. The usual pattern is to assign sex education/family/life skills education to science teachers as they know how to teach biology. These teachers usually have little skill in communication or in discussing about intimate issues. The students concerns about why they feel a certain way, whether this is right or wrong, are seldom addressed. There is little space of debate and discussion, a space that many girl students felt they needed and to some extent was met by the study. The boys on the other hand, felt discussion about sex would arouse them and that such discussions were not necessary. This study included qualitative data that illuminated boy girl relationships. Students from rural area had more interactions with opposite sex, and these relationships were rarely platonic. Surprisingly, Valentine’s Day and Rose Day were very popular, students said that it acceptable to show your interest and love on this day. In a society that lacks a script for boy girl interaction, expression of love or interest, communication by notes and letters is common. Students also use popular love songs from films to communicate with person they are interested in.
Concepts of love and stages of love relationship are patterned (see figure above), teasing is a part of the initial stage, unwelcome or actions bordering or harassment seen as problematic by girls. Outcome of love relationships are usually negative and even life threatening. Girls receive little support from their families if they report teasing and harassment, instead they are scolded and beaten asked what they did to invite such attention. Parents threaten to take them out of school. Options for a girl in a serious relationship are few - if the boy too opts for marriage- elopement and marriage is one; or parents may coerce girls to marry a partner of their choosing. If the girl becomes pregnant she has a few choices – abortion is one, attempted suicide or suicide is another. Lack of social support is striking, media and adults reinforce the notion that a girl who has brought such dishonour to her family is better off committing suicide. This is the context of the debate over the need for sexual education. Recognizing the reality of the prevailing situation in the country, NACO prepared educational materials in 2007. Five (eventually 12) states banned it, and one sent it for review stating that sex education
encourages sexual permissiveness in children. NACO clarified that the material with pictures was meant for teachers of senior secondary schools. Still this was thought to be ‘too brazen and explicit” and it hurt people’s cultural sensitivity. A minister opined that sex education would create an “immoral society” and lead to a collapse of the education system. “The proposed sex education modules are an encouragement rather than education about sex,” he observed and called for boycotting central government schools if they took up sex education. The director took a strong stand and commented "Banning sex education is hypocrisy on their part. It is rubbish and totally nonsense that we don't need sex education. Our survey has shown that teenage boys are indulging in casual sex. Fifteen per cent of total deliveries in India involve teenage girls.” She warned that banning educational material would adversely affect poor students, who depend on schools to provide the right information. She went on to say, “If sex education is not imparted to children, they could make wrong decisions that could have an adverse impact on their future and health.”
A year later NACO brought a teachers handbook with out explicit pictures and words like intercourse, condoms, and masturbation. The director said that the issue was too important to take a strident tone. She thought the ‘middle path adopted by NACO would keep the dialogue going.
Thirty-three NGOs who reviewed the content felt that the study material is out of sync with the reality of adolescence. So cagey is the text about offending sensibilities that the chapter on conception doesn't even mention intercourse. One NGO reviewer noted that the section on prevention of HIV transmission does not mention condoms. Experts note that studies show adolescents are sexually active, not taking about sex safe is irrational. Asking them to abstain will make them curious and they will experiment.
Several prominent organizations have drafted a petition in which they provide ample documentary evidence and cite international agreements and rights and “the urgent revision of the AEP (Adolescent Education Programme) curriculum on sexuality education for all children to be reflective of the “best interests of the child” rather than proscribing narrow notions of morality, culture and tradition. This would be the first step in creating a comprehensive sexuality education that is gender-sensitive, age-specific and free from negative value judgments which is essential to help young people lead lives free of fear, disease and violence; and to enjoy physical and mental health and wellbeing.
Despite these set backs, NACO reports that condom sales increased by five per cent during the six months from April to September in 2008. This was attributed to extensive mass media campaign to promote condoms as a socially acceptable health product by encouraging discussion. TV and radio advertisements and mobile ringtone to promote the concept of safe sex reached nearly 150m adult men across India. Half a million people are reported to have downloaded this ring tone, which chants 'condom, condom condom'.
However, the director reported that the campaign to install condom vending machines at public places, including petrol pumps, subways and bus stops was not as successful. She said, "We were a little mistaken in that effort. In our excitement we installed machines at places which were too public….For example, rather than installing the systems on the roadside, we should have done so in places like toilets to lend some privacy to a potential customer.”
NACO is still wary of extending “safe-sex" campaign to include the gay community directly. The director said, "There is no point openly promoting the use of condoms by gays at present as it may provoke a backlash. We, however, work through a range of NGOs working on the ground which promote safe-sex for homosexuals."
Therefore, with condoms, it is one step forward and two step backwards. Shifting policies in response to internal and external pressure and the continued reluctance to promote condoms undermine the development of a clear policy.
Emergency Contraceptives
Methods that need to be used correctly and consistently, that require engagement, dialogue, negotiation, and skill building where the choice of use lies with the person find little emphasis in the Indian family planning programme. In the current programme that promotes family planning in the context of reproductive and child health and rights, promotion of dual purpose condom use is mentioned. Emergency contraceptive (EC) are also advocated for unprotected intercourse and for failed dual purpose condom use (torn condom -Nirodh). The possibility of the condom not working, of it slipping, tearing is a recurrent unrealistic fear that is bolstered by such statements. This shows that the state is also not convinced of the efficacy of condoms. On the other hand, the efficacy of medications is seldom questioned. Emergency contraceptives have received special treatment, The Drugs ad Magical Remedies Act has been reviewed on a case by case basis to allow direct advertisement by the private sector, and these advertisements are being aired on the television and displayed on the back of autorickshaws. A news item last month (Chaudhuri 2009) noted that though emergency contraception was made available over the counter to prevent unnecessary abortions, women and girls were using it repeatedly - in place of regular contraceptives resulting in serious reproductive problems. This should be a serious concern in a country where more that half the women are anaemic. It is not surprising women/girls are using EC as a primary contraceptive as advertisements such as the one given below can easily be misinterpreted to mean the EC is a contraceptive. Further this misuse should have been anticipated as women /girls have long been used to taking hormonal pills to postpone menstrual periods during religious and social function.
i-pill emergency contraceptive pill. Just one pill within 72 hours of unprotected sex is all it takes to prevent a possible pregnancy and a traumatic abortion. Because prevention is better than abortion. Isn’t it?
This news story has not been followed up and there has been no public outcry. Viagra, Generics and Ayurvedic medicines
The Google search engine brings up 63,000, 000 hits for the word Viagra on the World Wide Web and 720,000 on Indian web pages. This includes other not necessarily biomedical products such as Ayurvedic Nights and Vita Ex Gold. It is said to be the most widely advertised substance on the internet, and the subject of a large proportion of spams. In 2005 Microsoft and Pfizer team up to file lawsuits against spammers as well as the companies they advertise, especially if they use the term Viagra in there domain name.
Virility, potency, energy, strong sex drive, vigour are associated with sexual prowess as well being potent in sense of having power, and ability to influence. The capacity to achieve an erection or to reach orgasm is also seen as symbolof manly courage and strength. Conversely the term impotence not only indicates the inability to have an erection but also powerless and ineffective. The term erectile dysfunction does not have these implicit meaning or symbolism, it is patently a medical condition. In keeping with the ayurvedic concept of the importance of semen men are concerned with sexual performance. A preparation by a reputable Ayurvedic pharmaceutical company, Baidyanath, called Vita – Ex Gold is widely used. It is said to contain gold and silver bhasma (ashes) and 14 potent herbs that ‘increase pleasure and heighten happiness for a longer period.’ It recharges, reactivates, refreshes vitality and vigour Male sex workers (kotis) that we interviewed reported that they ask their attractive clients, the ones that they are attracted to, to take this preparation so that they can ‘enjoy’ for a long time.
The information provided in the website is very much in the holistic Ayurvedic tradition, it emphasises psychological origin of sexual problems. It states that sex is an integral part of daily life (dinacharya). Frequency of sex depends on constitution of the individual. The website recommends Vajikaran therapy (virlification) - that part of Ayurveda which enhances male fertility and potency that for more and better sex. However, it points out that any misuse of the same may open up a deluge of emotional and psychological complications. For best results, it is recommends that the partners should be physically, emotionally and spiritually involved with each other. Further, it explains that touch, smell, food, music and ambience play a vital role in developing, increasing and prolonging intimacy
Premature ejaculation is identified as the most common problem that shortens duration of intimacy and hinders the couple from attaining orgasm. The most frequent cause of unsatisfactory erection or sexual deficiency is identified as psychological, nonetheless men are advised that pathological conditions need to be ruled out. It states that even after treatment the patient’s self confidence needs to be restored. It notes that with current hectic lifestyle and advancing years the male desire for sexual intercourse tends to taper off early and sexual intimacy tends to become unsatisfactory. Ayurvedic medicines can rectify this. Medicines are taken with fruit juice, warm milk, honey and other health enhancing substances.
Thus the medication is only a part of the strategy to improve, strengthen sexual function. In this view the problem is located in the person and the social situation. Pre- Viagra, in biomedicine the problem was thought to be largely psychological and came under the purview of psychologists and psychiatrists Physical interventions such as penile insertions and vacuum pump were seldom used. In contrast the current biomedical construction of erectile dysfunction pays little attention to factors that lie outside the body, as it is treatable with medication regardless of the cause be it physical, psychological, interpersonal or familial (Mosher 1991, p 16 cited in Potts p 490). It takes a reductionist view of the body and the notion that a healthy functioning male body must be capable of producing a normal erection that delivers sexual satisfaction to the partner (via penetrative sex) to both the man and his (female) partner.
Medicalisation a major intellectual trend of the 20th and 21st century and ncreasing medical modes of thought dominate the discourse on sexuality, and medical authority over many
domains is unquestioned. Medicalisation privileges a narrow concept of ‘normal’ and conformity to it is valued, and is largely not tolerant of divergence and shies away from accepting a range of normality. Anything outside this strict definition of normal is pathological, a disorder. Some challenge this notion of sexual dysfunction, they believe erectile dysfunction it is a natural aging process, and one learns to live with it (very much the tradition Indian view). Some state that advertising has caused a sense of inadequacy in older men. On the other hand, medicalisation of the unpleasant /unpalatable, conditions such as impotence makes them more acceptable. While, medicalisation especially in terms of prevention takes the pleasure out of things. Pfizer deemed 2005 as an opportune time to launch Viagra in India when India having signed various trade agreements had to fall in line with the patent regime. Earlier Indian patent laws did not recognise product patents, only process licenses. Reverse engineering was used to develop different processes for producing the same product. Hence, generic Viagra, i.e. sildenafil citrate produced by ‘multiple cost based local competitors’ were already present in the market. As India is considered to be lucrative markets with an estimated 70-90 men suffering from ED and market research suggested a demand for ED medication in the grey market and Pfizer planned to convert this demand into sales of the ‘original’ product. Pfizer imported Viagra, with its distinctive hologram from France and launched it in 30 cities. A tablet of 100mg was priced at about Rs. 600 as compared to Rs. 25 for the generic version. In spite of this higher price, Pfizer reported that sales in the first month far exceeded expectation and that it had succeeded in capturing 1.8% of the market worth Rs. 800 m ($16m). Pfizer’s strategy was to promote Viagra to doctors (urologists, endocrinologists, psychiatrists and STD specialists) and to inform them that the drug was available at a chemist located close to their clinic/hospital. Sales were higher in top rung cities, and there was hope that this strategy would ‘yield more prescriptions in the ensuing years’ in other cities as well. The strategy used by Pfizer was to educate men, potential patients, and doctors about ED, by distributing ‘scientific’ information. Pfizer also tracked 750 prescriptions given by doctors. With initial success Pfizer announced that it was confident of capturing 10% of the market in two years. However things have not gone well for Viagra in the Indian market, the company has been reticent about Viagra sales figures since March 2006. Local competition has been stiff, with the top three players controlling 65% of the market share. Apart from this, inexpensive counterfeit drugs have also been packaged and sold as, Viagra. And since 2007 the ED market in India has had a sluggish growth.
In a television programme organised to mark the tenth anniversary Viagra, panellists remarked that sexuality in India is either giggled about or frowned at and there are no mature debates on it. One asserted that sexual culture is related to youth culture and marginalises adults — people who are post 45. That such adults could also want to enjoy a sex life is not even considered a possibility in mainstream society.
An urologist agreed with this point of view, he remarked that patients who were to undergo prostate surgeries, when warned that their sex life might diminish, said that they are well past that. "But we have to give them the message that it’s not over, they are still young enough to enjoy sex," he said. “You've got to give the person a good, healthy life, not just treat their conditions," he explained.
Ironically he added thanks to the discovery of the co-relation between Erectile Dysfunction and heart attacks, more and more doctors are getting involved in dealing with their patients’ sexual histories.
The above account gives a good indication of Pfizer’s market strategy and its attempt to redefine the sexuality of older men. Even though there have been several reports of the deaths, 109 in Britain and other health problem related to Viagra use, the misuse of Viagra and the dangers there in this has not entered the public discourse.
Viagra for women: new markets
Of recent sildenafil has been found to relieve antidepressant related sexual dysfunction in women. Antidepressants that control the availability of the brain chemical serotonin are the most commonly prescribed drug for adults in the US, it is estimated that 160 million prescriptions are written per year. It is estimated that 30 to 70% of these women suffer from sexual dysfunction and many stop treatment for this reason. It is interesting to examine how this study was conducted. This prospective, parallel group, randomized, double-blind, placebo-controlled, 8-week consisted of 49 eligible patients in the experiment group –who received sildenafil and 49 to control group who received a similar blue pills. Subjective perception of sexual desire, physical signs of arousal, enjoyment, changes in pain and discomfort and something called partner (issues? problems?) were recorded. Women who took Viagra reported significantly1 more side effect than in the control group. Both groups improved but the reported change in the women taking Viagra was significantly more/better. It is not clear what this better is as the authors (Nurnberg et al) note serious limitations.2 Yet they go on to conclude that seems clear that effective evidence-based treatments for treatment-associated adverse effects can lead to improved outcomes for major depressive disorder and other conditions requiring extended medication treatment.
It is stated that the this study was supported by an independent investigator-initiated grant from Pfizer Inc provided sildenafil and matching placebo and had no other role in the study.
Campaigns Even after more than sixty years freedom from the British rule, Indian middle class is still burdened by Victorian puritanical outlook and morality. This colonial legacy, combined with reconstructed notions of the golden Indian past, has lead to rejection of the plurality, diversity and syncretic nature of the Indian society. This vocal group who are in the forefront of policy making, planning and implementation have a disproportionate impact. The diversity of views held by the silent majority is masked. People hesitate to question, or to express divergent
1 Headaches (43%vs. 27%), flushing (27%vs. 0%), transient changes in vision (14% vs. 2%). Nausea (16% vs. 2%) and anxiety (6% vs. 2%) were common in the control group
2 Lack of biological criterion for female sexual dysfunction, assessment instruments with high correlation, and use of analysis-of-variance models for samples assigning integers to ordinal categories of an outcome measure when the phenomenon in question has an underlying continuous scale), relied on scoring based on subjective responses to different questions for men and women, so the roles of expectations and adverse effects, as well as treatment response, influencing subjective report measures.
views for fear of being branded as immoral, unpatriotic or not subscribing to the Indian tradition. Space for dissention has reduced. At the same time, increasingly women are being educated, getting well paying jobs, becoming more mobile, dressing differently, and being more assertive. I would like to present a campaign that has effectively used information technology to rapidly mobilise an otherwise apathetic educated elite. First some background. Recently women in a pub were attacked (beaten and some injured quite badly) in full view of the public and recorded by television cameras and broadcast to the whole nation a few hours after the incident. The police did not respond swiftly, and the women were blamed for being in the pub. The leader of the right wing group, Ram Sene, said that these women were not behaving the way ‘good’ women should, that they should been at home learning to cook for their husbands. This group like many others of the ilk have been protesting the celebration of Valentines Day and the expression of love between people of the opposite sex. This year the group threatened to force unmarried heterosexual couples seen in public together to marry. In addition women who were out on their own, especially if they were clothed in non-Indian clothes were attacked. There seemed to be an ethnocentric element to this as well, women who could not speak the state language were particularly targeted. In other areas there have been attempts to curtail interaction (threats and violence) between youth of different religious persuasions; conservative elements in all the religions are tacitly supportive of this action. The media coverage of these incidents labelled it as Talibanisation. This caused more furore with people protesting, perhaps rightly, that in a Taliban country such debate would not be possible.
A young IT professional formed a group with membership on the Facebook social network website. They called themselves The Consortium of Pub-going, Loose and Forward Women, thus, effectively sabotaging the people who would potentially label them. This subvertive tactic has been effectively used by other stigmatised groups. They asked all those who did not agree with the action of the Ram Sene to send a pink chaddi (knickers) to the leader of the group on Valentine’s Day3. The originator of the campaign, Nisha Susan "The chaddi is slang for right-wing hardliners (shorts is part of the uniform) and the saffron agenda, while pink stands for things that are frivolous. The combination is offensive." Others have pointed out that pink also symbolises love, it is also the symbol of the gay movement and also stands for a soft communist (not so red). The aim was to reclaim Indian culture one chaddi at a time.
The campaign has been surprisingly successful, over 800 having joined the facebook group. Collection points were organised and people dropped of packages containing pink chaddi (s) and a valentine card. The campaign caught media attention and received wide publicity. Even older women and men who would probably never go to a pub joined, some said that they feared what would happen to their daughters in future, and this motivated them to participate.
The Ram Sene did not appreciate being ridiculed and predictably labelled the campaign as being un-Indian and not befitting Indian women. As a follow up the campaign to highlight the diversity and beauty of Indian culture, the campaign is asking Indians to make short videos of what they think of Indian culture. These videos would be hosted on You Tube.
3 Many have criticised the commercialisation and commoditisation of days including Valentines Day, the Hindu right wing sees at an imposition of western culture.
The Alternative Law Forum which has been at the forefront of fighting for rights, including those of the sexual minorities have started another campaign called Fearless Karnataka. It is working towards reclaiming lost spaces – Take back the night, take back the street. It is organising to protest against these incidents, show solidarity with the ‘victims’ and raise awareness of the public by involving bystanders.
The People’s Health Movement has brought together a wide coalition of marginalised groups to contribute to the gender and health section of the People’s Health Manifesto 2009, Health for All Now. The manifesto has come out just in time for the Indian general elections. Demands include:
Gender and Health
• Abolish all coercive laws, policies and practices that violate the reproductive and
democratic rights of women, including the two child norm.
• Stop coercion in the use of contraception; make user-controlled contraceptives
• Ensure safety, transparency and accountability in all clinical trials, and guarantee that
the post-trial benefits of research are made available to women even from marginalized groups. Ensure disclosure of funding and of potential conflict-of-interest in all clinical trials, medical research and publications.
• Make mandatory the inclusion of women’s organizations and women’s health
advocates on ethics committees, from national to local and institutional level.
• Recognize violence against women as a public health issue and ensure provision of
necessary services. Ensure prosecution and conviction of violators of the Prevention of Domestic Violence against Women and Girls Act as also the PCPNDT Act.
• Include the topic of “Violence against women” and “sexuality and gender” as part
medical and paramedical curricula to equip medical professionals deal in a sensitive manner with survivors of violence, including domestic violence. Train forensic experts on the social aspects of sexual assault, and rape, collection and retention of proof in cases of individual or mass sexual violence.
• Repeal Section 377 of the Indian Penal Code, and other laws, policies and practices
that discriminate on the basis of sexuality.
This manifesto is being distributed to all the political parties and their endorsement is being sought.
The Condoms and Viagra Paradox
It is easy to note the differences between condoms and Viagra. Condoms have been around for a long time, they are essentially mechanical devices, and they are not glamorous. Condoms also have negative association with sexually transmitted diseases, and relationships outside marriage (‘illicit relationships’). Condoms are for prevention and not pleasure. Although condoms help to prevent conception and sexually transmitted infections, the dual use is not emphasised. While Viagra (or Viagra clones) promises pleasure, increase in self
esteem, bolsters self image and magical swift action. It is backed by slick advertising and marketing. It is prescribed by doctors whose authority over the sexual domain is deepening and is increasing unquestioned. Apart from the above, the nature of condom use and Viagra are essentially different. For condoms to work it needs to be used correctly and consistently, such consistent behaviour needs support and reinforcement which is sadly lacking. Correct and consistent use of condom needs the partners to be able to talk about sex, to discuss, negotiate, this would mean an equal relationship. Unfortunately this is not the case. The persistence of the Victorian morality among the Indian middle classes who have disproportionate influence on policy formulation and programme implementation has greatly hampered the propagation of condoms. Policies in ‘developing’ countries are also greatly influenced by other agencies such as The World Bank4, IMF etc. and the process of globalisation that transforms national institutions may be seen as a form of neo-colonialism. This is visible in the condom debate, the policies made by PEPFAR and the pressure on India to change its patents laws and comply with the patent regime. There is also a conflation of science and religion, as is seen in the propagation of Vedic sciences (which seems apart from the scientific discoveries made in India) and the recent pronouncements by the pope on the efficacy of condom in cubing the spread of HIV in Africa. This again was backed by Green who works in a prestigious university and had a high position in the previous US government. Although Green’s statement are more nuanced and couched in caveats, the reading in the media particularly those affiliated to the church have been totally anti-condom. After quoting Green, The Catholic Secular Forum makes this observation, “If condoms were the answer, then why is it that New York City, which under Mayor Michael Bloomberg has given away tens of millions of free condoms, has (sic) an HIV rate three times the US national average? Furthermore, the promiscuous distribution of condoms in New York has coincided with a spike in sexually transmitted diseases of all sorts.” As for Viagra, it is not doing well in the Indian market despite the new regulations. Generic sildenafil as well as ayurvedic and other preparations are able to cope better with Indian market situation. It is ironic that after the global economic meltdown, India was lone voice rooting for ‘free trade,’ the countries that had hitherto advocated free market and privatisation were firmly for protectionism and government regulation. A new world order seems to be developing.
4 World Bank policies have been largely responsible for the dismantling of the Indian public health system.
REC Reference No. 10/H1102/30 A feasibility study evaluating the comparative effects of statins using your GP’s medical records Information Sheet You are being invited to take part in a research study. Before you decide, it is important for you to understand why the research is being done and what it will involve. Please take time to read the following information
Connecticut Parkinson's Working Group Newsletter Special Edition October 2003 ===================================================================Support for this newsletter comes from Pfizer Corporation and the donors to CPWG. Editor: Stan Wertheimer stan.wertheimeratgmail.comInterview Editor: Jeff Lincoln===================================================================This special edition of
 Concepts of love and stages of love relationship are patterned (see figure above), teasing is a part of the initial stage, unwelcome or actions bordering or harassment seen as problematic by girls. Outcome of love relationships are usually negative and even life threatening. Girls receive little support from their families if they report teasing and harassment, instead they are scolded and beaten asked what they did to invite such attention. Parents threaten to take them out of school. Options for a girl in a serious relationship are few - if the boy too opts for marriage- elopement and marriage is one; or parents may coerce girls to marry a partner of their choosing. If the girl becomes pregnant she has a few choices – abortion is one, attempted suicide or suicide is another. Lack of social support is striking, media and adults reinforce the notion that a girl who has brought such dishonour to her family is better off committing suicide. This is the context of the debate over the need for sexual education. Recognizing the reality of the prevailing situation in the country, NACO prepared educational materials in 2007. Five (eventually 12) states banned it, and one sent it for review stating that sex education
encourages sexual permissiveness in children. NACO clarified that the material with pictures was meant for teachers of senior secondary schools. Still this was thought to be ‘too brazen and explicit” and it hurt people’s cultural sensitivity. A minister opined that sex education would create an “immoral society” and lead to a collapse of the education system. “The proposed sex education modules are an encouragement rather than education about sex,” he observed and called for boycotting central government schools if they took up sex education. The director took a strong stand and commented "Banning sex education is hypocrisy on their part. It is rubbish and totally nonsense that we don't need sex education. Our survey has shown that teenage boys are indulging in casual sex. Fifteen per cent of total deliveries in India involve teenage girls.” She warned that banning educational material would adversely affect poor students, who depend on schools to provide the right information. She went on to say, “If sex education is not imparted to children, they could make wrong decisions that could have an adverse impact on their future and health.”
A year later NACO brought a teachers handbook with out explicit pictures and words like intercourse, condoms, and masturbation. The director said that the issue was too important to take a strident tone. She thought the ‘middle path adopted by NACO would keep the dialogue going.
Thirty-three NGOs who reviewed the content felt that the study material is out of sync with the reality of adolescence. So cagey is the text about offending sensibilities that the chapter on conception doesn't even mention intercourse. One NGO reviewer noted that the section on prevention of HIV transmission does not mention condoms. Experts note that studies show adolescents are sexually active, not taking about sex safe is irrational. Asking them to abstain will make them curious and they will experiment.
Several prominent organizations have drafted a petition in which they provide ample documentary evidence and cite international agreements and rights and “the urgent revision of the AEP (Adolescent Education Programme) curriculum on sexuality education for all children to be reflective of the “best interests of the child” rather than proscribing narrow notions of morality, culture and tradition. This would be the first step in creating a comprehensive sexuality education that is gender-sensitive, age-specific and free from negative value judgments which is essential to help young people lead lives free of fear, disease and violence; and to enjoy physical and mental health and wellbeing.
Despite these set backs, NACO reports that condom sales increased by five per cent during the six months from April to September in 2008. This was attributed to extensive mass media campaign to promote condoms as a socially acceptable health product by encouraging discussion. TV and radio advertisements and mobile ringtone to promote the concept of safe sex reached nearly 150m adult men across India. Half a million people are reported to have downloaded this ring tone, which chants 'condom, condom condom'.
However, the director reported that the campaign to install condom vending machines at public places, including petrol pumps, subways and bus stops was not as successful. She said, "We were a little mistaken in that effort. In our excitement we installed machines at places which were too public….For example, rather than installing the systems on the roadside, we should have done so in places like toilets to lend some privacy to a potential customer.”
NACO is still wary of extending “safe-sex" campaign to include the gay community directly. The director said, "There is no point openly promoting the use of condoms by gays at present as it may provoke a backlash. We, however, work through a range of NGOs working on the ground which promote safe-sex for homosexuals."
Therefore, with condoms, it is one step forward and two step backwards. Shifting policies in response to internal and external pressure and the continued reluctance to promote condoms undermine the development of a clear policy.
Emergency Contraceptives
Concepts of love and stages of love relationship are patterned (see figure above), teasing is a part of the initial stage, unwelcome or actions bordering or harassment seen as problematic by girls. Outcome of love relationships are usually negative and even life threatening. Girls receive little support from their families if they report teasing and harassment, instead they are scolded and beaten asked what they did to invite such attention. Parents threaten to take them out of school. Options for a girl in a serious relationship are few - if the boy too opts for marriage- elopement and marriage is one; or parents may coerce girls to marry a partner of their choosing. If the girl becomes pregnant she has a few choices – abortion is one, attempted suicide or suicide is another. Lack of social support is striking, media and adults reinforce the notion that a girl who has brought such dishonour to her family is better off committing suicide. This is the context of the debate over the need for sexual education. Recognizing the reality of the prevailing situation in the country, NACO prepared educational materials in 2007. Five (eventually 12) states banned it, and one sent it for review stating that sex education
encourages sexual permissiveness in children. NACO clarified that the material with pictures was meant for teachers of senior secondary schools. Still this was thought to be ‘too brazen and explicit” and it hurt people’s cultural sensitivity. A minister opined that sex education would create an “immoral society” and lead to a collapse of the education system. “The proposed sex education modules are an encouragement rather than education about sex,” he observed and called for boycotting central government schools if they took up sex education. The director took a strong stand and commented "Banning sex education is hypocrisy on their part. It is rubbish and totally nonsense that we don't need sex education. Our survey has shown that teenage boys are indulging in casual sex. Fifteen per cent of total deliveries in India involve teenage girls.” She warned that banning educational material would adversely affect poor students, who depend on schools to provide the right information. She went on to say, “If sex education is not imparted to children, they could make wrong decisions that could have an adverse impact on their future and health.”
A year later NACO brought a teachers handbook with out explicit pictures and words like intercourse, condoms, and masturbation. The director said that the issue was too important to take a strident tone. She thought the ‘middle path adopted by NACO would keep the dialogue going.
Thirty-three NGOs who reviewed the content felt that the study material is out of sync with the reality of adolescence. So cagey is the text about offending sensibilities that the chapter on conception doesn't even mention intercourse. One NGO reviewer noted that the section on prevention of HIV transmission does not mention condoms. Experts note that studies show adolescents are sexually active, not taking about sex safe is irrational. Asking them to abstain will make them curious and they will experiment.
Several prominent organizations have drafted a petition in which they provide ample documentary evidence and cite international agreements and rights and “the urgent revision of the AEP (Adolescent Education Programme) curriculum on sexuality education for all children to be reflective of the “best interests of the child” rather than proscribing narrow notions of morality, culture and tradition. This would be the first step in creating a comprehensive sexuality education that is gender-sensitive, age-specific and free from negative value judgments which is essential to help young people lead lives free of fear, disease and violence; and to enjoy physical and mental health and wellbeing.
Despite these set backs, NACO reports that condom sales increased by five per cent during the six months from April to September in 2008. This was attributed to extensive mass media campaign to promote condoms as a socially acceptable health product by encouraging discussion. TV and radio advertisements and mobile ringtone to promote the concept of safe sex reached nearly 150m adult men across India. Half a million people are reported to have downloaded this ring tone, which chants 'condom, condom condom'.
However, the director reported that the campaign to install condom vending machines at public places, including petrol pumps, subways and bus stops was not as successful. She said, "We were a little mistaken in that effort. In our excitement we installed machines at places which were too public….For example, rather than installing the systems on the roadside, we should have done so in places like toilets to lend some privacy to a potential customer.”
NACO is still wary of extending “safe-sex" campaign to include the gay community directly. The director said, "There is no point openly promoting the use of condoms by gays at present as it may provoke a backlash. We, however, work through a range of NGOs working on the ground which promote safe-sex for homosexuals."
Therefore, with condoms, it is one step forward and two step backwards. Shifting policies in response to internal and external pressure and the continued reluctance to promote condoms undermine the development of a clear policy.
Emergency Contraceptives