Primary Tracheomalacia T h o m a s H . Cogbill, M . D . , Frederick A . M o o r e , M . D . , Frank J . A c c u r s o , M . D . , a n d J o h n R. Lilly, M . D .
ABSTRACT Tracheomalacia is a rare congenital
malformation of the tracheobronchial cartilages in cheomalacia have been seen at our institution which the supporting cartilaginous rings permit ex-
over the past four years. The clinical symptoms
piratory collapse of the airway. The condition is usu-
of the 4 patients were remarkably similar and
ally mild and self-limited. There is a severe variant,
highly distinctive. Moreover, therapeutic inter-
however, that is life-threatening and warrants sepa-
vention was eventually identical in each in-
rate categorization. Four children with severe pri-
stance. The purpose of this article is to review
mary tracheomalacia were treated recently. The clin-
briefly the clinical features in the 4 patients, to
ical symptoms, diagnostic findings, and eventual describe the diagnostic process, and to discuss treatment of these patients were highly distinctive the therapeutic management of infants with se-and almost identical in all 4, permitting us to make
the following observations: (1) primary severe tracheomalacia must be suspected in infants with
unexplained respiratory distress manifested by Patient 1 stridor and cyanosis; (2) symptoms are not present at
A 10-week-old female infant was hospitalized
birth but appear insidiously after the first weeks of
for progressive stridor and respiratory distress
life, are markedly aggravated by respiratory tract in-
over a 3-week period. On admission she had
fections, and are made worse by agitation; (3) bron-
expiratory stridor, wheezing, and intercostal re-
choscopy is essential for definitive diagnosis and traction at rest. Symptoms became worse with should be employed early in the diagnostic process;
agitation. Chest roentgenogram and barium
(4) tracheostomy is probably essential in most in-
swallow were normal. At bronchoscope exami-
stances; and (5) resolution, although spontaneous,
nation, expiratory collapse of the mainstem
does not occur until after 2 years of age.
bronchi and distal trachea was noted, as well as indistinct tracheal rings. A small, clinically un-
Primary tracheomalacia is a rare disease of in-
important subglottic mass was also visualized.
fancy that is believed to be due to immaturity of
Postoperatively, stridor gradually became more
the tracheobronchial cartilage [1]. Tracheal nar-
severe and was not responsive to racemic epi-
rowing occurs with expiration and causes nephrine, isoetharine inhalations, and par-stridor, cyanosis, and respiratory distress. An-
enteral prednisolone. At repeat bronchoscopic
teroposterior tracheal collapse and indistinct examination five days later, the narrowing of tracheobronchial rings are visualized broncho-
the distal trachea and mainstem bronchi had be-
scopically. The disease is self-limited, generally come worse. There was now severe edema of resolving within the first 2 years of life [1]. the tracheobronchial mucosa and moderate There are different degrees of clinical severity,
bronchial secretions, which grew parainfluenza
however, and a high mortality has been associ-
ated with the more severe variants [2, 3].
Despite the tracheostomy, the patient's respi-
rator}' status deteriorated. Positive-pressure ventilation with pressures of 60 cm H 2 0 was necessary to provide an arterial oxygen tension
From the Departments of Surgery and Pediatrics, University
of 45 mm Hg on 100% forced inspiratory oxy-
of Colorado Health Sciences Center, Denver, CO.
gen. Cardiopulmonary arrest ensued, which
was reversed only by emergency rigid bron-
Address reprint requests to Dr. Cogbill, Department of Surgerv, Gundersen Clinic, 1836 South Ave, La Crosse,
choscopy through the tracheostomy wound.
The bronchoscope mechanically opened the al-
539 Cogbill et al: Primary Tracheomalacia
most totally collapsed mainstem bronchi, thus bronchoscopic examination that showed the permitting aeration of the distal tracheobron
tracheomalacia to be moderately improved. The
Over the next 11 days, the patient's symp
toms improved. Bedside bronchoscopy with Patient 3 tracheobronchial aspiration of thick sputum was A 21-month-old boy was hospitalized for recurrequired on numerous occasions. Over the fol
rent upper respiratory tract infections, cyanotic
lowing weeks, the airway lumen gradually di
episodes, apnea, and failure to thrive. At 6
lated because of resolution of mucosal edema weeks of age he was hospitalized for persistent and inflammation. The patient was removed cough, expiratory stridor, and cardiomegaly. A from positive-pressure ventilation and subse
diagnosis of "laryngomalacia" was made. Sev
quently discharged. Ten months later, bron-
eral subsequent hospitalizations for respiratory
choscopic examination demonstrated some distress and viral pneumonia occurred over the improvement of tracheomalacia and nearly next 18 months. complete resolution of the subglottic tumor. At
On admission the patient exhibited moderate
2 years of age, the patient had a bronchoscopic respiratory distress with a respiratory rate of 40 examination, the findings of which were almost breaths per minute, and there was perioral normal. The tracheostomy tube was success
cyanosis. Cardiomegaly and enlargement of the
fully removed, and the patient has been well for pulmonary artery were noted on the chest the past 5 months.
roentgenogram. Progressive carbon dioxide retention finally prompted nasotracheal intuba
tion. At subsequent bronchoscopic examina
A 3-month-old male infant was hospitalized for tion, severe tracheomalacia combined with failure to thrive and frequent cyanotic episodes. minimal subglottic stenosis was seen, and a traSymptoms began at 16 days of age with crying cheostomy was done. Postoperatively the paspells followed by choking and expiratory tient improved moderately, and congestive stridor. On examination the patient had expira
heart failure was treated successfully by diuret
tory stridor and grunting with severe chest re
traction. The respiratory rate was 52 breaths per
minute. Chest roentgenogram and barium swal
months over the next 18 months. Tracheal mat
low were normal. At bronchoscopic examina
uration was first noted when the patient was 33
tion there was nearly total collapse of the distal months old. Subsequently the tracheostomy trachea, and the tracheal rings were indistinct. tube was removed successfully. At ЗУг years of
A tracheostomy was done. Postoperatively the age, the patient has minimal symptoms. His
patient improved moderately but continued to heart is entirely normal. have respiratory distress with wheezing and copious tracheal secretions that only gradually Patient 4 improved.
A 36-week-old premature female infant was
At 10 months of age, the patient had a bron
seen with progressive cyanosis, apnea, and ex
choscopic examination that showed almost piratory stridor. Nasotracheal intubation was identical findings. For reasons that are unclear, eventually necessary. At bronchoscopic examithe tracheostomy tube was removed subse
nation, findings were severe tracheomalacia
quently at another institution. The patient did with marked tracheal collapse and mainstem well for 2 months and then had a sudden respi
bronchial narrowing. The patient could not be
ratory arrest. Emergency tracheostomy through
removed from controlled ventilation and devel
the old tracheostomy wound saved his life.
oped congestive heart failure resistant to di-
At 23 months of age, the patient developed a goxin and furosemide. A tracheostomy was
viral pneumonia that required mechanical venti
done, and there was gradual improvement. She
lation, theophylline, isoetharine, and postural was discharged on mask oxygen. She develdrainage. At 26 months of age, he had another
oped a mild upper respiratory tract infection 4
Clinical Data on 4 Patients with Severe Primary Tracheomalacia3
months later and died at home of respiratory
there is a definite worsening of symptoms with
crying and agitation, an observation that has
The courses of all 4 patients are summarized
not been reported previously. Each of our pa-
tients required sedation; in fact, Patient 1 re-quired temporary paralysis to control agitation
As noted earlier, tracheomalacia is characterized
Symptomatology is also markedly aggravated
by abnormal tracheal collapse secondary to in-
by respiratory tract infection. Three of our pa-
adequate supporting cartilaginous and myo-
tients had serious clinical deterioration during
elastic elements [1]. The condition has been di-
otherwise mild flu-like illnesses, and 1 died con-
vided into primary (congenital) and secondary
sequently. Presumably, the tracheobronchial lu-
(acquired) subgroups. Primary tracheomalacia men, already narrowed by tracheomalacia, be-is probably due to immaturity of the tracheo-
comes further compromised by inflammation.
bronchial cartilage [1]. Secondary tracheomala-
In addition, tracheobronchial secretions under
cia is due to degeneration of previously normal
these circumstances may be cleared less effec-
tracheal cartilages resulting from inflammatory
processes [4-7], extrinsic vascular compression
Baxter and Dunbar [1] employed fluoroscopy
[8, 9], bronchial neoplasms [5, 9], and tracheo-
and lateral inspiratory and expiratory chest
roentgenograms to establish the diagnosis of
There appear to be two distinct types of pri-
tracheomalacia. In our patients static inspiratory
mary tracheomalacia: the common or mild vari-
and expiratory chest roentgenograms were nor-
ant and an unusual, severe form. In 1963 Baxter
mal, and the critical clinical status of these in-
and Dunbar [1] reported 21 patients with pri-
fants precluded the use of fluoroscopy. We be-
mary tracheomalacia who displayed both types
lieve that bronchoscopy is absolutely necessary
of clinical symptomatology. The mortality de-
for definitive diagnosis. Also, because of the
pended upon the severity of the disease; there
safety of present-day equipment, this technique
were no deaths in patients with the mild form.
should be utilized early in the diagnostic pro-
Mortality in severe tracheomalacia has been re-
There is little information about the treatment
Severe primary tracheomalacia has an insidi-
of severe forms of tracheomalacia. Most of the
ous onset in an otherwise healthy infant, with patients reported by Cox and Shaw [11], Levin the appearance of progressively noisy respira-
and colleagues [12], and Baxter and Dunbar [1]
tions, episodic cyanosis, increased respiratory required no formal therapy, since they had the rate, intercostal retractions, and, finally, obvi-
mild form of the disease. In treatment of severe
ous stridor. The stridor is most noticeable dur-
forms, Picot and associates [3] recommended
ing expiration when maximal tracheobronchial hospitalization, oxygen, and, occasionally, tra-collapse normally occurs. In our experience cheostomy. Treatment with oxygen, postural
541 Cogbill et al: Primary Tracheomalacia
drainage, percussion, and frequent endotra-
cheal suctioning was unsuccessful in our pa-
1. Baxter JD, Dunbar JS: Tracheomalacia. Ann Otol
tients, and tracheostomy was ultimately neces-
2. Agosti E, DeFilippi G, Fior R, et al: Generalized
familial bronchomalacia. Acta Paediatr Scand
The efficacy of tracheostomy appears to be a
consequence of the tube's stenting effect on the
3. Picot C, Monnet P, Bethenod M, et al: La
semiflaccid trachea. More effective tracheo-
tracheomalacie du nourrisson. Arch Fr Ped
bronchial aspiration is also provided, but this is
probably less important. That tracheostomy is
4. Feist JH, Johnson TH, Wilson RJ: Acquired
not curative, or may not even prevent subse-
tracheomalacia: etiology and differential diag-
quent respiratory embarrassment in the face of
5. Johnson TH, Mikita JJ, Wilson RJ, et al: Acquired
intercurrent respiratory illness, was well illus-
trated in our small series. The probable mechan-
6. Jokinen K, Palva T, Sutinen S, et al: Acquired
ism for exacerbation of symptoms in this situa-
tracheobronchomalacia. Ann Clin Res 9:52, 1977
tion is inflammatory narrowing of the mainstem
7. Nuutinen J: Acquired tracheobronchomalacia.
bronchi. The bronchi are involved to some de-
8. Koopot R, Nikaidoh H, Idriss FS: Surgical man-
gree in all severe cases of tracheomalacia, and
agement of anomalous left pulmonary artery
can be supported only partially by the stenting
causing tracheobronchial obstruction. J Thorac
In mild forms of tracheomalacia, symptoms
9. Vasko JS, Ahn C: Surgical management of sec-
ondary tracheomalacia. Ann Thorac Surg 6:269,
disappear in most patients by the age of 18 to 24
months [1, 3]. Duration of symptoms in the se-
10 Benjamin B, Cohen D, Glasson M: Tracheo-
vere variants has not been reported. Resolution
malacia in association with congenital tracheo-
occurred in 2 of our patients between 2 and 3
esophageal fistula. Surgery 79:504, 1976
years of age, after which time the tracheostomy
11 Cox WL, Shaw RR: Congenital chondromalacia of
tube was successfully removed. Another pa-
the trachea. J Thorac Cardiovasc Surg 49:1033, 1965
tient, although improved, still demonstrates 12. Levin SJ, Adler P, Scherer RA: Collapsible
bronchoscopic and clinical findings of tra-
trachea (tracheomalacia). Ann Allergv 22:20,
Study eyes epileptics' use of generic drugs January 3, 2010 By RIDGELY OCHS [email protected] Photo credit: Bloomberg News File | Topamax migraine medicine A blow to her head 20 years ago during a mugging left Thia Moore of Huntington with epilepsy. Until the state began picking up her drug costs, she had been paying $1,200 a month out of pocket for brand-name drugs that kept her
Julebrev 2004 En dag i det 21. århundrede. Eller tog jeg fejl, er det måske i middelalderen? Jeg kan ikke se forskel! I den vestlige verden frygter vi terrorister i en sådan grad at vi opfører os som de værste af alle. Vi har dræbt flere uskyldige mennesker i Afghanistan og Irak end nogen fundamentalistisk terrorist nogensinde er lykkedes med i den vestlige verden. Engang håbe
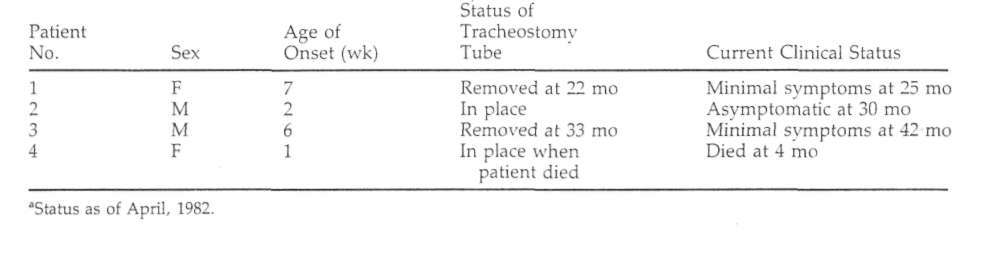 Clinical Data on 4 Patients with Severe Primary Tracheomalacia3
months later and died at home of respiratory
there is a definite worsening of symptoms with
crying and agitation, an observation that has
The courses of all 4 patients are summarized
not been reported previously. Each of our pa-
tients required sedation; in fact, Patient 1 re-quired temporary paralysis to control agitation
As noted earlier, tracheomalacia is characterized
Symptomatology is also markedly aggravated
by abnormal tracheal collapse secondary to in-
by respiratory tract infection. Three of our pa-
adequate supporting cartilaginous and myo-
tients had serious clinical deterioration during
elastic elements [1]. The condition has been di-
otherwise mild flu-like illnesses, and 1 died con-
vided into primary (congenital) and secondary
sequently. Presumably, the tracheobronchial lu-
(acquired) subgroups. Primary tracheomalacia men, already narrowed by tracheomalacia, be-is probably due to immaturity of the tracheo-
comes further compromised by inflammation.
bronchial cartilage [1]. Secondary tracheomala-
In addition, tracheobronchial secretions under
cia is due to degeneration of previously normal
these circumstances may be cleared less effec-
tracheal cartilages resulting from inflammatory
processes [4-7], extrinsic vascular compression
Baxter and Dunbar [1] employed fluoroscopy
[8, 9], bronchial neoplasms [5, 9], and tracheo-
and lateral inspiratory and expiratory chest
roentgenograms to establish the diagnosis of
There appear to be two distinct types of pri-
tracheomalacia. In our patients static inspiratory
mary tracheomalacia: the common or mild vari-
and expiratory chest roentgenograms were nor-
ant and an unusual, severe form. In 1963 Baxter
mal, and the critical clinical status of these in-
and Dunbar [1] reported 21 patients with pri-
fants precluded the use of fluoroscopy. We be-
mary tracheomalacia who displayed both types
lieve that bronchoscopy is absolutely necessary
of clinical symptomatology. The mortality de-
for definitive diagnosis. Also, because of the
pended upon the severity of the disease; there
safety of present-day equipment, this technique
were no deaths in patients with the mild form.
should be utilized early in the diagnostic pro-
Mortality in severe tracheomalacia has been re-
There is little information about the treatment
Severe primary tracheomalacia has an insidi-
of severe forms of tracheomalacia. Most of the
ous onset in an otherwise healthy infant, with patients reported by Cox and Shaw [11], Levin the appearance of progressively noisy respira-
and colleagues [12], and Baxter and Dunbar [1]
tions, episodic cyanosis, increased respiratory required no formal therapy, since they had the rate, intercostal retractions, and, finally, obvi-
mild form of the disease. In treatment of severe
ous stridor. The stridor is most noticeable dur-
forms, Picot and associates [3] recommended
ing expiration when maximal tracheobronchial hospitalization, oxygen, and, occasionally, tra-collapse normally occurs. In our experience cheostomy. Treatment with oxygen, postural
541 Cogbill et al: Primary Tracheomalacia
drainage, percussion, and frequent endotra-
cheal suctioning was unsuccessful in our pa-
1. Baxter JD, Dunbar JS: Tracheomalacia. Ann Otol
tients, and tracheostomy was ultimately neces-
2. Agosti E, DeFilippi G, Fior R, et al: Generalized
familial bronchomalacia. Acta Paediatr Scand
The efficacy of tracheostomy appears to be a
consequence of the tube's stenting effect on the
3. Picot C, Monnet P, Bethenod M, et al: La
semiflaccid trachea. More effective tracheo-
tracheomalacie du nourrisson. Arch Fr Ped
bronchial aspiration is also provided, but this is
probably less important. That tracheostomy is
4. Feist JH, Johnson TH, Wilson RJ: Acquired
not curative, or may not even prevent subse-
tracheomalacia: etiology and differential diag-
quent respiratory embarrassment in the face of
5. Johnson TH, Mikita JJ, Wilson RJ, et al: Acquired
intercurrent respiratory illness, was well illus-
trated in our small series. The probable mechan-
6. Jokinen K, Palva T, Sutinen S, et al: Acquired
ism for exacerbation of symptoms in this situa-
tracheobronchomalacia. Ann Clin Res 9:52, 1977
tion is inflammatory narrowing of the mainstem
7. Nuutinen J: Acquired tracheobronchomalacia.
bronchi. The bronchi are involved to some de-
8. Koopot R, Nikaidoh H, Idriss FS: Surgical man-
gree in all severe cases of tracheomalacia, and
agement of anomalous left pulmonary artery
can be supported only partially by the stenting
causing tracheobronchial obstruction. J Thorac
In mild forms of tracheomalacia, symptoms
9. Vasko JS, Ahn C: Surgical management of sec-
ondary tracheomalacia. Ann Thorac Surg 6:269,
disappear in most patients by the age of 18 to 24
months [1, 3]. Duration of symptoms in the se-
10 Benjamin B, Cohen D, Glasson M: Tracheo-
vere variants has not been reported. Resolution
malacia in association with congenital tracheo-
occurred in 2 of our patients between 2 and 3
esophageal fistula. Surgery 79:504, 1976
years of age, after which time the tracheostomy
11 Cox WL, Shaw RR: Congenital chondromalacia of
tube was successfully removed. Another pa-
the trachea. J Thorac Cardiovasc Surg 49:1033, 1965
tient, although improved, still demonstrates 12. Levin SJ, Adler P, Scherer RA: Collapsible
bronchoscopic and clinical findings of tra-
trachea (tracheomalacia). Ann Allergv 22:20,
Clinical Data on 4 Patients with Severe Primary Tracheomalacia3
months later and died at home of respiratory
there is a definite worsening of symptoms with
crying and agitation, an observation that has
The courses of all 4 patients are summarized
not been reported previously. Each of our pa-
tients required sedation; in fact, Patient 1 re-quired temporary paralysis to control agitation
As noted earlier, tracheomalacia is characterized
Symptomatology is also markedly aggravated
by abnormal tracheal collapse secondary to in-
by respiratory tract infection. Three of our pa-
adequate supporting cartilaginous and myo-
tients had serious clinical deterioration during
elastic elements [1]. The condition has been di-
otherwise mild flu-like illnesses, and 1 died con-
vided into primary (congenital) and secondary
sequently. Presumably, the tracheobronchial lu-
(acquired) subgroups. Primary tracheomalacia men, already narrowed by tracheomalacia, be-is probably due to immaturity of the tracheo-
comes further compromised by inflammation.
bronchial cartilage [1]. Secondary tracheomala-
In addition, tracheobronchial secretions under
cia is due to degeneration of previously normal
these circumstances may be cleared less effec-
tracheal cartilages resulting from inflammatory
processes [4-7], extrinsic vascular compression
Baxter and Dunbar [1] employed fluoroscopy
[8, 9], bronchial neoplasms [5, 9], and tracheo-
and lateral inspiratory and expiratory chest
roentgenograms to establish the diagnosis of
There appear to be two distinct types of pri-
tracheomalacia. In our patients static inspiratory
mary tracheomalacia: the common or mild vari-
and expiratory chest roentgenograms were nor-
ant and an unusual, severe form. In 1963 Baxter
mal, and the critical clinical status of these in-
and Dunbar [1] reported 21 patients with pri-
fants precluded the use of fluoroscopy. We be-
mary tracheomalacia who displayed both types
lieve that bronchoscopy is absolutely necessary
of clinical symptomatology. The mortality de-
for definitive diagnosis. Also, because of the
pended upon the severity of the disease; there
safety of present-day equipment, this technique
were no deaths in patients with the mild form.
should be utilized early in the diagnostic pro-
Mortality in severe tracheomalacia has been re-
There is little information about the treatment
Severe primary tracheomalacia has an insidi-
of severe forms of tracheomalacia. Most of the
ous onset in an otherwise healthy infant, with patients reported by Cox and Shaw [11], Levin the appearance of progressively noisy respira-
and colleagues [12], and Baxter and Dunbar [1]
tions, episodic cyanosis, increased respiratory required no formal therapy, since they had the rate, intercostal retractions, and, finally, obvi-
mild form of the disease. In treatment of severe
ous stridor. The stridor is most noticeable dur-
forms, Picot and associates [3] recommended
ing expiration when maximal tracheobronchial hospitalization, oxygen, and, occasionally, tra-collapse normally occurs. In our experience cheostomy. Treatment with oxygen, postural
541 Cogbill et al: Primary Tracheomalacia
drainage, percussion, and frequent endotra-
cheal suctioning was unsuccessful in our pa-
1. Baxter JD, Dunbar JS: Tracheomalacia. Ann Otol
tients, and tracheostomy was ultimately neces-
2. Agosti E, DeFilippi G, Fior R, et al: Generalized
familial bronchomalacia. Acta Paediatr Scand
The efficacy of tracheostomy appears to be a
consequence of the tube's stenting effect on the
3. Picot C, Monnet P, Bethenod M, et al: La
semiflaccid trachea. More effective tracheo-
tracheomalacie du nourrisson. Arch Fr Ped
bronchial aspiration is also provided, but this is
probably less important. That tracheostomy is
4. Feist JH, Johnson TH, Wilson RJ: Acquired
not curative, or may not even prevent subse-
tracheomalacia: etiology and differential diag-
quent respiratory embarrassment in the face of
5. Johnson TH, Mikita JJ, Wilson RJ, et al: Acquired
intercurrent respiratory illness, was well illus-
trated in our small series. The probable mechan-
6. Jokinen K, Palva T, Sutinen S, et al: Acquired
ism for exacerbation of symptoms in this situa-
tracheobronchomalacia. Ann Clin Res 9:52, 1977
tion is inflammatory narrowing of the mainstem
7. Nuutinen J: Acquired tracheobronchomalacia.
bronchi. The bronchi are involved to some de-
8. Koopot R, Nikaidoh H, Idriss FS: Surgical man-
gree in all severe cases of tracheomalacia, and
agement of anomalous left pulmonary artery
can be supported only partially by the stenting
causing tracheobronchial obstruction. J Thorac
In mild forms of tracheomalacia, symptoms
9. Vasko JS, Ahn C: Surgical management of sec-
ondary tracheomalacia. Ann Thorac Surg 6:269,
disappear in most patients by the age of 18 to 24
months [1, 3]. Duration of symptoms in the se-
10 Benjamin B, Cohen D, Glasson M: Tracheo-
vere variants has not been reported. Resolution
malacia in association with congenital tracheo-
occurred in 2 of our patients between 2 and 3
esophageal fistula. Surgery 79:504, 1976
years of age, after which time the tracheostomy
11 Cox WL, Shaw RR: Congenital chondromalacia of
tube was successfully removed. Another pa-
the trachea. J Thorac Cardiovasc Surg 49:1033, 1965
tient, although improved, still demonstrates 12. Levin SJ, Adler P, Scherer RA: Collapsible
bronchoscopic and clinical findings of tra-
trachea (tracheomalacia). Ann Allergv 22:20,