Women’s Health Issues 13 (2003) 74 –78
MIND CONTROL OF MENOPAUSE
Jawaid Younus, MDa, Ian Simpson, MDb, Alison Collins, RNb, Xikui Wang, PhDc
aLondon Regional Cancer Centre, London, Ontario, Canada
bWestern Memorial Regional Hospital, Corner Brook, Canada
cDepartment of Statistics, University of Manitoba, Winnipeg, Canada
Received 29 July 2002; accepted 14 November 2002
The primary objective of this study was to observe the effect of hypnosis on hot flashes (HF) and overall quality of life in symptomatic patients. A secondary objective was to observe the effect of hypnosis on fatigue. Ten healthy volunteers and four breast cancer patients (total 14 patients) with symptoms of HF were treated with four, 1 h/wk sessions of hypnosis. The same physician, with the help of a nurse, conducted every session. All subjects recorded frequency, duration, and severity of HF in a HF diary. The QLQ-C30 and Brief Fatigue Inventory forms were used to assess the impact on quality of life and fatigue, respectively. The statistical evaluations were performed, including analysis of variance and nonparametric procedures. The frequency (p Ͻ 0.0001), duration (p Ͻ 0.0001), and severity (p Ͻ 0.0001) of HF were significantly reduced. The overall quality of life was also improved (p ϭ 0.05). The subjects enjoyed better sleep and had less insomnia (p ϭ 0.012). There was a significant improvement on current fatigue level (p ϭ 0.017), but we did not find a statistically significant reduction in the total fatigue level. We conclude that hypnosis appears to be a feasible and promising intervention for HF, with a potential to improve quality of life and insomnia. Although improvement in current level of fatigue was observed in this pilot study, total fatigue improvement did not reach statistical significance. Keywords: Menopause, Hormonal replacement therapy, Hypnosis, Hot flash Thehotflash(HF)isdescribedasaheatorwarmth to improve HF. This pilot study was performed to
sensation of the skin, often accompanied by other
evaluate the role of hypnosis to improve HF symp-
symptoms, such as sweating.1 The majority of both
toms and to observe its impact on quality of life and
postmenopausal and perimenopausal women report
HF symptoms. Hormonal replacement therapy andvarious other pharmacologic interventions have lim-ited success and are not without side effects. Such
treatments include clonidine, methyldopa, vitamin E,
The Institutional Review Board of Western Memorial
megesterol acetate, and antidepressants such as ven-
Regional Hospital approved this study. Ten healthy
lafaxine. Nonpharmacologic approaches, such as be-
volunteers and four breast cancer patients were re-
havioral therapy, are viewed as helpful and generally
cruited at the Corner Brook Cancer Center, from
without side effects and thus appear attractive to both
August 2000 to April 2001. The participants were
considered eligible if they had history of HF for at
Hypnosis has been used successfully to improve
least 1 month with a frequency of 5 or more episodes/
symptoms in a variety of clinical disorders. To date,
week. Patients with breast cancer were eligible, pro-
there is no report in the literature of using hypnosis
vided they had completed their cancer therapy 3months before their enrollment for this trial. Patientswith metastatic breast cancer were not considered
* Correspondence to: Dr. Jawaid Younus, London Regional Can-
eligible. Patients were excluded upon their refusal or if
cer Centre, 790 Commissioners Road East, London, Ontario N6A4L6, Canada.
any physical condition or cognitive impairment pre-
vented them from completing the questionnaire and
Copyright 2003 by the Jacobs Institute of Women’s Health. J. Younus et al. / Women’s Health Issues 13 (2003) 74 –78Figure 1. One-way ANOVA for frequency. The upper and lower tips for each diamond indicate the 95% confidence interval for the mean on each day. The upper and lower horizontal segments within each diamond are the 95% overlap marks. When the sample sizs are equal (which is the case on most days), two means are significantly different if their overlap marks do not overlap. The horizontal line inside the rectangle is the overall sample mean.
HF diary. An informed consent was obtained before
all quality of life. The secondary end point was the
the registration for each participant. To maintain con-
fatigue level. Analysis of variance (ANOVA) and two
fidentiality, their provincial medical numbers identi-
nonparametric procedures—the Kruskal-Wallis test
fied participants. All data were pooled for analysis.
(KW) and the median test (MT)—were performed on
No concurrent therapy with chemotherapy, radiation
SAS and JMP IN (a product from SAS). Regression
therapy, or any known therapies for HF was allowed.
analysis was used to quantify the improvement in
Patients on tamoxifen were allowed to continue using
frequency of HF and in other variables.
All participants completed four weekly group hyp-
nosis sessions. Each group had 4 –5 participants. After
an introduction to hypnosis and an explanation ofmind/body interaction, participants underwent a gen-
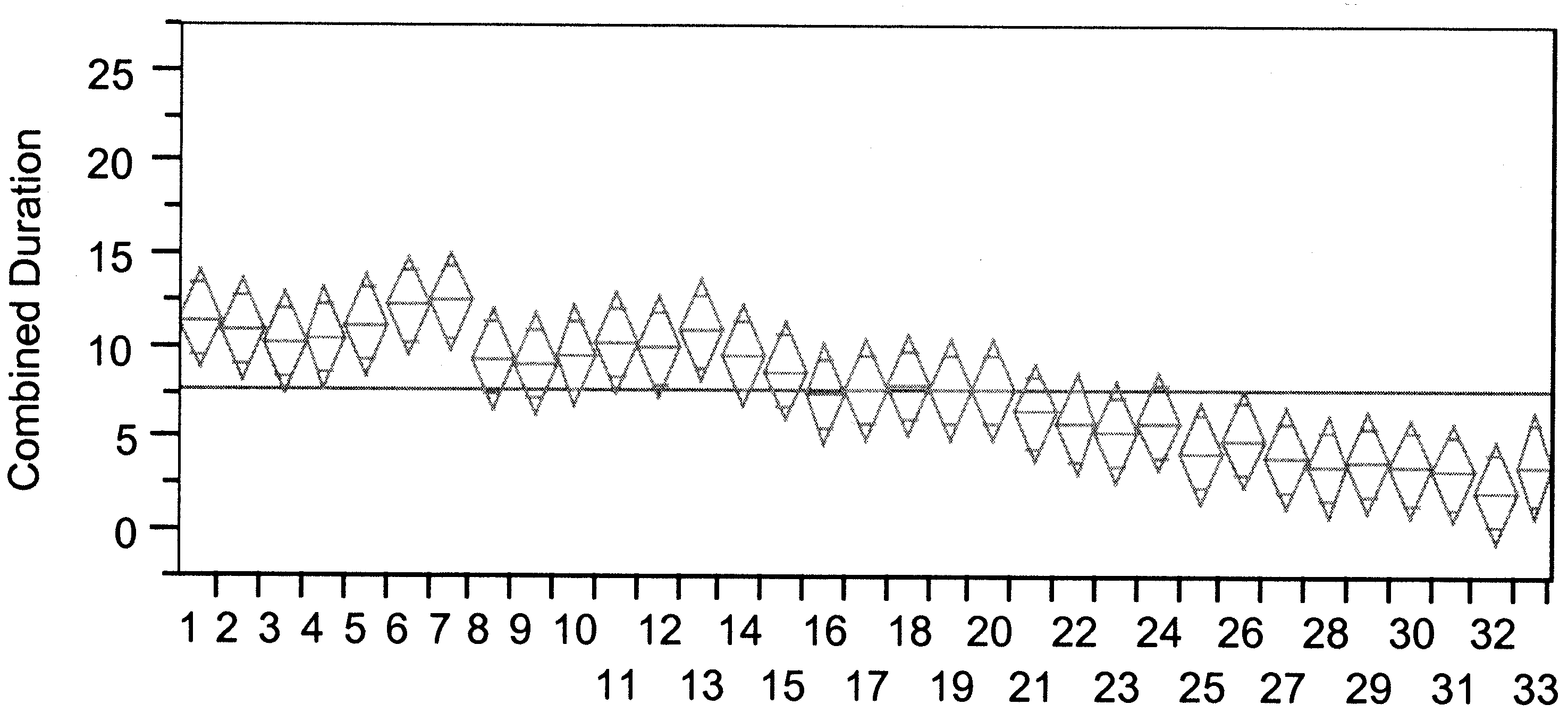
The frequency (p Ͻ 0.0001 for all tests), duration (p Ͻ
tle relaxation phase that led to light-trance hypnosis.
0.0001 for all tests), and severity (p Ͻ 0.0001 for all
Additionally, in the last two sessions, specific sugges-
tests) of HF were significantly reduced with hypnosis.
tions were given to reduce and block HF symptoms.
Figure 1 shows one-way ANOVA results for reduction
The same physician with the help of a registered nurse
in HF frequency during the treatment period. Because
conducted all the sessions. The quality of life, insom-
both duration and severity are ordinal with categorical
nia, and overall health evaluations were based on the
values, we introduced combined duration and com-
QLQ-C30 questionnaire,2 which is well described and
bined severity as the weighted average of various
widely used. We used the Brief Fatigue Inventory
levels. Figures 2 and 3 illustrate the improvement in
(BFI) form to calculate present and total level of
the combined severity and combined duration of HF
fatigue.3 The total fatigue level was derived as a
over the treatment period, respectively. Interestingly,
composite score from six different questions, which
all three figures show the beginning of improvement
asked the participants about their activity, mood,
around Day 14. Sensitivity analysis was performed to
walking ability, work, relationship with people, and
examine the effect of the weights on the results, and it
enjoyment of life. The trial participants filled out the
was found that statistical results were robust as long
QLQ-C30 and BFI form before the commencement of
as the weights were monotonic (with higher values for
hypnosis sessions, after the second and fourth ses-
higher levels of duration or severity). Regression anal-
sions, and finally at the 1-month follow-up visit. All
ysis showed that on average, there was a 0.2 reduction
participants kept a record of frequency, duration, and
per day seen in frequency (p Ͻ 0.0001), a 0.38 reduc-
severity of their HF in a daily diary, starting 1 week
tion per day in the combined duration (p Ͻ 0.0001),
before first session and continued throughout the
and 0.47 reduction per day observed in the combined
The primary end points for this study were the
There was a significant improvement on overall
frequency, duration, and severity of HF and the over-
quality of life for the first 3 weeks (p ϭ 0.0143 for
J. Younus et al. / Women’s Health Issues 13 (2003) 74 –78Figure 2. One-way ANOVA for combined Severity. The combined severity is calculated by the formula “Mild” ϩ 2 * “Moderate” ϩ 3 * “Severe” ϩ4 * “Extreme”.
ANOVA, 0.0203 for KW, and 0.0784 for MT) and for all
hormonal treatment for breast cancer can induce HF in
4 weeks (p ϭ 0.0509 for ANOVA, 0.0633 for KW, and
50% of such patients.5,6 Several reports have described
sleep disturbances and feeling a low status of well-
There is some evidence for a trend toward im-
being, with an overall reduced quality of life in
proved overall health for the first 3 weeks (p ϭ 0.0882
for ANOVA, 0.1058 for KW) but not for all 4 weeks (p
Although widely used, the routine use of hormonal
ϭ 0.12 for ANOVA, 0.1985 for KW). There was a
replacement therapy9 for the HF symptom is now
significant improvement on current fatigue level (p ϭ
under question after a recent report.10 Other pharma-
0.0184 for ANOVA, 0.0169 for KW, and 0.0304 for
cologic therapies like clonidine, methyldopa, and vi-
MT). The improvement observed on total fatigue
tamin E, provide modest relief at best.11–13 Megestrol
reduction was not statistically significant (p Ͼ 0.1 for
acetate and venlafaxine produce reasonable improve-
all questions and a composite value). There was a
ment in HF.14,15 However, the routine use of megestrol
significant reduction found for insomnia (p ϭ 0.0125
acetate in breast cancer patient is not recommended.15
for ANOVA, 0.067 for KW, and 0.0042 for MT) in the
Behavioral therapies have been used successfully for
HF. One study16 recruited four postmenopausalwomen and demonstrated significant reduction in HFafter using a combination of four behavioral therapies. DISCUSSION
The treatment benefits were felt to last up to 6 months
HF is a common symptom, experienced by 60 – 85% of
of follow-up. Another study compared muscle relax-
women around the menopause.4 Adjuvant chemo-
ation, paced respiration, and placebo in 33 postmeno-
Figure 3. One-way ANOVA for combined duration. The combined duration is calculated by the formula “Duration Ͻ” ϩ 2 * “Duration Ͼ 1”. J. Younus et al. / Women’s Health Issues 13 (2003) 74 –78
pausal women and found paced respiration to be
factors may still be largely considered as compo-
effective in reducing the HF significantly.17 More
recently, cognitive behavioral therapy, which con-
In summary, our study provides preliminary but
sisted of 1-h individual training for 6 – 8 weeks,
encouraging results for hypnosis to be explored as an
produced improvement in HF, depressive mood,
intervention against HF. This study is limited by small
and anxiety.18 Wijma et al.19 used applied relaxation
number of subjects and recruitment of consecutive
in 6 women, 1 h/wk for 12 weeks. They were able to
participants without premeasuring their individual
show a reduction in HF and improvement in quality
susceptibility to hypnosis. However, considering that
there has been no previous study about the role of
A simple definition of hypnosis would be a state
hypnosis against HF, this study should serve as a pilot
of attentive, focused concentration with suspension
of some peripheral awareness.20 Hypnosis has beenused to alleviate pain,21 treat gastrointestinal disor-ders,22,23 and reduce anticipatory nausea and vom-
References
iting related to chemotherapy.24 Hypnosis remains
[1] Ginsburg SE. Hot flashes—physiology, hormonal therapy and
as only partially understood intervention. Accord-
alternative therapies. Obstet Gynecol Clin North Am 1994;21:
ing to a recently described conceptual model,25
[2] Dancey J, Zee B, Osoba D, et al. Quality of life scores: an
hypnosis may utilize belief, expectation, relaxation,
independent prognostic variable in a general population of
imagery, and dissociation, either individually or in
cancer patients receiving chemotherapy. Qual Life Res 1997;6:
combination to provide symptomatic benefit. To
date there is no published report in the literature
[3] Mendoza TR, Wang XS, Cleeland CS, et al. The rapid assess-
describing the role of hypnosis to alleviate HF
ment of fatigue severity in cancer patients: use of the BriefFatigue Inventory. Cancer 1999;85:1186 –1196.
[4] McKinlay SM, Brambilla DJ, Posne JG. The normal menopause
The schedule we used was relatively simple and
transition. Am J Human Biol 1992;4:37– 46.
short, allowing 4 –5 participants to be treated at the
[5] Fisher B, Constantino J, Redmond C. A randomized clinical
same time. It is interesting to note that the HF
trial evaluating tamoxiferin in the treatment of patients withnode negative breast cancer who have estrogen receptor posi-
symptoms started to improve in our study partici-
tive tumors. N Engl J Med 1989;320:479 – 484.
pants around the second week mark (Figures 1–3),
[6] Knobf M. Breast cancer. In Bairs S; McCorkle R; Grant M,
coinciding with the time when actual suggestions
editors. Cancer nursing: a comprehensive textbook. Philadel-
against HF were included in the hypnotherapy
sessions. This observation favors hypnosis rather
[7] Erlik Y, Tataryn IV, Meldrum DR. Association of waking
episodes with menopausal hot flashes. JAMA 1981;245:1741–
than simple relaxation being responsible for these
results. It is encouraging to note the improved
[8] Ferrell BR. The quality of lives: 1525 voices of cancer. Oncol
overall quality of life in our study participants along
with the improvement in their HF symptoms. The
[9] Mishell D. Noncontraceptive benefits of oral contraceptives. J
Repro Med 1993;38(Suppl. 12):1021–1029.
overall health level showed only a trend to improve-
[10] Rossouw JE, Anderson GL, Prentice RL, et al. Risks and
ment, which may be partially explained by the fact
benefits of estrogen plus progestin in healthy post-menopausal
that there were 10 healthy volunteers among 14
women: principal results from the women’s health initiative
study participants. It is certainly plausible that in
randomized controlled trial. JAMA 2002;288:321–333.
addition to hypnosis, relaxation and better sleep
[11] Loprinzi CL, Goldberg RM, O’Fallon Jr, et al. Transdermal
clonidine for ameliorating post-orchiectomy hot flashes. J Urol
may have contributed to improve the present fa-
tigue level. The total fatigue remained unaffected.
[12] Nesheim BI, Saetre T. Reduction of menopausal hot flashes by
Although no clear inference can be drawn, our
methyldopa: a double blind crossover trial. Eur J Clin Pharma-
results provide a hint that HF may not significantly
[13] Barton DL, Loprinzi CL, Quella SK. Prospective evaluation of
affect general activity and may not interfere with
vitamin E for hot flashes in breast cancer survivors. J Clin
work, relationship with people, and enjoyment of
life in women with HF. These factors may be too
[14] Loprinzi DL, Michalak JC, Quella SK, et al. Megestrol acetate
general and spread across a longer period of time
for the prevention of hot flashes. N Engl J Med 1994;331:347–
(weeks/months) to be affected by HF. The inciden-
[15] Loprinzi CL, Pisansky TM, Fonseca R. Pilot evaluation of
tal finding of improved insomnia, in addition to
venlafaxine hydrochloride for the therapy of hot flashes in
hypnosis, could have resulted from psychosocial
cancer survivors. J Clin Oncol 1998;16:2377–2381.
group support and relaxation during the hypnother-
[16] Stevenson DW, Delprato DJ. Multiple component self-control
apy sessions. Thus, present level fatigue, insomnia,
program for menopausal hot flashes. J Behav Ther Exp Psy-chiat 1983;14:137–140.
and quality of life may have been possibly impacted
[17] Freedman RR, Woodward S. Behavioral treatment of meno-
by factors other than hypnosis. However, consider-
pausal hot flashes: evaluation by ambulatory monitoring. Am J
ing the multifactorial model for hypnosis,25 these
J. Younus et al. / Women’s Health Issues 13 (2003) 74 –78
[18] Hunter MS. A treatment option for menopausal hot flushes:
hypnotherapy in relapse prevention of duodenal ulceration.
cognitive relaxation therapy. Eur Menopause J 1995;2:16 –17.
[19] Wijma K, Melin A, Nedstrand E, Hammar M. Treatment of
[23] Harvey RF, Hinton RA, Gunray RM, Barry RE. Individual and
menopausal symptoms with applied relaxation: a pilot study. J
group hypnotherapy in treatment of refractory irritable bowel
Behav Ther Exp Psychiat 1997;28:251–261.
[20] Spiegel H, Spiegel D. Trance and treatment: clinical uses of
[24] Redd WH, Andersen GV, Minagawa RY. Hypnotic control of
hypnosis. New York: Asic books; 1978.
anticipatory emesis in patients receiving cancer chemotherapy.
[21] Spiegel D, Blo JR. Group therapy and hypnosis reduce meta-
static breast carcinoma pain. Psychosom Med 1983;45:333.
[25] Evans JF. The domain of hypnosis: a multifactorial model. Am J
[22] Colgan SM, Faragher EB, Whorwell PJ. Controlled trial of
Don’t Let the Flu Get You Down It’s no secret that the 2009/2010 flu season will be challenging. Between the H1N1 Virus (“Swine Flu”) the seasonal flu, and a myriad of cold viruses, staying healthy certainly won’t be easy this winter. In fact, to help prepare for a potential outbreak of H1N1 Flu virus, the Massachusetts Department of Public Health is working to distribute a flu
For Surrey and Borders Partnership Foundation Trust Migraine Awareness Week: 6th -12th September Opening hours Crawley Library: The Migraine Action Association is a charity which aims to encourage, support and raise funds for research into migraine, produce and dissimilate information about treatments, and East Surrey Library: provide reassurance and understanding to Mon, Th
 Women’s Health Issues 13 (2003) 74 –78
MIND CONTROL OF MENOPAUSE
Women’s Health Issues 13 (2003) 74 –78
MIND CONTROL OF MENOPAUSE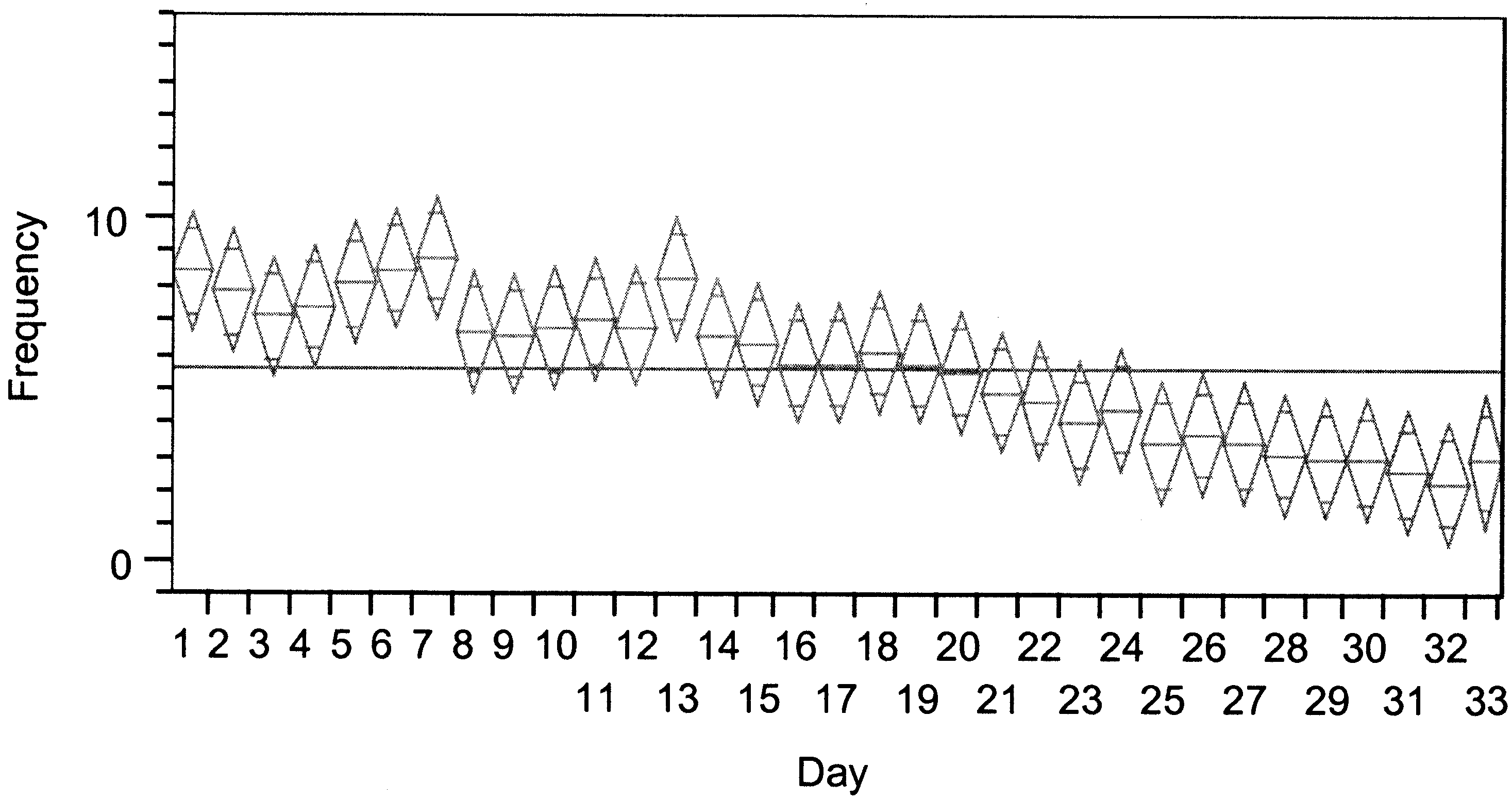 J. Younus et al. / Women’s Health Issues 13 (2003) 74 –78
Figure 1. One-way ANOVA for frequency. The upper and lower tips for each diamond indicate the 95% confidence interval for the mean on
J. Younus et al. / Women’s Health Issues 13 (2003) 74 –78
Figure 1. One-way ANOVA for frequency. The upper and lower tips for each diamond indicate the 95% confidence interval for the mean on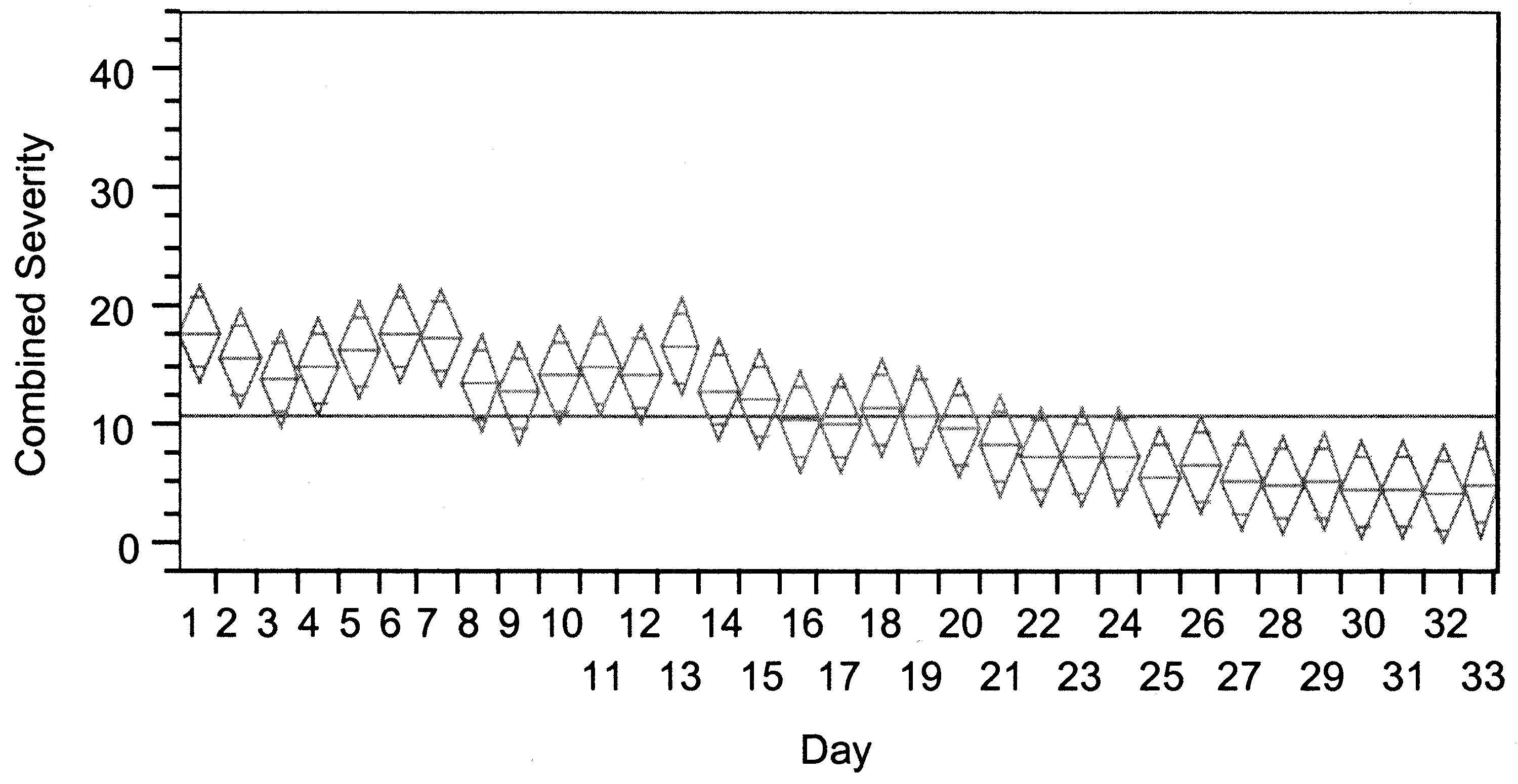
 J. Younus et al. / Women’s Health Issues 13 (2003) 74 –78
Figure 2. One-way ANOVA for combined Severity. The combined severity is calculated by the formula “Mild” ϩ 2 * “Moderate” ϩ 3 *
J. Younus et al. / Women’s Health Issues 13 (2003) 74 –78
Figure 2. One-way ANOVA for combined Severity. The combined severity is calculated by the formula “Mild” ϩ 2 * “Moderate” ϩ 3 *