Hepatite aguda por Dengue CASE REPORT ACUTE HEPATITIS DUE TO DENGUE VIRUS IN A CHRONIC HEPATITIS PATIENT
Souza L.J1, Coelho J.M.C.O.4, Silva E.J. 2, 5, Abukater M.1, 2, Almeida F.C.R.1, 2, Fonte A. S.1, 2, Souza L.A. 1,3
1Centro de Referência da Dengue/Hospital Plantadores de Cana – Campos dos Goytacazes – RJ;
2Faculdade de Medicina de Campos; 3Universidade Estácio de Sá; 4 Laboratório de Referência Nacional
para Diagnóstico Histopatológico de Doenças Infecciosas/IPEC/FIOCRUZ – RJ; 5 Faculdade de Ciências
Médicas da Universidade Estadual do Rio de Janeiro/UERJ.
ABSTRACT
We present a case of acute hepatitis caused by Dengue virus, with significant increase in aspartate
transferase and alanine transferase levels in a chronic hepatitis patient in the Cane Sugar Planters Hospital
Key words: dengue, liver failure, chronic hepatitis.
INTRODUCTION
Dengue is an arbovirus disease caused by a flavivirus with four known serotypes; it is typical of
tropical and subtropical regions, where socio-economic conditions favor the development of its vector, Aedes aegypti 1. Infection by one serotype confers permanent or long-term immunity only against that particular
serotype 1,2. It is believed that more than 100 million inhabitants of tropical countries become infected every
This disease can present with a wide spectrum of clinical manifestations, including asymptomatic,
classical dengue symptoms, dengue hemorrhagic fever, and atypical forms. The uncommon clinical
manifestations of this disease are generally due to a multifactor condition, associated with direct aggression
by dengue virus. Dengue can provoke alterations in hepatic functions and typical symptoms of acute
hepatitis, such as pain in the right hypochondrium, hepatomegaly, jaundice and elevated transaminase
levels. When hepatitis occurs, the transaminase levels reach their maximum on the ninth day after symptoms
appear and return to normal within three weeks 4,5.
Laboratory investigation of this arbovirus includes various types of exams, from non-specific
analyses to confirmatory serology. Hemograms of patients infected with this virus show leucopenia with
Hepatite aguda por Dengue
atypical lymphocytes, thrombocytopenia (<100,000/mm3) and in some cases, hemoconcentration 1,4. Low
degrees of inflammation and elevated hepatic enzymes are also indicative of infection by dengue.
CLINICAL CASE
The patient was 77 years old, male, white, married, retired, born in Campos dos Goytacazes, RJ.
Three days previously, the patient began to have fever, anorexia, arthralgia, myalgy, headaches, nausea,
vomiting, prostration, a bitter taste in the mouth and a dry cough; he was taking paracetanol. During this
period, he also complained of dark “coca cola” urine and light-colored stool. The patient evolved to
abdominal extension, associated with pain and feeling full. HPP: Negative for Diabetes Mellitus, high blood
pressure, which was being treated with captopril, and a history of dengue fever in 2003. Social status: ex
Physical exam: Awake, in good general condition, normal respiration, not cyanotic, jaundice (+/4),
dehydrated (+/4), no fever, normal color. ACV: normal cardiac rhythm in two phases, no audible. heart
wheezing Blood pressure: 170 x 100mm Hg. AR: no alterations. Abdomen: flaccid, depressible, diffusely
painful to deep palpation. Hepatomegaly three cm from the right costal margin. Spleen not palpable. MMII:
After seven days, the patient returned to the clinic, presenting strong deterioration of his general
condition, with worsening symptoms, and was consequently hospitalized. Physical exam showed prostration,
jaundice (4+/4), dehydrated (2+/4), no fever, and normal color. BP: 150 x 110mm Hg. Abdomen: Flaccid,
depressible, painful to deep palpation of the hypochondrium hipocôndrio and right side. Hepatomegaly 5 cm
from the right costal border. Spleen not palpable.
Complementary exams: X-ray of the thorax: Normal. Leucocytes 3,400/uL; Hematocrit: 42%;
hemoglobin 13.9g/dL; hemocytes 5,130 M/uL; platelets: 95,000/uL; VHS 23mm; AST 8,813 U/L, ALT 3,213 U/L, Alkaline phosphatase: 317U/L. Based on these symptoms, the patient was hospitalized.
In the hospital, the patient improved clinically, with increased jaundice. New exams were
requested: Leucocytes 7,600/uL, hematocrit 39.4%, hemoglobin 13.4g/dl, red blood cells 4,860M/uL,
platelets 216,000/uL, AST 1.081U/L, ALT 1.625U/L, TAP 18seg./18/%, Total proteins 6.9 (Alb. 2.2/Glob.
4.7), creatinine 0.92, urea 23.5, total bilirubin 20.12mg/dL (BD18.23/BI 1.89), amylase 82U/L, lipase 50U/L,
alkaline phosphatase 290U/L, gamaGT 82U/L. IgM Serology for Dengue: reactive, Anti-HAV(IgG): Hepatite aguda por Dengue
reactive, Anti-HAV(IgM), HbsAg, HbeAg, Anti-Hbs, Anti-Hbc(IgM), Anti-HCV, Seroagglutination for
Leptospirosis and serology for yellow fever: Not reactive.
USG of the abdomen: Echogenic liver, with normal dimensions, suggesting light to moderate
Observation: A small accumulation of free liquid was observed in the abdomen (ascites), with no
Figure 1.
On the seventh day of hospitalization, new exams were made: Leucocytes 8,000/uL, Hematocrit
43.4%, red blood cells 5,380M/uL, platelets 302.000, TAP 18s/47%, Total bilirubin 25.68mg/dL (BD 23.25/BI
2.43), AST 341U/L, ALT 576U/L, alkaline phosphatase 211U/L, total protein 7.9 (Alb. 2.7/ Glob. 5.2), direct
Coombs: negative, anti-smooth muscle: 1:80, anti KLM: negative.
Tomography of the abdomen: Free liquid in the cavity, but without other alterations.
Endoscopy of the upper digestive tract: normal.
During hospitalization, the patient was maintained on symptomatic medication, intravenous
hydration, furosemid and spironolactone. On the 15th day of hospitalization, after other diagnoses had been
discarded, the patient maintained symptoms of jaundice (4+/4) and a hepatic biopsy was solicited.
Anatomical-Pathological signs Microscopy:
Hepatic biopsy revealed an approximately 18 portal space ratio. Hepatocytes mainly
swollen, presenting reactional alterations and isolated necrosis foci. Portal space widened by fibrosis, with
porto-portal bridges, next to others portal-center. Ductal alterations, cholestasis and moderate lymphocytic
and neutrophilic infiltration. The color of the PAS did not reveal anomalous deposits. Masson staining
Conclusion: Acute and chronic hepatopathy associated with hepatic cirrhosis.
Hepatite aguda por Dengue
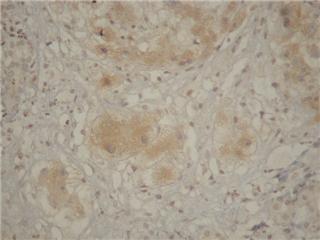
Observation: Imuno-histochemistry for Dengue revealed an immune reaction evident in the
The patient was released from the hospital and continued to be treated through ambulatory visits,
with remission of symptoms and normalization of hepatic enzymes.
Figure 2. Figure 3. DISCUSSION
Dengue is considered the most important arthropod-transmitted virosis that affects man in terms of
morbidity and mortality3. The world health organization (WHO) estimates that from 50-100 million people are
infected annually, in more than 100 countries, on all continents, except Europe6. In Brazil, Dengue occurs
primarily from January to May, because of favorable conditions for the mosquito vector, Aedes aegypti, that
time of year. During the 1990s, even during non-epidemic years, the disease affected tens of thousands of
people per year. The last epidemic in Brazil occurred in 2002, due to the introduction of DEN-3; 794,219
cases were reported, most of them in Rio de Janeiro. In the following years, the dispersion of DEN-3 to other
states in Brazil resulted in outbreaks and epidemics, but without reaching the levels of 2002. The secretary
for health vigilance of the health ministry (SVS/MS) registered 438,949 cases of classic Dengue, 926 cases
of Hemorrhagic Dengue and 98 deaths from January to July 20076. Consequently, Dengue has become one
of the principal problems for public health programs.
The clinical picture of classic dengue begins with high fever, head aches, intense myalgy,
prostration, nausea, vomiting and arthralgia. The first clinical manifestations of Dengue hemorrhagic fever
are indistinguishable from those of classic dengue4. In some individuals, the clinical presentation can
assume atypical forms, such as encephalitis, aseptic meningitis, poly neuropathies, cholecystitis acalculous,
polyserositis and acute viral hepatitis4,7. In most cases of acute hepatitis, caused by dengue virus, the
differential diagnosis should include leptospirosis, yellow fever, malaria and hepatitis A, B, and C4.
The liver is one of the target organs for dengue, and clinical manifestations of hepatic disfunction can
occur during the course of this disease4. Hepatic involvement is characterized by acute hepatitis, with pain in
the right hypochondrium, hepatomegaly, fever, coagulopathy, increased levels of aminotransferases, and
increased bilirubin, leading to jaundice. This can be explained by the host response to the agent, leading to
alterations in perfusion in various tissues, in an attempt to preserve vital organs. The liver is deprived of
oxygen, leading to lesion of the parenchyma, in which the lesioned hepatocytes liberate transanimases that
Hepatite aguda por Dengue
are detectable in the peripheral blood1. In most cases, the high levels of transaminases show the degree of
hepatocellular injury, prolonging the clinical course of this disease; however, there is no correlation with
prognosis. Another means to evaluate hepatic function is to measure protein synthesis, based on albumin
concentration and prothrombin time, which can be measured.
Hepatic cirrhosis, characterized by diffuse substitution of the normal hepatic structure by abnormally
structured nodules, surrounded by fibrosis, is the common final stage of a series of hepatic pathologies with
various causes, such as alchoholism, viral and auto-immune chronic hepatitis, as well as metabolic, vascular
In our patient, the intensity of the alterations observed in the hepatic exams, with initial values of AST
8.813U/L and ALT 3.213U/L, coagulopathy, ascitis and some degree of disorientation, suggested an
investigation of contributing pathologies, which lead to a diagnosis of hepatic insufficiency.
Initially, drug-induced hepatitis was suggested, because the patient had used paracetanol for several
days. Paracetanol can cause liver damage and can lead to or aggravate primary lesions caused by dengue
virus. This diagnosis was discarded after hepatic biopsy.
Laboratory and imaging exams excluded a diagnosis of viral hepatitis (A, B and C), auto-immune
hepatitis, leptospirosis, biliary tract diseases and obstructive neoplasias. As serology was positive for dengue
virus, a hepatic biopsy was made to confirm the diagnosis.
Analysis of the liver tissue was made using Hematoxilin-Eosin, Masson trichrome, PAS, PEARL’S
and silver Reticulin staining. Observed morphology was that of acute and chronic hepatopathy, associated
with liver fibrosis and regeneration nodules, consistent with liver cirrhosis. Immuno-histochemical studies
were made, using the streptavidin-Biotin-Peroxidase technique, and a polyclonal anti-Dengue antibody,
which revealed a granular positive immune reaction in the hepatocytes. Consequently, the diagnosis of acute
hepatitis due to dengue virus was confirmed in this cirrhotic patient.
BIBLIOGRAPHY
1- Souza L.J., Dengue – Diagnóstico Tratamento e Prevenção, Rio de Janeiro: Ed Rúbio, 2007.
2- Wilder-Smith A, Schwartz E.Dengue in Travelers, NEJM 353:924, September 1, 2005 Review
3- Focaccia, R(Ed.).Veronesi tratado de infectologia. 3. ed, rev. e atual. São Paulo: Atheneu, 2006. 1 v.
4- Souza, LJ de et al. Hepatitis in Dengue Shock Syndrome. Braz J Infect Dis, Dec 2002, vol.6, nº6,
Hepatite aguda por Dengue
5- Souza, LJ de et al. Aminotransferase changes and acute hepatitis in patients with dengue fever:
analysis of 1,585 cases. Braz J Infect Dis, Apr 2004, vol.8, nº2, p.156-163. ISSN 1413-8670
saúde. Secretaria de Vigilância em Saúde.
7- Nogueira S.A. Dengue: artigo de revisão. Revista de Pediatria Soperj 2001;2(1):22-8.
8- Venancio AFA et al. Cirrose hepática: aspectos morfológicos relacionados às suas possíveis
complicações. Um estudo centrado em necropsias. J. Bras. Patol. Med. Lab. vol.41 no.1 Rio de
9- Navarro VJ, Senior JR. Drug-Related Hepatotoxicity, NEJM 354:731, February 16, 2006 Review
10- KASPER, Dennis L. (Ed. et al.). Harrison Medicina Interna. 16ªed. Rio de Janeiro: McGraw Hill,
Hepatite aguda por Dengue Figure 1. Abdominal Ultrasound showing ascites Hepatite aguda por Dengue Figure 2. Hepatic Biopsy - T. Masson – Hepatic Cirrhosis Figure 3. Positive immune reaction for Dengue in the cytoplasm of hepatocytes.
ORDINANCE NO. 2013-05 An Ordinance Pertaining to the Regulation of Firearms, Weapons, and Explosives, Throwing or Shooting of Arrows, Stones and other Missiles and Facsimile Firearms The Common Council of the City of Cedarburg, Wisconsin, hereby ordains as follows: SECTION 1. Section 11-2-1 of the Municipal Code of the City of Cedarburg is hereby SEC. 11-2-1 REGULATION OF FI
European Journal of Neurology 2004, 11: 483–488Pergolide mesylate can improve sexual dysfunction in patientswith Parkinson’s disease: the results of an open,prospective, 6-month follow-upM. Pohankaa, P. Kanˇovsky´b, M. Baresˇb, J. Pulkra´bekb and I. RektorbaDepartment of Sexology, Teaching Hospital, Brno Bohunice; and bFirst Department of Neurology, Masaryk University, St Anne Hospital,

 Hepatite aguda por Dengue
Hepatite aguda por Dengue 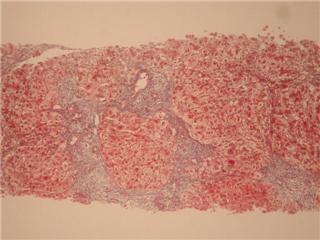
 Hepatite aguda por Dengue
Hepatite aguda por Dengue