Annals of Oncology 24 (Supplement 2): ii24–ii29, 2013
Intermediate hepatocellular carcinoma: currenttreatments and future perspectives
J.-F. Dufour1,2*, I. Bargellini3, N. De Maria4, P. De Simone4, I. Goulis5 & R. T. Marinho61Hepatology, Department of Clinical Research, University of Berne, Berne; 2University Clinic for Visceral Surgery and Medicine, Inselspital, University of Berne, Berne,Switzerland; 3Department of Diagnostic and Interventional Radiology, University of Pisa, Pisa; 4Gastroenterology, Department of Internal Medicine, University Hospital of
Modena, Modena, Italy; 54th Department of Internal Medicine, Aristotelian University of Thessaloniki, Greece; 6Liver Unit, Department of Gastroenterology and
Hepatology, Hospital de Santa Maria, Medical School of Lisbon, Lisboa, Portugal
Current guidelines recommend transarterial chemoembolization (TACE) as the standard treatment of Barcelona-Clinic
Liver Cancer (BCLC)-B patients. However, the long-term survival outcomes of patients managed with this technique do
not appear fully satisfactory; in addition, intermediate-stage hepatocellular carcinoma (HCC) includes a heterogeneous
population of patients with varying tumour burdens, liver function and disease aetiology. Therefore, not all patients with
intermediate-stage HCC may derive similar benefit from TACE, and some patients may benefit from other treatmentoptions, which are currently approved or being explored. These include different TACE modalities, such as selective
TACE or drug-eluting beads TACE and radioembolization. The introduction of sorafenib in the therapeutic
armamentarium for HCC has provided a new therapeutic option for the treatment of BCLC-B patients who are
unsuitable to TACE or in whom TACE resulted in unacceptable toxicity. In addition, clinical trials aimed at investigating
the potential role of this molecule in the treatment of patients with intermediate-stage HCC within combination
therapeutic regimens are ongoing. This narrative review will present and discuss the most recent evidence on the
locoregional or medical treatment with sorafenib in patients with intermediate-stage HCC.
Key words: adverse events, chemoembolization, locoregional, SIRT, sorafenib, systemic targeted therapy, TACE
with still well-preserved liver function (Child-Pugh A5 due toalbumin 4.8 g/dl, total bilirubin 0.9 mg/dl, INR 0.99) and only
The recent guidelines issued by the European Association for
two nodules <3 cm and a patient with persistent ascites and
the Study of Liver (EASL) endorse the Barcelona-Clinic Liver
jaundice (Child-Pugh B) with multifocal large tumours will be
Cancer (BCLC) classification for the staging of hepatocellular
classified as affected by intermediate-stage HCC.
carcinoma (HCC) []. This classification divides HCC
Therefore, not all patients with intermediate-stage HCC will
patients into five stages (0, A, B, C and D) according to
derive similar benefit from TACE, and some patients may
different prognostic variables and allocates therapies according
benefit from other treatment options, which are currently
approved or being explored (Figure ) These include
About 20% of HCC patients are classified as affected by
different TACE modalities, such as selective TACE or drug-
BCLC-B, or intermediate-stage HCC, and present a 2-year
eluting beads (DB)-TACE, and radioembolization or
survival of ∼50% []. The management of these patients, like
combination approaches [–For instance, the combination
that of other HCC subjects, should be based on themultidisciplinary interaction among different specialists ].
of TACE and radiofrequency ablation gave promising results in
Current guidelines recommend transarterial
chemoembolization (TACE) as the standard treatment of
The introduction of sorafenib in the therapeutic
BCLC-B patients ]. However, despite several recent
armamentarium for HCC has provided a new therapeutic
advances and technical refinements, the long-term survival
option for the treatment of BCLC-B patients who are
outcomes of patients managed with this technique do not
unsuitable to TACE or in whom TACE resulted in
appear fully satisfactory [in addition, intermediate-stage
unacceptable toxicity. In addition, clinical trials aimed at
HCC includes a heterogeneous population of patients with
investigating the potential role of this molecule in the
varying tumour burdens, liver function and disease aetiology
treatment of patients with intermediate-stage HCC within
[]. As reported by Piscaglia and Bolondi both a patient
combination therapeutic regimens are ongoing.
This review will present and discuss the most recent
evidence on the locoregional or medical treatment withsorafenib in patients with intermediate-stage HCC. Surgical
*Correspondence to: Prof. Jean-Francois Dufour, Hepatology, Department of Clinical
procedures, including resection or transplantation, can be
Research, University of Berne, Murtenstrasse 35, 3010 Bern, Switzerland; Tel: +41-31-632-31-91; Fax: +41-31-632-49-97; E-mail: [email protected]
considered in selected patients, as reviewed in Zhang et al.
The Author 2013. Published by Oxford University Press on behalf of the European Society for Medical Oncology. All rights reserved. For permissions, please email: [email protected].
the imaging modalities for locoregional treatments is beyondthe scopes of this review.
TACE is considered as the standard treatment of patients withcompensated liver function (Child B up to 8 points), with largesingle nodule or multifocal HCC (<5 cm) not occluding theportal venous vessels and without extrahepatic spreadSurvival benefits determined by TACE were reportedin two randomized, controlled trials (RCTs): Llovet et al. [
Figure 1. Locoregional (LR) or medical treatment of patients with
showed a significant survival advantage in favour of TACE over
intermediate-stage HCC, either approved or under investigation. Asterisk
transarterial embolization [hazard ratio (HR) for death: 0.47;
95% confidence interval (CI), 0.25–0.91; P = 0.025], and Lo
et al. [showed a 50% reduction in the relative risk of deathwith TACE versus symptomatic treatment (95% CI, 0.31–0.81;
Resection may be a valid option in selected patients ]. More
P = 0.005). In addition, the efficacy of TACE has been
in detail, radical resection can be considered in: (i) patients
evaluated in other RCTs, and two of these did not show a
with single HCC and large tumour nodule, swelling outward,
prolonged survival time with respect to controls
clear border or pseudocapsule and <30% hepatic tissue
Despite this, the results of a meta-analysis published in 2003
destroyed or >50% compensatory hepatic hypertrophy and (ii)
indicated that treatment with transarterial embolization/TACE
patients with multiple HCC with ≤3 nodules localized in one
is associated with a significantly higher 2-year survival rate
lobe or segment of the liver []. Other patients may be eligible
than in the control group (odds ratio, 0.53; 95% CI, 0.32–0.89;
for palliative resection (see Zhang et al. ] for a deeper
P = 0.017) []. These findings are in agreement with those
discussion on indication for palliative resection). Due to the
reported in another meta-analysis of 18 RCTs, which shows
shortage of available organs, it is currently recommended that
that TACE improves the overall survival (OS) at 2 years
only those HCC patients with an estimated high probability of
compared with non-active treatment; however, the magnitude
post-transplant survival benefit may be selected for liver
of this benefit is relatively small [].
transplantation. The Milan criteria (1 lesion ≤5 cm or 2–3
TACE-associated adverse events (AEs), although usually
lesions ≤3 cm), proposed in 1996, still represent the basis for
transient and manageable, occur in a significant proportion
the selection of the best candidates for liver transplant [–
(35–100%) of patients: they include post-embolization
]. However, the adoption of expanded and/or down-staging
syndrome (comprising fever, abdominal pain and a moderate
criteria for liver transplant has been proposed and is currently
degree of ileus), relevant liver function deterioration, ascites
under clinical investigation ]. For instance, a study by
and gastrointestinal bleeding In addition, TACE does
Mazzaferro—the leading investigator of the team who
have some contra-indications, both absolute and relative
identified the same Milan criteria —conducted on 1556
patients has suggested that more HCC patients could be
Collectively, these findings indicated that treatment with
eligible for transplantation if the Milan criteria were replaced
TACE may be associated with some benefits in terms of OS,
by a more precise estimation of survival based on individual
although the level of benefit varies and considerable AEs may
tumour characteristics and up-to-seven criteria ].
occur: therefore, a careful selection of patients appears crucial
These findings are confirmed by a study on more than 6000
before the initiation of TACE therapy ].
patients included in the US Scientific Registry of Transplant
In the future, additional trials should be conducted to
Recipients database: this analysis shows that the Milan criteria
investigate some ‘grey areas’ still present in the current
are too restrictive, and patients with larger total tumour
knowledge of TACE, such as the use and type of the
volume can enjoy satisfactory post-transplant survivals [].
chemotherapeutic agent, as well as the best type of embolizing
Moreover, a composite patient selection score combining total
medium Of note, recent evidence supports the use of the
tumour volume and alpha fetoprotein can be considered the
EASL criteria or the mRECIST criteria, rather than the
most effective of all tested staging criteria for the prediction of
standard RECIST criteria, in the evaluation of clinical response
the survival of transplanted patients [].
after TACE ]. Gilmore et al. reported a significantassociation between survival and overall EASL and mRECIST
responses: response was associated with a 44% risk reduction
and mRECIST with a 42% reduction. Conversely, there was nosignificant association between survival and RECIST 1.1
The most widely used locoregional therapies for the treatment
responses These data are corroborated by those reported
of intermediate-stage HCC are TACE, selective TACE, DB-
by Shim et al. who show that the HRs for time to
progression (TTP) and OS in responders were 0.15 (95% CI:
interventions are image-guided and therefore a careful
0.10–0.21) and 0.18 (95% CI: 0.13–0.26), respectively, when the
imaging, also before and after treatment, represents an essential
mRECIST definition of an objective response was used and
prerequisite for their success A detailed description of
0.16 (95% CI: 0.11–0.22) and 0.23 (95% CI: 0.16–0.33),
Table 1. Absolute and relative contraindications for TACE (reproducedfrom Raoul et al. with permission)
• Decompensated cirrhosis (Child-Pugh B ≥8) including:
– Jaundice– Clinical encephalopathy– Refractory ascites– Hepatorenal syndrome
• Extensive tumour with massive replacement of both entire lobes
• Severely reduced portal vein flow (e.g. non-tumoural portal vein
• Technical contraindications to hepatic intra-arterial treatment,
• Renal insufficiency (creatinine ≥2 mg/dl or creatinine clearance
Figure 2. Complete response, objective response and disease control rate
[cumulative number (%) of patients] at 6 months in the PRECISION V
trial (reproduced from Lammer et al. [], with permission).
• Co-morbidities involving compromised organ function:
The randomized, controlled PRECISION V trial has
compared DB-TACE with the standard TACE for the treatment
of 212 cirrhotic patients with HCC ]. At 6 months, the DB-
• Untreated varices at high risk of bleeding
TACE group showed higher rates of complete response,
• Bile-duct occlusion or incompetent papilla due to stent or surgery
objective response and disease control compared with thecTACE group (Figure ) []. Although the predefinedhypothesis of superiority was not met in the overall population,
respectively, with the EASL response criteria. In a recent paper,
patients with Child-Pugh B, Eastern Cooperative Oncology
Kim et al. reached the same conclusions, further supporting
Group 1, bilobar disease and recurrent disease presented a
the significant association between TACE response and OS
significant increase in objective response (P = 0.038). In
addition, DB-TACE was associated with a reduction in serious
Selectivity in positioning the catheter may enhance the
liver toxicity and a lower rate of doxorubicin-related side-effects
efficacy of TACE. Selective TACE indeed comprises the
when compared with the standard TACE.
injection of chemotherapeutic agents into the segmental or
These findings are overall in line with those reported in
subsegmental branches feeding the tumours [Golfieri et al.
another RCT by Malagari et al. ], which compared DB-
[] compared the effectiveness of selective/superselective
TACE with doxorubicin (n = 41) and bland embolization
TACE versus standard TACE in determining tumour necrosis,
(n = 43). At 6 months, a complete response, assessed with the
in a prospective database of 67 consecutive patients (122
EASL criteria, was seen in 11 patients (26.8%) in the DB-TACE
nodules, all <5 cm). The mean histological necrosis level was
group versus 6 patients (14%) in the bland embolization group,
64.7%; complete tumour necrosis was obtained in 42.6% of the
whereas a partial response was achieved in 19 patients (46.3%)
nodules. When compared with the standard TACE, selective/
and 18 (41.9%) patients, respectively. An advantage for DB-
superselective TACE was associated with higher mean levels of
TACE has been also reported in terms of rate of recurrences
necrosis (75.1 versus 52.8%; P = 0.002) and a higher rate of
and TTP (42.4 ± 9.5 versus 36.2 ± 9.0 weeks; P = 0.008).
complete necrosis (53.8 versus 29.8%, P = 0.013). A direct
The overall favourable efficacy of DB-TACE is further
relationship was reported between the tumour diameter and
corroborated by a recent international, long-term (5 years of
the mean tumour necrosis level (59.6% for lesions <2 cm,
follow-up) study In total, 173 HCC patients not suitable
68.4% for lesions 2.1–3 cm and 76.2% for lesions >3 cm).
for curative treatments were enrolled; 41% were classified as
These findings suggest that selective/superselective TACE may
Child-Pugh B. The OS at 5 years was 22.5%, with higher rates
determine a higher rate of tumour necrosis than the standard
achieved in Child-Pugh class A compared with Child-Pugh
TACE; however, very small nodules (<2 cm) may not respond
class B patients (29.4 versus 12.8%). The mean OS was 43.8
months. Multivariate analysis identified some significant andindependent determinants of 5-year survival: these were thenumber of lesions, lesion vascularity, initially achieved
complete response and objective response.
DB-TACE uses doxorubicin-loaded beads rather than the
In a recent observational study by Burrel et al. [] (n = 104;
conventional doxorubicin Lipiodol® (Guerbet, Genoa, Italy)
63 patients were BCLC-B), DB-TACE was associated with the
emulsion It has been suggested that this approach could
median survival of 48.6 months, and only 10 patients reported
result in an overall favourable toxicity profile and antitumor
major complications associated with this intervention. This
activity (response rates ranging from 13.3 to 80.7%)
study confirmed the safety of DB-TACE in patients with HCC
and defined the survival gain that can be obtained, providing
key evidence to decide among controversial indications and
TACE [However, these data might not be directly extendedto clinical practice, since they were collected in a single, highly
Sorafenib is currently the only drug approved for the treatment
specialized centre. In addition, included patients had to meet
of patients with advanced HCC (BCLC-C stage); however, the
very stringent selection criteria ( preserved liver function,
use of this molecule in the treatment of intermediate patients is
absence of symptoms, extrahepatic spread or vascular
approved in patients with BCLC-B HCC who are unsuitable to
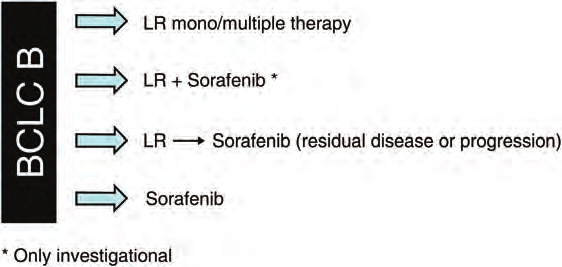
TACE or in whom TACE resulted in unacceptable toxicityAccording to available evidence, sorafenib has arole in patients who fail or are not eligible to TACE, as recently
suggested by a Panel of Experts []. We propose here a
Radioembolization is an investigational technique which
slightly modified version of the same algorithm (Figure ).
has given some promising results in preliminary experiences
Bruix et al. [] carried out a subanalysis of the landmark
]. It is defined as the infusion of radioactive substances
SHARP study to compare the efficacy and safety of sorafenib
(such as Iodine-131-labelled lipiodol or microspheres
alone in patients with BCLC-B (sorafenib, n = 54; placebo,
containing Yttrium-90) into the hepatic artery ]. Given the
n = 51) versus BCLC-C (sorafenib, n = 245; placebo, n = 252)
hypervascularity of HCC, microspheres will be preferentially
stage of HCC. Overall, the benefit determined by sorafenib,
delivered to the tumour area and selectively emit high-energy,
expressed in terms of OS and TTP, was similar in BCLC-B
low-penetration radiation to the tumour Salem et al. ]
(median OS: 14.5 months, +39% versus placebo; median TTP:
have reported the results of a feasibility study which included
6.9 months, +113% versus placebo, P = 0.0016) and BCLC-C
291 patients with HCC, who received a total of 526 treatments
(median OS: 9.7 months, +43% versus placebo, P = 0.018;
with radioembolization. The response rate according to the
median TTP: 4.9 months, +69% versus placebo, P = 0.00003)
EASL criteria was 57%; the overall TTP was 7.9 months.
subgroups and was consistent with that reported in the overall
Survival times were longer in patients with Child-Pugh A (17.2
population The incidence of grade 3/4 drug-related AEs
months) than in those with Child-Pugh B disease (7.7 months;
was not different in the two subgroups and was similar to that
P = 0.002). Reported toxic effects included fatigue (57%), pain
reported for the overall SHARP study population. The authors
(23%) and nausea/vomiting (20%); 19% exhibited grade 3/4
concluded that these findings confirm a retained efficacy of
bilirubin toxicity. The 30-day mortality rate was 3%.
sorafenib even in the intermediate-stage HCC [].
However, the relevant costs associated with
In an observational setting, a subanalysis of the global phase
radioembolization may limit a wide use of this technique [].
IV GIDEON study documented an OS of 12.6 months for
Moreover, the recent EASL Guidelines stressed that, due to the
BCLC-B patients, as assessed in a cohort of 311 Child-Pugh A
lack of RCTs comparing radioembolization with
and B patients []. In the smaller Italian SOFIA study, the OS
chemoembolization or sorafenib in patients with intermediate-
of the 74 BCLC-B patients treated with sorafenib was longer
or advanced-stage HCC, further research is needed to establish
than that reported in the 222 BCLC-C patients evaluated (20.6
a competitive efficacy role in these populations [
versus 8.4 months; P < 0.0001) []. Taken together, these
Figure 3. Proposed algorithm for the treatment of patients with intermediate-stage HCC. Response is defined according to mRECIST criteria.
preliminary results lend some support to the potential use of
multidisciplinary perspective. Lastly, sorafenib, the only
sorafenib monotherapy in patients with BCLC-B stage of HCC.
systemic treatment currently approved for the treatment of
It is widely accepted that TACE promotes the synthesis of
HCC, has a role in the treatment of patients with BCLC-B
proangiogenic factors via a hypoxia-driven mechanism
stage of HCC who are unsuitable to TACE or in whom TACE
Therefore, there may be a rationale for the combination of
sorafenib with TACE, since sorafenib inhibits the action of
Another intriguing arena is represented by the combination
or the sequential use of locoregional approaches and sorafenib.
Preliminary evidence, collected in a phase I trial, shows that
Moreover, preliminary evidence suggests that sorafenib may be
the combination of sorafenib and TACE is not associated with
used in patients who fail or are not eligible to TACE, in a
major AEs and, therefore, could deserve further investigations
sequential manner. The potential combination of TACE (either
[]. Moreover, given the overall more favourable efficacy/
standard TACE or DB-TACE) and systemic targeted therapy
safety profile of DB-TACE compared with the standard TACE,
also represents a promising treatment strategy, currently being
the combination of sorafenib with DB-TACE appears
explored in different phase III trials.
promising. Clinical trials investigating this therapeuticapproach (namely the START, SOCRATES and TACTIS) are
ongoing and will likely provide new evidence on the efficacyand safety of a combination of TACE and sorafenib in the
Editorial assistance was provided by Luca Giacomelli, PhD, on
treatment of intermediate-stage HCC patients. The results of
behalf of inScience Communication, Springer Healthcare; this
the global phase II SPACE trial have been recently published in
assistance was funded by Bayer Italy.
an abstract form []. In total, 307 patients with BCLC-B stageof HCC were randomized to sorafenib (n = 154) or placebo(n = 153) in combination with TACE with doxorubicin-eluting
beads (DEBDOX). Even if this study met its primary end point
JFD participated in advisory boards for BMS, Bayer, Gilead,
from a statistical point of view (P = 0.072 for TTP), the actual
Novartis, Roche. IG participated in advisory boards for BMS,
improvement of the median TTP was not clinically relevant
Gilead, Novartis, Roche, MSD. Other authors declare no
(from 166 to 169 days). The results of other ongoing studies
conflict of interest directly relevant to this study.
1. European Association for the Study of the Liver, European Organisation for
Patients with intermediate-stage HCC represent a
Research and Treatment of Cancer. EASL-EORTC Clinical Practice Guidelines:
heterogeneous population, characterized by varying tumour
management of hepatocellular carcinoma. J Hepatol 2012; 56(4): 908–943.
burdens, liver function and disease aetiology. Therefore, a ‘one
2. Llovet JM, Brú C, Bruix J. Prognosis of hepatocellular carcinoma: the BCLC
size fits all’ approach may not be entirely feasible in these
staging classification. Semin Liver Dis 1999; 19: 329–338.
subjects. We believe, in line with current guidelines, that a
3. Lencioni R. Loco-regional treatment of hepatocellular carcinoma. Hepatology
multidisciplinary management by specialists with different
4. Lencioni R, Chen XP, Dagher L et al. Treatment of intermediate/advanced
expertise may represent the optimal approach for the diagnosis
hepatocellular carcinoma in the clinic: how can outcomes be improved?
and treatment of patients classified as affected from
Oncologist 2010; 15(Suppl 4): 42–52.
5. Piscaglia F, Bolondi L. The intermediate hepatocellular carcinoma stage: should
TACE represents the standard treatment approach in this
treatment be expanded? Dig Liver Dis 2010; 42(Suppl 3): S258–S263.
population. This therapy is associated with some OS benefits,
6. Kim JH, Won HJ, Shin YM et al. Medium-sized (3.1–5.0 cm) hepatocellular
although the level of benefit reported varies—according to
carcinoma: transarterial chemoembolization plus radiofrequency ablation versus
patient’s and tumour characteristics as well as the methodology
radiofrequency ablation alone. Ann Surg Oncol 2011; 18(6): 1624–1629.
used. In addition, TACE is not suitable for all patients and can
7. Zhang ZM, Guo JX, Zhang ZC et al. Therapeutic options for intermediate-advanced
be associated with the onset of some AEs, although transitory.
hepatocel ular carcinoma. World J Gastroenterol 2011; 17(13): 1685–1689.
Variants of TACE or other locoregional treatments have been
8. Mazzaferro V, Llovet JM, Miceli R et al. Metroticket Investigator Study Group.
Predicting survival after liver transplantation in patients with hepatocellular
tested, and DB-TACE in particular showed promising results,
carcinoma beyond the Milan criteria: a retrospective, exploratory analysis. Lancet
but further evidence is necessary to fully support these
approaches. In addition, a very recent paper has documented
9. Ravaioli M, Grazi GL, Piscaglia F et al. Liver transplantation for hepatocellular
the potential benefits of a ‘repeated-TACE’ approach [], and
carcinoma: results of down-staging in patients initially outside the Milan selection
research aimed at investigating the factors who can predict a
criteria. Am J Transplant 2008; 8(12): 2547–2557.
failure of response with this treatment is active
10. Yao FY, Kerlan RK, Jr, Hirose R et al. Excellent outcome following down-staging
In our opinion, the potential role of radioembolization, or a
of hepatocellular carcinoma prior to liver transplantation: an intention-to-treat
combination of locoregional approaches (see for instance, the
analysis. Hepatology 2008; 48(3): 819–827.
11. Toso C, Asthana S, Bigam DL et al. Reassessing selection criteria prior to liver
combination of activated liposomal encapsulation of
transplantation for hepatocellular carcinoma utilizing the Scientific Registry of
doxorubicin in combination with radiofrequency ablation,
Transplant Recipients database. Hepatology 2009; 49(3): 832–838.
currently being explored in the HEAT trial NCT00617981), for
12. Meza-Junco J, Montano-Loza AJ, Liu DM et al. Locoregional radiological
the intermediate patients definitely deserves further
treatment for hepatocellular carcinoma; which, when and how? Cancer Treat Rev
investigations and should be considered from a
13. Gervais DA, Kalva S, Thabet A. Percutaneous image-guided therapy of intra-
29. Malagari K, Pomoni M, Moschouris H et al. Chemoembolization with doxorubicin-
abdominal malignancy: imaging evaluation of treatment response. Abdom
eluting beads for unresectable hepatocellular carcinoma: five-year survival
analysis. Cardiovasc Intervent Radiol 2012; 35(5): 1119–1128.
14. Davis CR. Interventional radiological treatment of hepatocellular carcinoma.
30. Burrel M, Reig M, Forner A et al. Survival of patients with hepatocellular
Cancer Control 2010; 17(2): 87–99.
carcinoma treated by transarterial chemoembolization (TACE) using DCBeads.
15. O’Neil BH, Venook AP. Hepatocellular carcinoma: the role of the North American
Implications for clinical practice and trial design. J Hepatol 2012; 56(6):
GI Steering Committee Hepatobiliary Task Force and the advent of effective drug
therapy. Oncologist 2007; 12: 1425–1432.
31. Salem R, Lewandowski RJ, Mulcahy MF et al. Radioembolization for
16. Llovet JM, Real MI, Montaña X et al. Arterial embolisation or chemoembolisation
hepatocellular carcinoma using Yttrium-90 microspheres: a comprehensive report
versus symptomatic treatment in patients with unresectable hepatocellular
of long-term outcomes. Gastroenterology 2010; 138: 52–64.
carcinoma: a randomised controlled trial. Lancet 2002; 359: 1734–1739.
32. Ibrahim SM, Lewandowski RJ, Sato KT et al. Radioembolization for the treatment
17. Lo CM, Ngan H, Tso WK et al. Randomized controlled trial of transarterial lipiodol
of unresectable hepatocellular carcinoma: a clinical review. World J Gastroenterol
chemoembolization for unresectable hepatocellular carcinoma. Hepatology 2002;
33. Woodall CE, Scoggins CR, Ellis SF et al. Is selective internal radioembolization
18. Dof oël M, Bonnetain F, Bouché O et al. Multicentre randomised phase III trial
safe and effective for patients with inoperable hepatocellular carcinoma and
comparing tamoxifen alone or with transarterial lipiodol chemoembolization for
venous thrombosis? J Am Coll Surg 2009; 208: 375–382.
unresectable hepatocellular carcinoma in cirrhotic patients (Fédération Francophone
34. Park JW, Koh YH, Kim HB et al. Phase II study of concurrent transarterial
de Cancérologie Digestive 9402). Eur J Cancer 2008; 44: 528–538.
chemoembolization and sorafenib in patients with unresectable hepatocellular
19. Groupe d’Etude et de Traitement du Carcinome Hépatocellulaire. A comparison of
carcinoma. J Hepatol 2012; 56(6): 1336–1342.
lipiodol chemoembolization and conservative treatment for unresectable
35. Dufour JF. TACE with or without systemic therapy? J Hepatol 2012; 56(6):
hepatocellular carcinoma. N Engl J Med 1995; 332: 1256–1261.
20. Llovet JM, Bruix J. Barcelona Clinic Liver Cancer Group. Systematic review of
36. Farinati F, Giacomin A, Vanin V et al. TACE treatment in hepatocellular carcinoma:
randomized trials for unresectable hepatocellular carcinoma: chemoembolization
what should we do now? J Hepatol 2012; 57(1): 221–222.
improves survival. Hepatology 2003; 37: 429–442.
37. Bruix J, Raoul JL, Sherman M et al. Efficacy and safety of sorafenib in patients
21. Cammà C, Schepis F, Orlando A et al. Transarterial chemoembolization for
with hepatocellular carcinoma (HCC): subanalysis of sharp trial based on
unresectable hepatocellular carcinoma: meta-analysis of randomized controlled
Barcelona Clinic Liver Cancer (BCLC) stage. J Hepatol 2009; 50: S28–S29.
trials. Radiology 2002; 224(1): 47–54.
38. Lencioni R. Second interim results of the GIDEON (Global Investigation of
22. Raoul JL, Sangro B, Forner A et al. Evolving strategies for the management of
Therapeutic DEcisions in HCC and of its treatment with sorafenib) study:
intermediate-stage hepatocellular carcinoma: available evidence and expert
Barcelona Clinic Liver Cancer (BCLC) Stage Subgroup Analysis (abstract #6500).
opinion on the use of transarterial chemoembolization. Cancer Treat Rev 2011;
In: ESMO-ECCO oncology meeting Stockholm; 2011.
39. Iavarone M, Cabibbo G, Piscaglia F et al.; SOFIA (SOraFenib Italian Assessment)
23. Gillmore R, Stuart S, Kirkwood A et al. EASL and mRECIST responses are
study group. Field-practice study of sorafenib therapy for hepatocellular
independent prognostic factors for survival in hepatocellular cancer
carcinoma: a prospective multicenter study in Italy. Hepatology 2011; 54(6):
patients treated with transarterial embolization. J Hepatol 2011; 55(6):
40. Dufour JF, Johnson P. Liver cancer: from molecular pathogenesis to new
24. Shim JH, Lee HC, Kim SO et al. Which response criteria best help predict
therapies: summary of the EASL single topic conference. J Hepatol 2010; 52:
survival of patients with hepatocellular carcinoma following chemoembolization?
A validation study of old and new models. Radiology 2012; 262(2): 708–718.
41. Lencioni R. Chemoembolization for hepatocellular carcinoma. Semin Oncol 2012;
25. Kim BK, Kim KA, Park JY et al. Prospective comparison of prognostic values of
modified response evaluation criteria in solid tumours with European Association
42. Dufour JF, Hoppe H, Heim MH et al. Continuous administration of sorafenib in
for the Study of the Liver criteria in hepatocellular carcinoma following
combination with transarterial chemoembolization in patients with
chemoembolisation. Eur J Cancer 2013; 49(4): 826–834.
hepatocellular carcinoma: results of a phase I study. Oncologist 2010; 15(11):
26. Golfieri R, Cappelli A, Cucchetti A et al. Efficacy of selective transarterial
chemoembolization in inducing tumor necrosis in small (<5 cm) hepatocellular
43. Lencioni R, Llovet JM, Han G et al. Sorafenib or placebo in combination with
carcinomas. Hepatology 2011; 53(5): 1580–1589.
transarterial chemoembolization (TACE) with doxorubicin-eluting beads (DEBDOX)
27. Lammer J, Malagari K, Vogl T et al.; PRECISION V Investigators. Prospective
for intermediate-stage hepatocellular carcinoma (HCC): Phase II, randomized,
randomized study of doxorubicin-eluting-bead embolization in the treatment of
double-blind SPACE trial. J Clin Oncol 2012; 30(Suppl. 4): abstr LBA154.
hepatocellular carcinoma: results of the PRECISION V study. Cardiovasc Intervent
44. Terzi E, Golfieri R, Piscaglia F et al. Response rate and clinical outcome of HCC
after first and repeated cTACE performed ‘on demand’. J Hepatol 2012; 57(6):
28. Malagari K, Pomoni M, Kelekis A et al. Prospective randomized comparison of
chemoembolization with doxorubicin-eluting beads and bland embolization with
45. Georgiades C, Geschwind JF, Harrison N et al. Lack of response after initial
BeadBlock for hepatocellular carcinoma. Cardiovasc Intervent Radiol 2010; 33(3):
chemoembolization for hepatocellular carcinoma: does it predict failure of
subsequent treatment? Radiology 2012; 265(1): 115–123.
PARA ADQUIRIR O RESTANTE DO CONTEÚDO DOS MANUAIS FARMATÉCNICA.COM.BR EFETUAR A COMPRA ATRAVÉS DO SITE: GEL ARISTOFLEX Aristoflex AVC 4,5% Nipagim 0,15% Nipazol 0,1% Propilenoglicol 5% Água qsp 100% Procedimento: 1. Dissolver o nipagim e o nipazol com qs de propilenoglicol e reservar. 2. Hidratar o polímero aristoflex na água sob agitação. 3. Verter o propilenoglicol com os
Rapid Trabecular Bone Loss After Cardiac Transplantation Using FK506 (Tacrolimus)-Based Immunosuppression H.U. Stempfle, C. Werner, S. Echtler, T. Assum, B. Meiser, C.E. Angermann, K. Theisen, and R. Ga¨rtnerTHE MACROLIDE lactone tacrolimus (FK506) is a P Ͻ .01). No fracture was documented. There were nonew immunosuppressive drug that has demonstratedsignificant differences in biochemi
 the imaging modalities for locoregional treatments is beyondthe scopes of this review.
the imaging modalities for locoregional treatments is beyondthe scopes of this review. Table 1. Absolute and relative contraindications for TACE (reproducedfrom Raoul et al. with permission)
• Decompensated cirrhosis (Child-Pugh B ≥8) including:
– Jaundice– Clinical encephalopathy– Refractory ascites– Hepatorenal syndrome
• Extensive tumour with massive replacement of both entire lobes
• Severely reduced portal vein flow (e.g. non-tumoural portal vein
• Technical contraindications to hepatic intra-arterial treatment,
• Renal insufficiency (creatinine ≥2 mg/dl or creatinine clearance
Figure 2. Complete response, objective response and disease control rate
[cumulative number (%) of patients] at 6 months in the PRECISION V
trial (reproduced from Lammer et al. [], with permission).
Table 1. Absolute and relative contraindications for TACE (reproducedfrom Raoul et al. with permission)
• Decompensated cirrhosis (Child-Pugh B ≥8) including:
– Jaundice– Clinical encephalopathy– Refractory ascites– Hepatorenal syndrome
• Extensive tumour with massive replacement of both entire lobes
• Severely reduced portal vein flow (e.g. non-tumoural portal vein
• Technical contraindications to hepatic intra-arterial treatment,
• Renal insufficiency (creatinine ≥2 mg/dl or creatinine clearance
Figure 2. Complete response, objective response and disease control rate
[cumulative number (%) of patients] at 6 months in the PRECISION V
trial (reproduced from Lammer et al. [], with permission). and defined the survival gain that can be obtained, providing
key evidence to decide among controversial indications and
TACE [However, these data might not be directly extendedto clinical practice, since they were collected in a single, highly
Sorafenib is currently the only drug approved for the treatment
specialized centre. In addition, included patients had to meet
of patients with advanced HCC (BCLC-C stage); however, the
very stringent selection criteria ( preserved liver function,
use of this molecule in the treatment of intermediate patients is
absence of symptoms, extrahepatic spread or vascular
approved in patients with BCLC-B HCC who are unsuitable to
TACE or in whom TACE resulted in unacceptable toxicityAccording to available evidence, sorafenib has arole in patients who fail or are not eligible to TACE, as recently
suggested by a Panel of Experts []. We propose here a
Radioembolization is an investigational technique which
slightly modified version of the same algorithm (Figure ).
and defined the survival gain that can be obtained, providing
key evidence to decide among controversial indications and
TACE [However, these data might not be directly extendedto clinical practice, since they were collected in a single, highly
Sorafenib is currently the only drug approved for the treatment
specialized centre. In addition, included patients had to meet
of patients with advanced HCC (BCLC-C stage); however, the
very stringent selection criteria ( preserved liver function,
use of this molecule in the treatment of intermediate patients is
absence of symptoms, extrahepatic spread or vascular
approved in patients with BCLC-B HCC who are unsuitable to
TACE or in whom TACE resulted in unacceptable toxicityAccording to available evidence, sorafenib has arole in patients who fail or are not eligible to TACE, as recently
suggested by a Panel of Experts []. We propose here a
Radioembolization is an investigational technique which
slightly modified version of the same algorithm (Figure ).