Neurol Med Chir (Tokyo) 50, 622¿626, 2010
Intravenous Methylprednisolone Reduces the Risk of
Propofol-Induced Adverse Effects During Wada Testing
Nobuhiro MIKUNI, Youhei YOKOYAMA, Atsuhito MATSUMOTO,
Takayuki KIKUCHI, Shigeki YAMADA, Nobuo HASHIMOTO*,
Department of Neurosurgery, Kyoto University Graduate School of Medicine, Kyoto;
*National Cerebral and Cardiovascular Center, Suita, Osaka
The adverse effects and risks associated with intracarotid propofol injection during Wada testing wereretrospectively compared in two groups of patients with (n = 75) and without (n = 58) intravenousmethylprednisolone administered before intracarotid propofol injection. The incidences of all adverseeffects were decreased in the methylprednisolone group. In particular, severe adverse effects such as in-creased muscle tone with twitching and rhythmic movements or tonic posture, which could adverselyaffect Wada test results, were seen in one patient in the methylprednisolone group and seven patients inthe control group, indicating 92% risk reduction. This study suggests that Wada testing using in-travenous methylprednisolone administration prior to propofol injection is a safe approach to thepreoperative evaluation of brain tumors, epilepsy, and arteriovenous malformations.
The Wada test, a direct intracarotid amobarbital in-
jection that induces transient anesthesia in a singlecerebral hemisphere,11) has been the gold standard
The clinical records were retrospectively examined
for lateralization of hemispheric speech and memo-
of all 75 patients (44 men and 31 women), aged 10 to
ry dominance. Although amobarbital has been com-
74 years, who underwent the Wada test from 2006 to
monly used for this purpose, its limited availability
2008 as part of a preoperative examination. The
due to worldwide shortages has led to the explora-
population included 43 patients with brain tumors,
tion of alternative agents such as propofol,10) metho-
18 patients with temporal or frontal lobe epilepsy,
hexital,2) and etomidate.6) We have previously report-
and 14 patients with arteriovenous malformations
ed the clinical utility of an intracarotid propofol test
(AVMs). Fifty-eight patients who underwent the
for speech and memory dominance with a moderate-
Wada test from 2001 to 2005 using intracarotid
ly high risk of adverse effects.8) Previous research
has suggested that propofol infusion is likely to
formed the control group in this study. Adverse ef-
cause a considerably high incidence of adverse ef-
fects of the control group were reported previously.8)
fects, although no data on adverse effects for
None of the patients had received steroids before the
amobarbital equivalents has been provided.5)
The present study evaluated the efficacy of
The methylprednisolone group received an in-
methylprednisolone for improving the safety of
travenous bolus injection of 500 mg (or 250 mg for
propofol administration during the Wada test by
children 15 years of age and younger) methylpred-
comparing outcome measures of 75 patients who
nisolone at most 5 minutes prior to propofol ad-
received methylprednisolone (methylprednisolone
ministration. The Wada test was then performed
group) to those of 58 patients who did not (control
using the propofol-based protocol reported previous-ly.8,10) Propofol was administered as a 10 ml saline
suspension at a concentration of 1 mg/ml. If this
dose did not induce contralateral hemiplegia, addi-
Intravenous Methylprednisolone During Wada Testing
tional propofol was injected immediately, up to a
eye version. Grade 3 adverse effects included in-
maximum dose of 15 mg in one side. All patients in
creased muscle tone with twitching and rhythmic
both groups received equal total propofol injection
movements or tonic posture. To evaluate the poten-
volumes bilaterally except for one patient in the con-
tial risks of propofol injection, the odds ratios and
trol group who suffered strong adverse effect after
95% confidence intervals (CIs) associated with vari-
the first propofol dose, and so did not receive a sec-
ous demographic variables were calculated, such as
ond injection. Total propofol injection volume (me-
sex, age, history of convulsions, lesion type, lesion
an ± standard deviation) was 22.7 ± 3.8 mg in the
laterality, laterality of language function, relation-
methylprednisolone group and 20.8 ± 3.7 mg in the
ship between the laterality of the lesion and the lan-
guage center, and injection volume (total, first injec-
Clinical characteristics of the two groups were
tion, and second injection), using SAS version 8.2
compared using the x2 test at a significance level of p
software (SAS Institute, Cary, N.C., U.S.A.). P values
º 0.05. The results showed no significant difference
less than 0.05 were considered to be statistically sig-
in underlying disease, sex, history of epilepsy, lesion
nificant in each analysis, whereas p values equal to
laterality, speech dominance, or mean age, indicat-
0.05 were considered to indicate marginal risks.
ing the control group was appropriate (Table 1).
The adverse effects following propofol injection
were grouped into three categories as previouslymentioned.8) Grade 1 adverse effects included eye
In the methylprednisolone group, 9 of 75 patients ex-
pain, shivering, face contortion and lacrimation,
perienced adverse effects, all of which were ob-
laughing, or apathy. Grade 2 adverse effects consist-
served immediately after propofol injection. In all of
ed of confusion, involuntary movement, or head and
these patients, symptoms disappeared within 5minutes of injection, and were mild enough to allowcontinuation of the Wada test as usual. In the control
group, 19 of 58 patients had adverse effects. The in-
cidence in the methylprednisolone group was sig-
nificantly lower, with an odds ratio of 0.280 (95% CI:
0.115–0.679, p = 0.0036), yielding a 72% risk reduc-
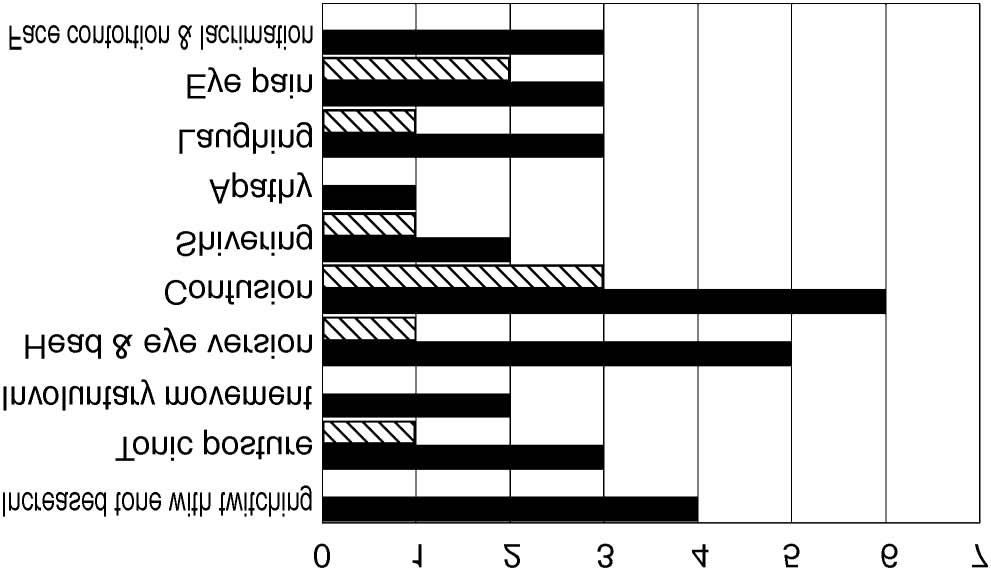
Analysis of the incidence of individual signs and
symptoms found that the methylprednisolone group
included 1 epilepsy patient with tonic posture (con-
trol group 3 patients) and no patients with increased
tone with twitching (control group 4 patients) (Fig.
1). These results indicated a significant reduction in
Grade 3 adverse effects in the methylprednisolone
group, with an odds ratio of 0.084 (95% CI:
0.010–0.712, p = 0.0052) and a 92% risk reduction
(Table 2). The methylprednisolone group included
no patients with involuntary movements and 1 with
head and eye version, demonstrating a marked
*Excludes one patient who stopped the examination and
reduction in Grade 2 adverse effects compared with
the control group, in which 2 patients showed in-
malformation, SD: standard deviation.
voluntary movements and 5 exhibited head and eye
Adverse effects of intracarotid propofol injection
into the brachial artery has been reported, suggest-ing particulate embolization or chemical incom-patibility with the blood could be the cause of thedecrease in vascular supply following propofol ar-terial injection.1) The significant decrease in Grade 3adverse effects seen in methylprednisolone-treatedpatients could have involved methylprednisolone ef-fects such as improvement of vascular supply andanti-allergic action, which reduced ischemia-in-duced
trophysiological or imaging studies during in-tracarotid propofol injection are needed to elucidatethe mechanism of reduction of these severe adverse
Comparison of the number of patients with in-
dividual adverse effects between the groups with (shadedcolumns) and without (closed columns) methylpredniso-
Methohexital2) and etomidate6) have been reported
lone injection prior to propofol administration.
as equivalent to amobarbital in terms of the efficacyin the Wada test. However, methohexital was soshort-acting that two successive injections wereneeded for each hemisphere, and no detailed
version (Fig. 1). The number of patients experienc-
description of adverse effects was provided. In-
ing confusion in the methylprednisolone group was
half that in the control group (3 patients versus 6).
shivering-like tremors in approximately half of the
Statistical analysis found no significant difference
patients, and either evidence of contralateral elec-
in the effect of methylprednisolone on the incidence
troencephalography slowing following most injec-
of Grade 1 or Grade 2 adverse effects (odds ratio:
tions, or an increase in interictal spike activity in the
0.394, 95% CI: 0.105–1.483, p = 0.1570) (Table 2).
hemisphere ipsilateral to injection.6) Moreover,etomidate infusion may be a major risk factor for the
development of relative adrenocortical insufficiencyin critically ill patients.7) Future reports of adverse
Our previous study showed that intracarotid
effects in a large number of patients undergoing
propofol injection is associated with a moderately
neurosurgery will provide useful information.
high risk of side effects. The present study found
The only adverse effects observed in two or more
that intravenous administration of methylpredniso-
patients in the methylprednisolone group were con-
lone followed by intracarotid propofol injection sig-
fusion (3 patients) and eye pain (2 patients), but the
nificantly reduced the incidence of severe (Grade 3)
incidences were approximately half those in the con-
trol group. Confusion is a condition arising from
Grade 3 adverse effects, which are comparatively
suppression of frontal lobe function and is indepen-
rare after amobarbital administration, may result in
dent of the type of anesthesia used. Confusion was
incompletion or inaccuracy of the Wada test.8) These
observed with at least one other adverse effect in 5 of
adverse effects may be caused by propofol-induced
7 control patients that experienced Grade 3 adverse
cerebral hyperexcitation.4) A recent systemic review
effects; no patients in this group experienced only
confusion. On the other hand, confusion was ob-
served as the only adverse effect in 3 methylpred-
phenomena were correlated with sudden increases
nisolone-treated patients. These results suggest that
in the cerebral concentrations of propofol, not sei-
infusion of methylprednisolone suppressed the oc-
zure history.12) In our previous study, no electroen-
currence of serious adverse effects. Further studies
cephalographic seizures or increasing epileptiform
are needed to clarify the mechanism reducing these
discharges were recorded before, during, and after
moderate adverse events with methylprednisolone.
the onset of clinical symptoms.8) Propofol induces
Methylprednisolone did not reduce the incidence of
contractions at low concentrations and relaxation at
eye pain, a Grade 1 adverse effect, presumably be-
high concentrations in the perfused cerebral artery
cause it does not influence the direct effect of
of the dog,9) but no in vivo action on cerebral perfu-
sion after intraarterial injection has been described.
In our previous study, the risk factors for Grade 3
Transient decrease in arterial blood flow immedi-
adverse effects (increased tone with twitching, tonic
ately after inadvertent injection of 10 ml propofol
posture) included age of 55 years or greater, AVM,
Intravenous Methylprednisolone During Wada Testing
High-grade adverse effects of intracarotid propofol injection among 113 patients
*Excludes 4 patients with Grade 1 and 4 patients with Grade 2 adverse effects. AVM: arteriovenous malformation, CIs:confidence intervals.
and total propofol injection dose greater than 20 mg.
artery. Anaesth Intensive Care 22: 291–292, 1994
In our current study, 113 subjects were selected by
Buchtel H, Passaro E, Selwa L, Deveikis J, Gomez-
eliminating 10 patients with Grade 1 adverse effects
Hassan D: Sodium methohexital (Brevital) as an
and 10 with Grade 2 adverse effects. Analysis con-
anesthetic in the Wada test. Epilepsia 43: 1056–1061,
ducted on these 113 patients confirmed that risk fac-
tors for Grade 3 adverse effects were age of 55 years
Chyatte D, Fode NC, Nichols DA, Sundt TM Jr: Preli-minary report: effects of high dose methylpredniso-
or greater, AVM, and total propofol injection dose
lone on delayed cerebral ischemia in patients at high
greater than 20 mg (Table 3). Other factors (sex,
risk for vasospasm after aneurysmal subarachnoid
history of epilepsy, lesion laterality, and speech
hemorrhage. Neurosurgery 21: 157–160, 1987
dominance) did not reach statistical significance. To
Collier C, Kelly K: Propofol and convulsions: the evi-
further clarify the effects of the methylprednisolone,
dence mounts. Anaesth Intensive Care 19: 573–575,
subgroup analysis was performed on 67 patients
selected by excluding 4 patients with Grade 1 ad-
Grote CL, Meador K: Has amobarbital expired? Con-
verse effects and 4 with Grade 2 adverse effects from
sidering the future of the Wada. Neurology 65:
the methylprednisolone group. The results showed
that none of the 3 factors mentioned above sig-
Jones-Gotman M, Sziklas V, Djordjevic J, Dubeau F,Gotman J, Angle M, Tampieri D, Olivier A, Ander-
nificantly affected the risk of Grade 3 adverse effects
mann F: Etomidate speech and memory test (eSAM):
a new drug and improved intracarotid procedure.
This study suggests that Wada testing using in-
travenous methylprednisolone administration prior
Malerba G, Romano-Girard F, Cravoisy A, Dousset B,
to propofol injection is a safe approach to the
Nace L, L áevy B, Bollaert PE: Risk factors of relative
preoperative evaluation of brain tumors, epilepsy,
adrenocortical deficiency in ICU patients needing
and AVMs. Further studies in a large number of
mechanical ventilation. Intensive Care Med 31:
patients are needed to compare the adverse effects
associated with intracarotid methohexital and
etomidate injection during Wada testing.
Hayashi N, Nishida N, Taki J, Enatsu R, Ikeda A,Miyamoto S, Hashimoto H: Evaluation of adverse ef-
fects in intracarotid propofol injection for Wada test. Neurology 65: 1813–1816, 2005
Nakamura K, Hatano Y, Hirakata H, Nishiwada M,
Supported by Grants-in-Aid for Scientific Research
Toda H, Mori K: Direct vasoconstrictor and vasodila-
2059713 from the Japan Society for the Promotion of
tor effects of propofol in isolated dog arteries. Br J
Takayama M, Miyamoto S, Ikeda A, Mikuni N, Taka-
hashi JB, Usui K, Satow T, Yamamoto J, MatsuhashiM, Matsumoto R, Nagamine T, Shibasaki H,
Brimacombe J, Gandini D, Bashford L: Transient
Hashimoto N: Intracarotid propofol test for speech
decrease in arm blood flow following accidental in-
and memory dominance in man. Neurology 63:
tra-arterial injection of propofol into the left brachial
Wada J, Rasmussen T: Intracarotid injection of sodi-
The current study is a retrospective comparison of
um amytal for the lateralization of cerebral speech
75 patients who underwent a Wada test from 2006 to
dominance: experimental and clinical observations. J
2008 using intracarotid propofol with intravenous
methylprednisolone and 58 patients who underwent
Walder B, Tramer MR, Seeck M: Seizure-like
the Wada test from 2001 to 2005 using intracarotid
phenomena and propofol: a systematic review. Neu-
propofol without methylprednisolone. The compari-
son was performed to determine if the use of in-travenous methylprednisolone decreased the inci-dence of adverse effects associated with the arterial
Address reprint requests to: Nobuhiro Mikuni, M.D.,
injection of propofol. The analysis demonstrated that
Ph.D., Department of Neurosurgery, Kyoto Univer-
the methylprednisolone group had fewer adverse ef-
sity Graduate School of Medicine, 54 Kawahara–cho,
fects, including a significantly lower incidence of
Shogoin, Sakyo–ku, Kyoto 606–8507, Japan.
Although the study is retrospective, the two groups
were well matched with regard to demographics, un-
derlying disease and propofol dosage. This study sug-gests the use of intravenous methylprednisolone may
Mikuni and his colleagues previously reported ad-
reduce the incidence of adverse effects associated with
verse effects associated with the intracarotid injection
the use of intracarotid injections of propofol for Wada
of propofol for Wada testing. These adverse effects
testing. What this retrospective, non-randomized
were divided into three grades: Grade 1 includes eye
study does not address is any change in the manufac-
pain, shivering, face contortion and lacrimation,
turing of propofol over the time period of the study
laughing or apathy. Grade 2 includes confusion, in-
that may account for the reduced incidence of side ef-
voluntary movement, or head and eye version. Grade
3 includes increased muscle tone with twitching and
rhythmic movements or tonic posture. Grade 3 ad-
verse effects are the most clinically relevant since they
may result in incompletion or inaccuracy of the Wada
ICMS • IPI • ISS Destaques • Matéria que dispõe sobre a concessão de bene-fícios nas operações com algodão em caroço e • Operações com Algodão em Caroço – Considerações• Anulação do Crédito mediante Estorno na Escrita Fiscal – • Trabalho com esclarecimentos sobre as hipóte-ses em que o contribuinte será obrigado a efetuar o estorno do c
The Skil s Development Service Ltd Master Practitioner Diploma in Cognitive Behavioural Therapy (Approved by The British Psychological Society LC) Evidenced Reading Module Topic: Interpreting Research in CBT Reading List* Agras, W. S., Walsh, B. T., Fairburn, C. G., Wilson, G. T., & Kraemer, H. C. (2000). A Multicenter Comparison of Cognitive-Behavioral Therapy and
 into the brachial artery has been reported, suggest-ing particulate embolization or chemical incom-patibility with the blood could be the cause of thedecrease in vascular supply following propofol ar-terial injection.1) The significant decrease in Grade 3adverse effects seen in methylprednisolone-treatedpatients could have involved methylprednisolone ef-fects such as improvement of vascular supply andanti-allergic action, which reduced ischemia-in-duced
trophysiological or imaging studies during in-tracarotid propofol injection are needed to elucidatethe mechanism of reduction of these severe adverse
Comparison of the number of patients with in-
dividual adverse effects between the groups with (shadedcolumns) and without (closed columns) methylpredniso-
Methohexital2) and etomidate6) have been reported
lone injection prior to propofol administration.
into the brachial artery has been reported, suggest-ing particulate embolization or chemical incom-patibility with the blood could be the cause of thedecrease in vascular supply following propofol ar-terial injection.1) The significant decrease in Grade 3adverse effects seen in methylprednisolone-treatedpatients could have involved methylprednisolone ef-fects such as improvement of vascular supply andanti-allergic action, which reduced ischemia-in-duced
trophysiological or imaging studies during in-tracarotid propofol injection are needed to elucidatethe mechanism of reduction of these severe adverse
Comparison of the number of patients with in-
dividual adverse effects between the groups with (shadedcolumns) and without (closed columns) methylpredniso-
Methohexital2) and etomidate6) have been reported
lone injection prior to propofol administration.