Breast Cancer Research and Treatment 66: 225–237, 2001. 2001 Kluwer Academic Publishers. Printed in the Netherlands. Breast cancer survival and in vitro tumor response in the extreme drug resistance assay
Rita S. Mehta1,4, Richard Bornstein2, Ing-Ru Yu1, Ricardo J. Parker1, Christine E. McLaren3,4,Khanh P. Nguyen4, Kuo-Tung Li4, and John P. Fruehauf1,41Oncotech, Inc., CA; 2Center for Breast Health, OH; 3Epidemiology Division, Department of Medicine, Universityof California, Irvine; 4Chao Family Comprehensive Cancer Research Center, University of California, Irvine,Orange, CA, USAKey words: breast cancer, chemotherapy, drug resistance, in vitro assay, survival
Purpose. To determine whether in vitro extreme drug resistance (EDR) assay results for patients with breastcarcinoma were associated with clinical outcome after chemotherapy. Patients and methods. EDR assays were performed on tumor tissue obtained from 103 newly diagnosed breast
cancer cases. EDR scores of 2 for low, 1 for intermediate, or 0 for extreme drug resistance were determined foreach agent tested. In vitro EDR scores for 4-hydroxycyclophosphamide (4HC) and doxorubicin were summed forpatients treated with AC, or for 4HC and 5-FU for patients treated with CMF. Treatment selection was blinded toassay results. Results. Median time to progression was significantly shorter for patients with extreme or intermediate in vitro
resistance (n = 55, 48 months), compared to patients with low in vitro resistance, (n = 41, 100 months, p = 0.022). Patients demonstrating extreme to intermediate drug resistance also showed poorer survival than the low resistancegroup (49.5 months vs. not reached, median follow-up 48 months, p = 0.011). Summed EDR scores, stage,and number of lymph nodes were significantly associated with survival in univariate and multivariate analysis. Compared to EDR scores of 4, summed EDR scores of 0–1 and summed EDR scores of 2–3 were associated witha relative risk of death of 3.09 (95%, CI 1.05–9.06, Cox proportional hazards model, p = 0.040) and 2.35 (95%,CI 1.07–5.15, Cox proportional hazards model, p = 0.033), respectively. Conclusion. Extreme drug resistance testing identified patients with individual patterns of drug resistance
prior to therapy. In this cohort of breast cancer patients treated with chemotherapy, summed EDR scores weresignificantly associated with time to tumor progression and overall survival. EDR results may offer a method foroptimizing treatment selection. Abbreviations: EDR: extreme drug resistance; IDR: intermediate drug resistance; LDR: low drug resistance; CTX:cyclophosphamide; 4HC: 4-hydroxycyclophosphamide; 5-FU: 5-fluorouracil; MTX: methotrexate; AC: doxorubi-cin and cyclophosphamide; CMF: cyclophosphamide, methotrexate and fluorouracil; CI: confidence interval; ER:estrogen receptor
Introduction
Coldman hypothesis by targeting the heterogeneousmalignant clones within each patient [1, 2]. This
Multiagent chemotherapy is an important compon-
strategy led to the development and clinical valida-
ent of treatment for invasive breast cancers > 1 cm in
tion of various standard combination chemotherapy
size. Combination chemotherapy exploits the Goldie–
regimens comprised of non-cross-resistant agents. Re-
cent clinical trials have demonstrated that treatment
doxorubicin and taxane resistant breast cancer patients
with combination chemotherapy can significantly pro-
long the lives of breast cancer patients. The degree
These observations suggest that the ability to
of improved clinical outcomes, however, is mod-
identify individual patterns of resistance prior to ini-
est and comparable among the various standard re-
tiating chemotherapy might have a substantial clinical
gimens [3, 4]. In a recently reported Inter Group
impact. Tailoring treatment regimens by eliminating
trial for node negative patients, the marginally super-
agents found to be inactive in vitro prior to therapy
ior disease free and overall survival with the CAF
administration would potentially avoid the toxicity,
regimen, compared to the CMF regimen, was bal-
lost time, and costs associated with ineffective treat-
anced by modestly increased toxicity [5]. For node
ment [25–27]. This is especially important in an era
positive patients, FAC/CAF, AC followed by paclit-
that has witnessed the introduction of a variety of
axel, doxorubicin followed by CMF, or CMF alone
new, non-cross-resistant classes of agents (taxanes
are all considered to be appropriate options [4, 6–
[28, 29], gemcitabine [30], and vinorelbine). Treat-
8]. The majority of randomized clinical trials have
ment with paclitaxel, vinorelbine, or docetaxel has led
failed to demonstrate a benefit from high dose chemo-
to similar durations of quality- adjusted progression-
therapy with stem cell rescue for high risk patients
free survival in anthracycline-resistant breast cancer
[31]. With the advent of more agents to choose from,
The inability to demonstrate a clear superiority of
and third-generation in vitro drug response assays, it
one regimen over another, or the superiority of high
may be possible to tailor combination therapy to the
dose combination regimens over standard dose chemo-
unique drug response characteristics of each patient’s
therapy, suggests that a plateau in benefit may have
tumor [32, 33]. For this potential to be realized, in vitro
been reached using the current non-targeted, empirical
assays must be evaluated for their ability to predict
approach to treatment selection. The empirical use of
one of the standard regimens for a specific patient does
Although the predictive accuracy of the in vitro ex-
not routinely take into account that patient’s unique tu-
treme drug resistance (EDR) assay to identify drugs
mor biology. On the other hand, treatment targeted to
unlikely to demonstrate clinical response with greater
the patient’s tumor characteristics holds promise. The
than 99% accuracy has been established in a double
initial proof of principle that targeted therapy could
blind retrospective study [33], there is paucity of data
be a useful strategy stemmed from observations that
on the relationship between EDR assay results and
tamoxifen treatment could significantly improve sur-
survival. The present study was, therefore, conducted
vival in patients with estrogen receptor (ER) positive
in breast cancer patients to examine the relationship
tumors [16]. In addition, the benefit of targeted treat-
between in vitro EDR assay results, and progression-
ment has been demonstrated in two retrospective trials
free and overall survival. EDR assay results were
where dose escalated doxorubicin-based chemother-
obtained for a serial cohort of 103 cases prior to first
apy was found to be superior in lymph node-positive
line chemotherapy. The treating physician was blinded
patients whose tumors overexpressed Her-2/neu [17,
to EDR results, and lab personnel were blinded to
18]. More importantly, Herceptin therapy targeted to
clinical characteristics. We report here the relationship
Her-2/neu overexpressing breast cancer patients has
between EDR assay results and patient outcomes after
yielded improved survival in a prospective randomized
treatment with agents tested in the assay.
trial when given in combination with cisplatin or pacl-itaxel chemotherapy [19]. These observations support
Patients and methods
the notion that tailoring treatment to each patient’stumor characteristics can be advantageous. Clinical
trials with cross over designs in breast cancer havevalidated the concept of individual patterns of drug-
Between October 1990 and March 1996, tissue
specific resistance, with some patients failing single
samples from 187 serial patients with newly diagnosed
agent paclitaxel, yet subsequently responding to non-
invasive breast cancer for which tumor tissue could be
cross resistant doxorubicin on cross over, or vice versa
obtained were sent from a single NSABP institution to
[20, 21]. Additionally, docetaxel has demonstrated
Oncotech, Inc. (Irvine, CA) for in vitro drug resistance
significant responses in doxorubicin resistant patients,
testing. We performed a retrospective double-blinded
while capecitabine has shown modest responses in
study on a serial group of patients who had specimens
In vitro drug response and breast cancer survival
submitted for EDR assays. Our primary objective was
viable malignant cells per well were suspended in soft
to determine if in vitro drug response was associ-
agarose and growth media in a 24-well plates and
ated with clinical outcomes. Treating physicians were
exposed to the following chemotherapeutic agents:
blinded to EDR results, as were the personnel who
doxorubicin, 5-FU, or 4-hydroxycyclophosphamide
collected clinical outcome data. EDR assays were
(4HC), the active metabolite of cyclophosphamide.
unsuccessful in 17 cases (9%). Thus, EDR results
Melphalan was employed as a cyclophosphamide sur-
were available for 170 patients (91%). Eleven patients
rogate for the first 10 cases because the 4-hydroperoxy
were lost to follow-up. Of the remaining 159 cases,
formulation of cyclophosphamide was not available
103 cases were treated with primary chemotherapy,
for in vitro use when this study was initiated. When
of which 96 cases had a complete EDR profile of 4-
4HC became available, a series of cases were run to
hydroxycyclophosphamide (4HC) and doxorubicin for
compare melphalan with 4HC on the same specimens.
patients treated with AC, or for 4HC and 5-fluorouracil
Using spearman’s correlation coefficient, a highly sig-
(5-FU) for patients treated with CMF.
nificant association was found between in vitro per-
Primary treatment consisted of mastectomy with
cent cell inhibition (PCI) produced by 4HC versus
axillary lymph node dissection, or lumpectomy with
melphalan (R = 0.43, p < 0.0001) (n = 468). Based
axillary node dissection and local radiation. A small
on this association, we included the in vitro response
(0.2–1 g) section of representative malignant tissue
data for the 10 cases tested against melphalan as a
from the primary tumor or involved lymph node was
placed in transport media and sent overnight to On-
Drugs were added to wells containing the malig-
cotech for analysis in the in vitro EDR assay. Chemo-
nant cells at doses that approximated their in vivo
therapy was started 14 to 21 days after definitive
peak plasma concentrations [32, 33]. Treated cell sus-
surgery. The following two regimens were employed:
pensions were incubated for 72 h with drug and thenpulsed with 5 µCi 3H-thymidine. After an additional
1. CMF – cyclophosphamide 100 mg/m2 days 1–
48-h incubation period, agarose-cell suspensions were
14, methotrexate 40 mg/m2 and 5-fluorouracil
liquefied at 96◦C, well contents were harvested onto
600 mg/m2, day 1 and day 8, every 28 days for
glass fiber filters, and cells were lysed with deionized
water. The incorporated radioactivity in the filter-
2. AC – cyclophosphamide 600 mg/m2 and doxoru-
trapped macromolecular DNA was measured by liquid
bicin 60 mg/m2, day 1 every 21 days for 4 cycles.
scintillation as counts per minute (CPM). Positive
White blood cell and platelet counts were monitored,
control (supralethal cisplatin-exposed) and negative
with dosages adjusted prior to each cycle if needed.
control (media-exposed) cultures were performed with
EDR assays were performed prior to the initiation
each assay. Results were reported as percent cell in-
of chemotherapy. Patients were subsequently treated
hibition (PCI) compared with media-exposed control
with classical CMF or AC regimens independent of
cultures after subtraction of positive control CPM. The
the assay results. Less than one third of the patients
performance characteristics, including the population
received hormone therapy, and these cases were bal-
median PCI and standard deviation (SD), were de-
anced between the two in vitro drug response groups
termined for 4HC (n = 372), 5-FU (n > 6,000) and
doxorubicin (n > 3,000) on independent cases evalu-ated using the same methods. Individual patient PCI
values were compared to the median and SD estab-lished for each agent to determine their EDR score.
Once received at Oncotech, tumor tissue sampleswere accessioned and assigned a tracking number. Tu-
mor specimens were mechanically disaggregated intosuspensions of small tumor clumps. Stained tissue
For each patient’s tumor specimen, in vitro responses
sections and cytospin preparations of tumor suspen-
to individual drugs were scored as ‘0’ for extreme
sions were reviewed by a pathologist to confirm the
drug resistance (EDR) when the PCI was ≥ 1SD below
diagnosis and the presence of adequate numbers of
the median, ‘1’ for intermediate drug resistance (IDR)
malignant cells. Tissue culture was performed as pre-
when the PCI was between the median and 1SD be-
viously described [32, 33]. Cell viability was determ-
low the median, or ‘2’ for low drug resistance (LDR)
ined by trypan blue exclusion. Approximately 30,000
when the PCI was above the median. EDR scores
for 4HC and doxorubicin were summed for patients
istical tests were two-tailed and a significance level of
treated with AC. 4HC and 5-FU scores were selected
0.05 was used. All clinical outcomes and laboratory
for summation for patients treated with CMF. Me-
data were independently reviewed by the Biostatistics
thotrexate was not tested in the EDR assay because
the addition of thymidine for labeling rescues DNAsynthesis, thereby yielding an inaccurate measure ofproliferation inhibition. Further, methotrexate has only
limited activity by itself, but it significantly potentiates5-FU toxicity when both compounds are administered.
Summed EDR Scores ranged from 0 to 4. For ex-
At a median duration of follow-up of 48.17 months,
ample, a patient treated with AC and having a tumor
there were 59 surviving patients out of 96 patients
with extreme resistance to 4HC and low resistance to
who had successful EDR assay results for at least two
doxorubicin was assigned an EDR Score of 0 + 2 = 2.
of the chemotherapy agents they received. Details ofpatient characteristics for the cohort of 96 patients
treated with chemotherapy, and for whom a completeEDR profile was available are detailed in Table 1.
We examined the relationship between the frequencies
Patients were treated with classical CMF or AC re-
of tumors with low resistance scores (4), or extreme
gimens. Some patients received additional hormone
to intermediate resistance scores (0–3), and patient
therapy. Treatment profiles are shown in Table 2.
clinical characteristics using contingency table ana-lysis with the chi-squared test or Fisher’s exact test.
Prognostic indicators considered as categorical vari-ables included age, stage, number of involved lymph-
Single agent EDR assay results for the 96 patients
nodes, tumor size, and ER receptor status. Similarly,
treated with chemotherapy that had summed EDR
we examined the association between the dichotom-
scores are shown in Table 3. The incidence of ex-
ized EDR scores and treatment modalities, including
treme drug resistance to the treatment drugs varied:
mastectomy versus lumpectomy/radiation, hormonal
13% for 4HC (or the index alkylator, Melphalan), 5%
treatment and chemotherapeutic regimen. Time to tu-
for doxorubicin, and 19% for 5-FU. The incidence of
mor progression and overall survival were calculated
intermediate resistance ranged from 25% to 32%, and
from the date of diagnosis to date of progression or
the incidence of low drug resistance ranged from 49%
death, respectively. For overall survival, death from
to 62%, respectively, for the individual drugs. The
any cause was considered as an event. Data from pa-
EDR scores for 4HC and doxorubicin were summed
tients without events were censored at the date of last
for patients treated with AC (n = 42), and EDR scores
follow up. Progression free and overall survival curves
for 4HC and 5-FU were summed for patients treated
were constructed using the Kaplan–Meier method, and
with CMF (n = 54). Table 4 shows the EDR assay
differences between groups were assessed by the log-
results and the corresponding summed EDR score cat-
rank test. Univariate analysis included age, stage,
egories for the study set. Fifty-five tumors (57%) ex-
degree of lymph node involvement, ER status, surgical
hibited extreme or intermediate drug resistance, with
treatment with or without radiation, chemotherapy re-
summed EDR scores for these cases ranging from 0 to
gimens, hormonal treatment status, and single agent
1 and 2 to 3. Of these tumors, only two demonstrated
EDR scores, and composite EDR scores. We used the
EDR to both drugs (summed EDR score of 0), and
Cox Proportional Hazards Model to evaluate the influ-
only eight cases showed EDR to one drug in conjunc-
ence of prognostic factors on survival in univariate and
tion with IDR to the other (summed EDR score of 1).
multivariate models. To assess the relative influence of
Forty-one (42%) patients were treated with a two-drug
prognostic factors on progression-free and overall sur-
combination to which their tumors showed low in vitro
vival, we included the variables that were predictive of
resistance (summed EDR score of 4). Patients with
survival in univariate analyses (EDR scores, stage and
summed EDR scores of 0 to 1 and 2 to 3 were grouped
lymph nodes) in multivariate models. We also used
into the extreme and intermediate resistance categor-
the log-rank test for trend to assess the association
ies, respectively, while patients with summed EDR
of progression-free survival, or overall survival, with
scores of 4 were placed into the low drug resistance
EDR scores trichotomized as 0–1, 2–3, and 4. All stat-
In vitro drug response and breast cancer survivalTable 1. Comparison of patient characteristics and summed EDR scores
Table 2. Comparison of treatment modalities related to summed EDR scores
Table 3. In vitro drug resistance profiles for single agents
treated with AC. For the 96 patients with successful
assays for two of the drugs they received (42 patients
received AC; 54 patients received CMF), their respect-ive summed EDR scores for intermediate and extreme
versus low drug resistance (0–3 vs. 4), lymph node
status, and stage were significantly associated with
progression-free and overall survival in univariate ana-lysis. Figure 1 and Table 5A show the influence of thelevel of drug resistance on time to tumor progression,
Table 4. Composite EDR scores profile
with a median of 100 months for patients with lowdrug resistance, compared to 48 months for patients
with intermediate to extreme-resistance (log-rank test
hazard ratio 2.05, CI = 1.110–3.747, p = 0.022). No
statistically significant difference was found between
the intermediate to extreme resistance and low drug
resistance categories with respect to age, lymph node
status, stage, size of primary tumor, ER status, primary
surgical, radiation, hormonal and chemotherapeutic
∗EDR: extreme drug resistance; IDR: intermediate drug resist-
treatment (Tables 1 and 2). However, there was a
trend in the intermediate to extreme-resistance groupfor smaller tumor size (p = 0.072), negative lymph-nodes (p = 0.246), and cases undergoing lumpectomy
Correlation of outcomes with EDR scores
and radiation rather than mastectomy (p = 0.058).
Of the evaluable cases with at least one successful drug
A significant difference in survival was noted
result in the EDR assay, 103 received primary chemo-
between patients with intermediate to extreme drug
therapy. At a median follow up time of 48 months,
resistance (summed EDR scores of 0–3), compared
37 of the 96 patients with full EDR profiles had died,
with the low drug resistance group (summed EDR
and 43 patients had progressed. Table 5, panels A
score of 4) in univariate analysis using log rank test
and B, show the association of EDR results for single
(p = 0.010) (Table 5B; Figure 2). Patients with inter-
agent 4HC and 5-FU with progression-free (p = 0.056
mediate to extreme-drug resistance demonstrated sig-
and p = 0.042) and overall survival (p = 0.078 and
nificantly shorter survival, with 5-year survival rates of
p = 0.005) for patients receiving a Cytoxan contain-
45% compared to 81% in patients with low drug resist-
ing regimen (n = 99) or a 5FU containing regimen
ance. Median survival was 50 months in the intermedi-
(n = 56), respectively. The association of survival and
ate to extreme-resistance group, while the median sur-
EDR results for single agent doxorubicin did not reach
vival for the low resistance group had not been reached
statistical significance (p = 0.286) for the 44 cases
Table 5A. Univariate analysis and progression-free survival
∗EDR score was summed for two of the agents received by the patient as described inMaterials and methods.
In vitro drug response and breast cancer survivalTable 5B. Univariate analysis and overall survival
∗EDR score was summed for two of the agents received by the patient as described inMaterials and methods.
log-rank test). Age, lymph node status, stage, ER
Discussion
status, and hormonal treatment status have all been re-ported to influence survival independent of the chemo-
This study demonstrated a significant association
therapeutic regimen used. In this cohort, stage and
between survival and EDR assay results for primary
lymph node status were the only other variables sig-
tumor tissues obtained from breast cancer patients
nificantly associated with progression-free and overall
prior to chemotherapy. The treatment of these pa-
survival (Tables 5A and 5B). The relative probab-
tients was blinded to assay results. With respect to
ility of progression and death was 2.19 (CI 1.24–
potential bias between groups, prognostic factors were
4.35, p = 0.022) and 2.49 (CI 1.18–5, p = 0.017) for
not found to be significantly different between pa-
patients treated with agents showing in vitro inter-
tients with intermediate to EDR (score 0–3) and LDR
mediate to extreme-resistance compared to patients
(EDR scores 4). However, there was a trend in the
treated with low drug resistance agents, using Cox
intermediate to EDR group for smaller tumor size
proportional hazards model (data not shown).
(p = 0.072) and presentation with negative lymph-
In view of the significant association between
nodes (p = 0.246), compared to patients in the LDR
the dichotomous EDR score categories of 0–3 and
group. More patients, therefore, underwent lumpec-
4 variable and progression free and overall survival,
tomy and radiation in the high resistance group as
we evaluated the trichotomous variables of low, in-
opposed to higher numbers of patients undergoing
termediate, and extreme resistance using summed
mastectomy in the low resistance group. This trend
EDR scores of 4, 2–3, and 0–1, respectively. As
may have potentially biased results against an associ-
shown in Figures 2A and 2B, the log-rank test for
ation between EDR assay results and survival. Using
trend demonstrated a significant association between
a Cox Proportional Hazards model adjusting for the
these three resistance categories and progression-free
variables significant in univariate analysis, the relative
(p = 0.013) and overall survival (p = 0.002), respect-
risk of death for patients with adverse EDR scores of
ively. Table 6A depicts the results of analysis using
0–1 and 2–3 was 3- and 2-fold higher, respectively,
the Cox proportional hazards model for progression-
compared with patients with a favorable EDR score of
free survival for summed EDR scores of 0–1 and 2–3
versus summed EDR scores of 4 (Relative risk 2.60,
In vitro patterns of resistance varied among pa-
CI 0.94–7.22, p = 0.066 and Relative risk 2.09, CI
tients, with few patients showing resistance to all
1.04–4.24, p = 0.039, respectively), adjusted for stage
drugs tested, suggesting that alternative agents may
and lymph node status. Similarly, Table 6B illustrates
have been available to chose from for a majority of
Cox proportional hazards model showing that EDR
patients when one specific agent was found to be in-
scores were independent predictors of survival when
active in vitro for a given patient. Further, there was
patients with extreme and intermediate drug resistance
a significant association between in vitro drug res-
were compared with patients with low drug resistance
istance for single agent 5-FU and progression-free
(Relative risk 3.09, 95%, CI 1.05–9.06, p = 0.040
(p < 0.0423) and overall survival (p < 0.005) of pa-
and Relative risk 2.35, 95%, CI 1.07–5.15, p = 0.033,
tients treated with CMF, suggesting that the clinical
activity of 5-FU in the CMF regimen may be a ma-jor determinant of outcome for patients treated with
Figure 1. (a) Kaplan–Meier progression-free survival curves for patients with EDR scores of 4 (—–) vs. < 4 (—-); (b) Kaplan–Meier overallsurvival curves for patients with EDR scores of 4 (—–) vs. < 4 (—-).
CMF. We also noted that single agent 4HC EDR
methotrexate acted as a modulator of 5-FU or 4HC
scores showed a trend towards a significant associ-
cytotoxicity. Absence of in vitro assay results for me-
ation with progression-free (p < 0.056) and overall
thotrexate did not detract from the robust nature of
survival (p < 0.078) for patients treated with AC or
in vitro 4HC or 5-FU response association with PF
CMF. Because methotrexate cannot be reliably tested
and OS. The significant relationship between in vitroin vitro, it was not possible for us to evaluate if
drug resistance scores and survival supports the no-
In vitro drug response and breast cancer survivalFigure 2. (a) Kaplan–Meier progression free survival curves for patients with EDR scores of 4 vs. 2–3 vs. 0–1; (b) Kaplan–Meier overallsurvival curves for patients with EDR scores of 4 vs. 2–3 vs. 0–1. Table 6A. Progression-free survival: Multivariate analyses of
The drug exposures used in the EDR assay are 5–
10 times higher than those achieved in vivo, biasing
assay reliability towards accurate detection of drug
resistance. In correlating in vitro drug resistance withclinical response, only 1 out of 127 patients showing
in vitro EDR showed clinical response, while 52%
of patients showing in vitro sensitivity demonstrated
clinical response. The prediction of resistance may be
more robust than the prediction of sensitivity because
of the inability of in vitro systems to parallel relevant
in vivo pharmacodynamics, such as individual vari-
ations in tumor vascular supply and drug metabolism,that influence clinical response. The practical utilityof in vitro testing has been enhanced by the devel-opment of third generation assay techniques, such as
Table 6B. Overall survival: Multivariate analyses of prognostic
the EDR assay employed in this study. While older
clonogenic systems yielded results in 2–3 weeks with50% success rates, newer technologies have shortened
assay time to less than one week and improved the
evaluability rate to 85%, which is similar to the eval-
uability rate of 91% in the present study [27]. Yet,
the relationship between in vitro results and survival
has not been adequately addressed either by chemo-
sensitivity or chemoresistance assays. Our study is the
first large series to demonstrate the clinical relevance
of in vitro drug resistance for patients with all stages
of breast cancer treated with first line chemotherapy.
We found that patients treated with combinations ofdrugs with low in vitro drug resistance enjoy betterprogression-free and overall survival. Patients whowere treated with combinations of drugs found to be
tion that drug resistance testing can identify a tumor
intermediate or extremely resistant in the EDR assay
phenotype related to clinical outcome. Information re-
had a 5-year survival rate of only 45%, compared
garding the unique in vitro drug response profile of an
to 81% for patients who were treated with a com-
individual patient may potentially be exploited to im-
bination of drugs to which their tumors showed low
prove outcomes by tailoring treatment based on assay
The improved survival demonstrated for patients
Several smaller studies have indicated that re-
treated with combinations of low resistance agents
sponse rates are improved when patients received
is intriguing. In a recent review, 12 of 17 studies
chemotherapy to which their tumors were not res-
were found to demonstrate a statistically significant
istant in vitro [27, 33–35]. A review of published
survival advantage for patients treated with agents
in vitro assay results for 4,263 patients, where correla-
to which they were ‘sensitive’ in vitro [27]. Three
tions with treatment response were available, indicated
prospective studies, two of which were randomized,
that clinical response rates were significantly associ-
showed a survival advantage for patients treated with
ated with in vitro results, with an overall sensitivity
assay-directed therapy [27]. More recently, a random-
of 85%, and an overall specificity of 80% [27]. Of
ized study by Cortazar demonstrated that survival was
note was the finding that prediction of drug resistance
improved for small-cell lung cancer patients random-
was > 90% accurate, compared to 72% accuracy for
ized to assay directed therapy [36]. Orr et al., have
prediction of chemosensitivity. The EDR assay was
shown that costs can be lowered using assay direc-
reported to have a negative predictive accuracy of 99%
ted therapy, with at least equivalent survival in newly
in a double-blind retrospective study of 450 cases [33].
diagnosed, optimally resected ovarian cancer patients
In vitro drug response and breast cancer survival
[25]. Gambino et al., demonstrated high response rates
The following authors have a financial interest in
with assay directed therapy in patients with chemo-
Oncotech, the Principle Sponsor of this study: R.
therapy refractory gynecological malignancies [37].
Mehta, I.Y. Yu, R. Parker, and J.P. Fruehauf.
Similarly, a prospective trial by Kurbacher et al.,demonstrated a high response rate and promising sur-vival outcomes in recurrent ovarian cancer treated withtherapy tailored according to their in vitro assay res-
References
ults [38]. One shortcoming of in vitro testing is the
Goldie JH, Coldman AJ: A mathematic model for relating the
necessity of obtaining adequate amounts of malig-
drug sensitivity of tumors to the spontaneous mutation rate.
nant tissue for cell culture, which limited the EDR
testing to those with tumors ≥ 0.5 cm in size. How-
Goldie JH, Coldman AJ, Gadauskas GA: Rationale for the use
of alternating non-cross-resistant chemotherapy. Cancer Treat
increasingly being detected mammographically, are
Fisher F, Brown AM, Dimitrov NV, Poisson R, Redmond
not routinely considered to be candidates for chemo-
C, Margolese RG, Bowman D, Wolmark N, Wickerham DL,
therapy. A second shortcoming of this study was the
Kardinal CG: Two months of doxorubicin-cyclophosphamidewith and without interval reinduction therapy compared to
absence of HER2 profiling, which may affect the clin-
6 months of cyclophosphamide, methotrexate, and fluor-
ical outcome in patients treated with AC. Because
ouracil in node-positive breast cancer patients with tamoxifen-
HER2 was not routinely tested at the time we began
nonresponsive tumors. Results from the National Surgical
this study, these data are not available.
Adjuvant Breast and Bowel Project B-15. J Clin Oncol 8:1483–1496, 1990
Our study was performed in newly diagnosed
Early Breast Cancer Trialists’ Collaborative Group: Poly-
breast cancer patients. Our finding of a significant as-
chemotherapy for early breast cancer: an overview of the
sociation between survival and in vitro drug resistance
randomized trials. Lancet 352: 930–942, 1998
to the agents used clinically suggests that completing
Hutchins L, Green S, Ravdin P, Lew D, Martino S, Abeloff M,Lyss A, Henderson C, Allred C, Dakhil S, Pierce I, Goodwin
4–6 cycles of ineffective adjuvant chemotherapy may
W, Caton J, Rivkin S, Chapman R, Osborne K: CMF versus
adversely delay selection of effective chemotherapy,
CAF with and without tamoxifen in high-risk node-negative
potentially induce or select for additional chemores-
breast cancer and a natural history follow-up study in low-risk
istance, and may also decrease the patient’s capacity
node-negative patients: first results of Intergroup Trial INY0102. Proc Am Soc Clin Oncol 17: 1a, 1998 (abstr 2)
to undergo further therapy. EDR assay results iden-
Henderson IC, Berry D, Demetri G, Cirrincione C, Goldstein
tified patients with inferior survival after treatment
L, Martino S, Ingle JN, Cooper MR, Canellos G, Borden E,
with agents their tumor was resistant to in vitro. The
Fleming G, Holland JF, Graziano S, Carpenter J, Muss H,
clinical utility of this finding may stem from the elim-
Norton L: Improved disease-free (DFS) and overall survival(OS) from the addition of sequential paclitaxel (T) but not
ination of such agents from treatment planning. In
from dose escalation of doxorubicin (A) dose level in the
addition, such testing may identify alternative forms
adjuvant chemotherapy of patients (pts) with node-positive
of treatment with a greater probability of success.
primary breast cancer (BC) (abstract). Proc Am Soc ClinOncol 17: 101a, 1998 (abstr 390)
This is of major importance when considering the re-
Carlson RW, Goldstein LJ, Gradishar WJ, Lichter AS, Mc-
cent introduction of several new non-cross resistant
Cormick B, Moe RE, Theriault RL: NCCN breast cancer prac-
drugs into clinical practice. Our study was performed
tice guidelines. The national comprehensive cancer network.
when fewer chemotherapeutic choices were available
Anderson BO, Bensinger W, Cox CE, Davidson NE, Edge
for first line treatment of breast cancer. The utility
SB, Farrar WB, Goldstein LJ, Gradishar WJ, Lichter AS, Mc-
of in vitro testing is increased with the addition of
Cormick B, Nabell LM, Reed EC, Silver SM, Smith ML,
these newer agents. While we await the results of fu-
Somlo G, Theriault R, Ward JH, Winer EP, Wolff A: Update:
ture randomized trials of assay directed treatment, it
NCCN Practice Guidelines for Breast Cancer. Oncology 14(11Suppl): 33–49, 2000
is logical to conclude that the risk/benefit ratio favors
Hortabagyi GN, Buzdar AU, Champlin R, Gajewski J, Holmes
the utility of EDR assay results when considering the
FA, Booser D, Valero V, Theriault RL: Lack of efficacy of
elimination of ineffective treatment options for breast
adjuvant high dose (HD) tandem combination chemotherapy
(CT) for high risk primary breast cancer – a randomized trial(abstract). Proc Am Soc Clin Oncol 17: 123a, 1998 (abstr 471)
Rodenhuis S, Richel DJ, van der Wall E, Schornagel JH, Baars
Acknowledgements
JW, Koning CC, Peterse JL, Borger JH, Nooijen WJ, Bakx R,Dalesio O, Rutgers E: Randomized trial of high-dose chemo-therapy and hematopoietic progenitor-cell support in operable
This study was supported, in part, by a grant from
breast cancer with extensive axillary lymph-node involvement.
Peters W, Rosner G, Vredenburgh J, Shpall E, Crump M,
Ravdin P, Burris HA, Cook G, Eisenberg P, Kane M,
Richardson P, Marks L, Cirrincione C, Wood W, Henderson
Bierman WA, Mortimer J, Genevois E, Bellet RE: Phase
I, Hurd D, Norton L: A prospective, randomized comparison
II trial of docetaxel in advanced anthracycline-resistant or
of two doses combination alkylating agents (AA) as consolid-
anthracenedione-resistant breast cancer. J Clin Oncol 13:
ation after CAF in high-risk primary breast cancer involving
ten or more axillary lymph nodes (LN): Preliminary results of
Valero V, Holmes FA, Walters RS, Theriault RL, Esparza
CALGB 9082/SWOG 9114/NCIC MA-13. Proc Am Soc Clin
L, Fraschini G, Fonseca GA, Bellet RE, Buzdar AU, Horto-
bagyi GN: Phase II trial of docetaxel: A new, highly effect-
Bezwoda WR: Randomized, controlled trial of high dose
ive antineoplastic agent in the management of patients with
chemotherapy (HD-CNVp) vs. standard dose (CAF) chemo-
anthracycline-resistant metastatic breast cancer. J Clin Oncol
therapy for high risk, surgically treated, primary breast cancer.
Proc Am Soc Clin Oncol 18: 2a, 1999 (abstr 4)
Blum JL, Jones SE, Buzdar AU, LoRusso PM, Kuter I, Vogel
The Scandinavian Breast Study Group 9401: Results from
C, Osterwalder B, Burger HU, Brown CS, Griffin T: Multi-
a randomized adjuvant breast cancer study with high dose
center phase II study of capecitabine in paclitaxel-refractory
chemotherapy with CTCb supported by autologous bone mar-
metastatic breast cancer. J Clin Oncol 17: 485–493, 1999
row stem cells versus dose escalated and tailored FEC therapy.
Orr JW, Orr P, Kern D: Cost-effective treatment of women
Proc Am Soc Clin Oncol 18: 2a, 1999 (abstr 3)
with advanced breast cancer by cytoreductive surgery and
Lotz J-P, Curé H, Janvier M, Morvan F, Asselain B, Guillemot
chemotherapy directed by an in vitro assay for drug resistance.
M, Laadem A, Maraninchi D, Gisselbrecht C, Roché H: High-
Dose Chemotherapy (HD-CT) with hematopoietic stem cells
DeVita VT Jr: In: DeVita, Hellman, Rosenberg (eds), Cancer:
transplantation (HSCT) for metastatic breast cancer: Results
Principles and Practice of Oncology. 5th edn, Lippincott-
of the French Protocol Pegase 04. Proc Am Soc Clin Oncol
Raven Publishers, Philadelphia, 1997, 345 p
Fruehauf JP, Bosanquet AG: In vitro determination of drug
Stadtmauer EA, O’Neill A, Goldstein PG, Crilley P, Man-
response: A discussion of clinical applications, In: DeVita VT
gan KF, Ingle JN, Lazarus HM, Erban J, Sickles C, Glick
Jr, Hellman S, Rosenberg SA (eds), Principles and Practice of
JH: Phase III Randomized trial of high-dose chemotherapy
Oncology Updates, 4th edn, JB Lippincott, Philadelphia, PA,
(HDC) and stem cell support (SCT) shows no difference in
overall survival or severe toxicity compared to maintenance
Seidman AD, Reichman BS, Crown JP, Yao TJ, Currie V,
chemotherapy with cyclophosphomide, methotrexate and 5-
Hakes TB, Hudis CA, Gilewski TA, Baselga J, Forsythe P,
fluorouracil (CMF) for women with metastatic breast cancer
et al.: Paclitaxel as second and subsequent therapy for meta-
who are responding to conventional induction chemotherapy:
static breast cancer: activity independent of prior anthracycline
The Philadelphia Intergroup Study (PBT-01), ECOG, U. of
response. J Clin Oncol 13: 1152–1159, 1995
Pennsylvania. Proc Am Soc Clin Oncol 18: 1a, 1999 (abstr
Seidman AD, Hudis CA, Norton L: Memorial Sloan Ketter-
ing Cancer Center experience with paclitaxel in the treatment
Early Breast Cancer Trialists’ Collaborative Group: Tamox-
of breast cancer: from advanced disease to adjuvant therapy.
ifen for early breast cancer: an overview of the randomized
trials. Lancet 351(9114): 1451–1467, 1998
Mavroudis D, Malamos N, Alexopoulos A, Kourousis C,
Thor AD, Berry DA, Budman DR, Muss HB, Kute T, Hender-
Agelaki S, Sarra E, Potamianou A, Kosmos C, Rigatos G, Gi-
son IC, Barcos M, Cirrincione C, Edgerton S, Allred C, Norton
annakakis T, Kalbakis K, Apostolaki F, Vlachonicolis J, Kako-
L, Liu ET: erbB-2, p53, and efficacy of adjuvant therapy
lyris S, Samonis G, Georgoulias V: Salvage chemotherapy
in lymph node-positive breast cancer. J Natl Cancer Inst 90:
in anthracycline-pretreated metastatic breast cancer patients
with docetaxel and gemcitabine. Ann Oncol 10: 211–215,
Paik S, Bryant J, Park C, Fisher B, Tan-Chiu E, Hyams D,
Fisher ER, Lippman ME, Wickerham DL, Wolmark N: erbB-
Leung PP, Tannock IF, Oza AM, Puodziunas A, Dranitsaris
2 and response to doxorubicin patients with axillary lymph
G: Cost-Utility analysis of chemotherapy using paclitaxel,
node-positive, hormone receptor-negative breast cancer. J Natl
docetaxel, or vinorelbine for patients with Anthracycline-
resistant breast cancer. J Clin Oncol 17: 3082–3090, 1999
Norton L, Slamon D, Leyland-Jones B, Wolter J, Fleming T,
Kern DH, Drogemuller CR, Kennedy MC, Hildebrand-Zanki
Eirmann W, Baselga J, Mendelsohn J, Bajamonde A, Ash
SU, Tanigawa N, Sondak VK: Development of a miniatur-
M, Shak S: Overall survival (OS) advantage to simultan-
ized, improved nucleic acid-precursor incorporation assay for
eous chemotherapy (CRx) plus the Humanized Anti-HER2
chemosensitivity testing of human solid tumors. Cancer Res
Monoclonal Antibody Herceptin (H) in HER2-Overexpressing
(HER2 +) metastatic breast cancer (MBC). Proc Am Soc Clin
Kern DH, Weisenthal LM: Highly specific prediction of an-
tineoplastic drug resistance with an in vitro assay using
Sledge GW Jr, Neuberg D, Ingle J, Martino S, Wood W:
suprapharmacologic drug exposures. J Natl Cancer Inst 82:
Phase III trial of doxorubicin vs. paclitaxel vs. doxoru-
bicin + paclitaxel as first-line therapy for metastatic breast
Elledge RM, Clark GM, Hon J, Thant M, Belt R, Maguire YP,
cancer. Proc Am Soc Clin Oncol 16: 1a, 1997 (abstr 2)
Brown J, Bartels P, Von Hoff DD: Rapid in vitro assay for
Gammuci T, Piccart M, Brüning P, Klijn J, Biganzoli L, Hous-
predicting response to fluorouracil in patients with metastatic
ton S, Coleman R, Van Vreckem A, Cleall S, Curran D, Awada
breast cancer. J Clin Oncol 17: 419–423, 1995
A, Paridaens R: Single agent taxol (T) versus doxorubicin
Cortazar P, Johnson BE: Review of the efficacy of indi-
(D) as first-line chemotherapy (CT) in advanced breast cancer
vidualized chemotherapy selected by in vitro drug sensitivity
(ABC): result of an EORTC randomized study with crossover.
testing for patients with cancer. J Clin Oncol 17: 1125–1631,
Proc Am Soc Clin Oncol 17: 11a, 1998 (abstr 428)
In vitro drug response and breast cancer survival
Cortazar P, Gazdar AF, Woods E, Russell E, Steinberg SM,
Wilhelm LM, Engel H, Mallmann PK, Andreotti PE: A
Williams J, Ihde DC, Johnson BE: Survival of patients with
prospective clinical trial on individualized chemotherapy
limited-stage small cell lung cancer treated with individualized
for recurrent ovarian cancer selected by the Use of an
chemotherapy selected by in vitro drug sensitivity testing. Clin
ex vivo ATP luminescence assay to direct chemotherapy
for recurrent ovarion cancer. Anticancer Drugs 9: 51–57,
Gambino A, Favalli G, Salinaro, Pecorelli S: The use of Ex-
treme Drug Resistance Assay in Gynecologic malignanciesafter failure of conventional chemotherapy. IGCS Oncol 17:F139a, 1999 (abstr)
Address for offprints and correspondence:
Kurbacher CM, Bruckner HW, Cree IA, Bruckner HW,
Oncotech, Inc., 1791 Kaiser Avenue, Irvine, CA 92614; Tel.:
Brenne U, Kurbacher JA, Muller K, Ackermann T, Gilster TJ,
949-474-9262; E-mail: [email protected]
INTERNATIONAL JOURNAL OF PSYCHOTHERAPHY, VOL. 5, NO. 2, 2000 An inspired resurrection of Freudian drive theory: but does Nick Totton’s Reichian `bodymind’ concept supersede Cartesian dualism? Review article on Nick Totton’s The Water in the Glass: body and mind in psychoanalysis , London: Rebus Press, 1998, 266 pp., ISBN: L 900877 L2 0 Minster Centre/Scarborough Psychotherapy Training
Bij andere (chronische) ziektes is de kans op een ernstiger verloop van de griep geringer en wordt de griepprik niet vergoed. Ook is er geen vergoeding voor beroepsgroepen die misschien een hogere kans op het krijgen van griep hebben (bijvoorbeeld werkers in de De kans om griep te krijgen wordt kleiner wanneer u een goede weerstand hebt opgebouwd. Een goede weerstand Behoort u niet tot de i
 Breast Cancer Research and Treatment 66: 225–237, 2001.
Breast Cancer Research and Treatment 66: 225–237, 2001.









 In vitro drug response and breast cancer survival
Table 1. Comparison of patient characteristics and summed EDR scores
Table 2. Comparison of treatment modalities related to summed EDR scores
In vitro drug response and breast cancer survival
Table 1. Comparison of patient characteristics and summed EDR scores
Table 2. Comparison of treatment modalities related to summed EDR scores








 Table 3. In vitro drug resistance profiles for single agents
treated with AC. For the 96 patients with successful
assays for two of the drugs they received (42 patients
received AC; 54 patients received CMF), their respect-ive summed EDR scores for intermediate and extreme
versus low drug resistance (0–3 vs. 4), lymph node
status, and stage were significantly associated with
progression-free and overall survival in univariate ana-lysis. Figure 1 and Table 5A show the influence of thelevel of drug resistance on time to tumor progression,
Table 4. Composite EDR scores profile
with a median of 100 months for patients with lowdrug resistance, compared to 48 months for patients
with intermediate to extreme-resistance (log-rank test
hazard ratio 2.05, CI = 1.110–3.747, p = 0.022). No
statistically significant difference was found between
the intermediate to extreme resistance and low drug
resistance categories with respect to age, lymph node
status, stage, size of primary tumor, ER status, primary
surgical, radiation, hormonal and chemotherapeutic
∗EDR: extreme drug resistance; IDR: intermediate drug resist-
treatment (Tables 1 and 2). However, there was a
trend in the intermediate to extreme-resistance groupfor smaller tumor size (p = 0.072), negative lymph-nodes (p = 0.246), and cases undergoing lumpectomy
Correlation of outcomes with EDR scores
and radiation rather than mastectomy (p = 0.058).
Table 3. In vitro drug resistance profiles for single agents
treated with AC. For the 96 patients with successful
assays for two of the drugs they received (42 patients
received AC; 54 patients received CMF), their respect-ive summed EDR scores for intermediate and extreme
versus low drug resistance (0–3 vs. 4), lymph node
status, and stage were significantly associated with
progression-free and overall survival in univariate ana-lysis. Figure 1 and Table 5A show the influence of thelevel of drug resistance on time to tumor progression,
Table 4. Composite EDR scores profile
with a median of 100 months for patients with lowdrug resistance, compared to 48 months for patients
with intermediate to extreme-resistance (log-rank test
hazard ratio 2.05, CI = 1.110–3.747, p = 0.022). No
statistically significant difference was found between
the intermediate to extreme resistance and low drug
resistance categories with respect to age, lymph node
status, stage, size of primary tumor, ER status, primary
surgical, radiation, hormonal and chemotherapeutic
∗EDR: extreme drug resistance; IDR: intermediate drug resist-
treatment (Tables 1 and 2). However, there was a
trend in the intermediate to extreme-resistance groupfor smaller tumor size (p = 0.072), negative lymph-nodes (p = 0.246), and cases undergoing lumpectomy
Correlation of outcomes with EDR scores
and radiation rather than mastectomy (p = 0.058).

 In vitro drug response and breast cancer survival
Table 5B. Univariate analysis and overall survival
∗EDR score was summed for two of the agents received by the patient as described inMaterials and methods.
In vitro drug response and breast cancer survival
Table 5B. Univariate analysis and overall survival
∗EDR score was summed for two of the agents received by the patient as described inMaterials and methods.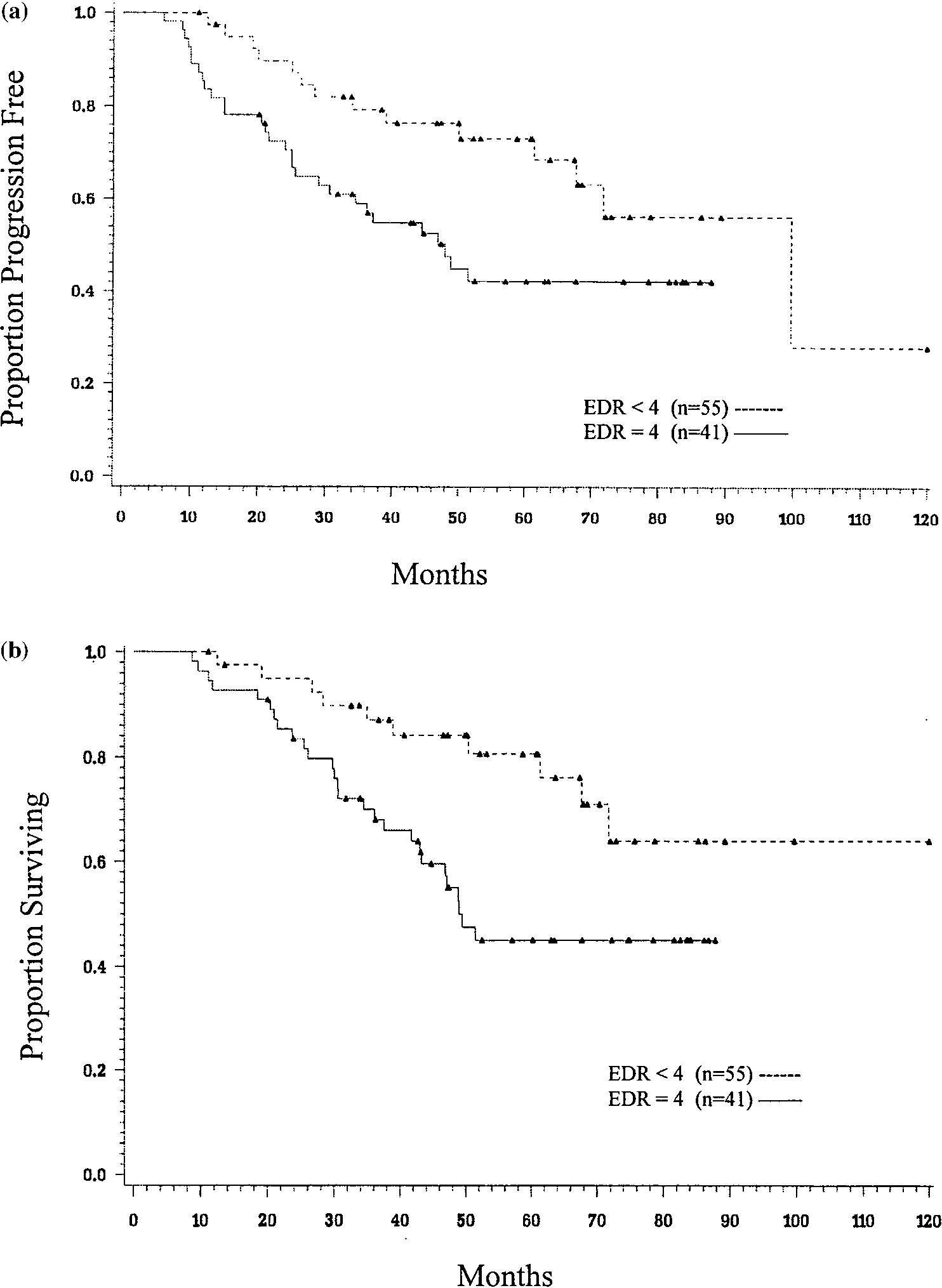 Figure 1. (a) Kaplan–Meier progression-free survival curves for patients with EDR scores of 4 (—–) vs. < 4 (—-); (b) Kaplan–Meier overallsurvival curves for patients with EDR scores of 4 (—–) vs. < 4 (—-).
Figure 1. (a) Kaplan–Meier progression-free survival curves for patients with EDR scores of 4 (—–) vs. < 4 (—-); (b) Kaplan–Meier overallsurvival curves for patients with EDR scores of 4 (—–) vs. < 4 (—-).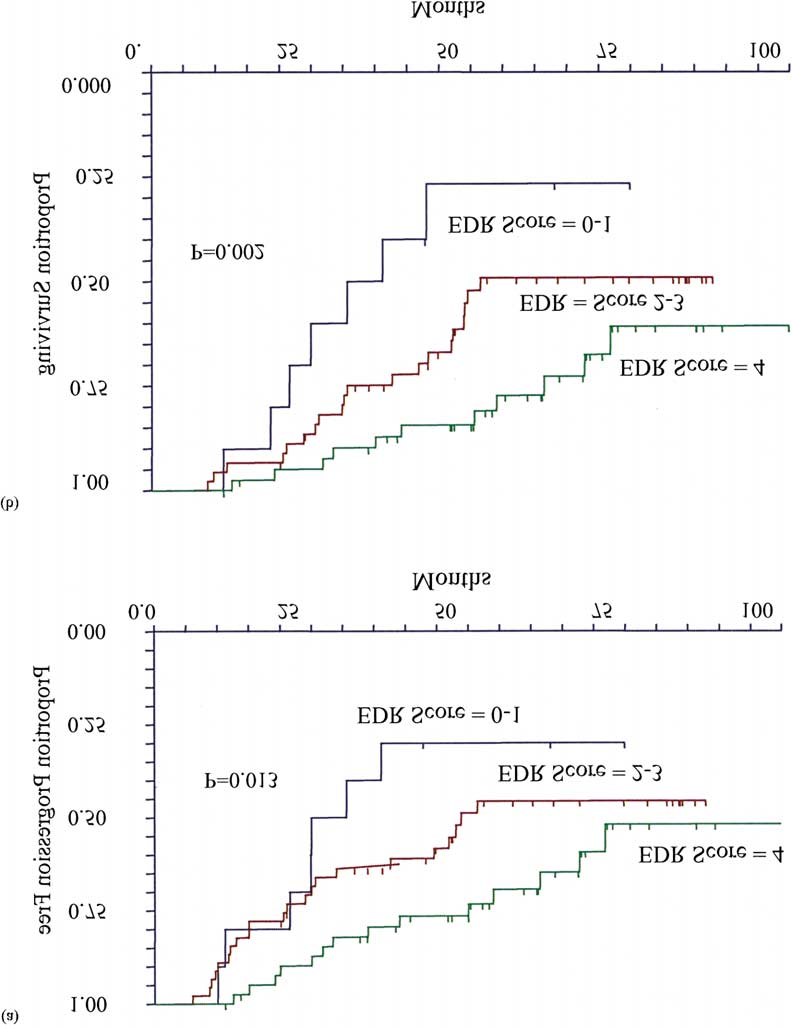 In vitro drug response and breast cancer survival
Figure 2. (a) Kaplan–Meier progression free survival curves for patients with EDR scores of 4 vs. 2–3 vs. 0–1; (b) Kaplan–Meier overallsurvival curves for patients with EDR scores of 4 vs. 2–3 vs. 0–1.
In vitro drug response and breast cancer survival
Figure 2. (a) Kaplan–Meier progression free survival curves for patients with EDR scores of 4 vs. 2–3 vs. 0–1; (b) Kaplan–Meier overallsurvival curves for patients with EDR scores of 4 vs. 2–3 vs. 0–1.




 Table 6A. Progression-free survival: Multivariate analyses of
The drug exposures used in the EDR assay are 5–
10 times higher than those achieved in vivo, biasing
assay reliability towards accurate detection of drug
resistance. In correlating in vitro drug resistance withclinical response, only 1 out of 127 patients showing
in vitro EDR showed clinical response, while 52%
of patients showing in vitro sensitivity demonstrated
clinical response. The prediction of resistance may be
more robust than the prediction of sensitivity because
of the inability of in vitro systems to parallel relevant
in vivo pharmacodynamics, such as individual vari-
ations in tumor vascular supply and drug metabolism,that influence clinical response. The practical utilityof in vitro testing has been enhanced by the devel-opment of third generation assay techniques, such as
Table 6B. Overall survival: Multivariate analyses of prognostic
the EDR assay employed in this study. While older
clonogenic systems yielded results in 2–3 weeks with50% success rates, newer technologies have shortened
assay time to less than one week and improved the
evaluability rate to 85%, which is similar to the eval-
uability rate of 91% in the present study [27]. Yet,
the relationship between in vitro results and survival
has not been adequately addressed either by chemo-
sensitivity or chemoresistance assays. Our study is the
first large series to demonstrate the clinical relevance
of in vitro drug resistance for patients with all stages
of breast cancer treated with first line chemotherapy.
Table 6A. Progression-free survival: Multivariate analyses of
The drug exposures used in the EDR assay are 5–
10 times higher than those achieved in vivo, biasing
assay reliability towards accurate detection of drug
resistance. In correlating in vitro drug resistance withclinical response, only 1 out of 127 patients showing
in vitro EDR showed clinical response, while 52%
of patients showing in vitro sensitivity demonstrated
clinical response. The prediction of resistance may be
more robust than the prediction of sensitivity because
of the inability of in vitro systems to parallel relevant
in vivo pharmacodynamics, such as individual vari-
ations in tumor vascular supply and drug metabolism,that influence clinical response. The practical utilityof in vitro testing has been enhanced by the devel-opment of third generation assay techniques, such as
Table 6B. Overall survival: Multivariate analyses of prognostic
the EDR assay employed in this study. While older
clonogenic systems yielded results in 2–3 weeks with50% success rates, newer technologies have shortened
assay time to less than one week and improved the
evaluability rate to 85%, which is similar to the eval-
uability rate of 91% in the present study [27]. Yet,
the relationship between in vitro results and survival
has not been adequately addressed either by chemo-
sensitivity or chemoresistance assays. Our study is the
first large series to demonstrate the clinical relevance
of in vitro drug resistance for patients with all stages
of breast cancer treated with first line chemotherapy.