A 28-year-old man underwent surgical correction of
hyperopia. Preoperative assessment showed corrected distance visual acuity of 20/20 and 20/32 with a refrac-
Victoria de Rojas, MD, PhD; Félix González-López, MD;
tion of +6 -1.5 ϫ 10° and +6.25 -1.5 ϫ 165° in the right
and left eye, respectively. IOP was 19 mm Hg in both eyes. White-to-white distance as measured with Orbscan
(Bausch & Lomb, Rochester, NY) was 12.25 and 12 mm in the right and left eye, respectively, and mean keratometry
PURPOSE: To present the case of a 28-year-old man with ac-
was 41.25 diopters in both eyes. Automated perimetry
etazolamide-induced bilateral choroidal effusion after uneventful
was within normal limits in both eyes, and the endothe-
surgery of the second eye in delayed sequential bilateral insertion
lial cell count measured by noncontact specular micro-
of an implantable collamer lens for hyperopia.
scope SP2000P (Topcon, Oakland, CA) was 2,741 and 2,916 cells/mm2 in the right and left eye, respectively.
The anterior chamber depth measured by A-scan ultra-
RESULTS: Surgery of the left eye was uneventful, and the im-
sound was 3.86 mm in both eyes, and thickness was 640
plantable collamer lens was implanted 3 weeks later in the right
and 611 μm in the right and left eye, respectively; thus,
eye. Twenty-four hours after surgery, the patient presented with
anterior chamber depth from endothelium measured
bilateral shallow anterior chamber, vault 0, and myopic shift
3.25 and 3.24 mm in the right and left eye, respectively.
(-8 diopters) in both eyes. B-scan ultrasound showed choroidal
Fundus examination was normal in both eyes.
thickening in both eyes, which was consistent with choroidal ef-fusion syndrome. A causal relationship was suspected with oral
A decision was made to implant ICLs with intraop-
acetazolamide, which had been prescribed after surgery. When
erative paired opposite incisions in both eyes. Fifteen
the drug was stopped, the condition improved slowly and re-
days before surgery in the left eye, two laser peripheral
iridotomies were performed in both eyes. The ICL was implanted in the left eye without complications (VICH
CONCLUSIONS: Choroidal effusion should be included in the dif-
12.6 +6.5AQ1). The patient was prescribed 250 mg of
ferential diagnosis of shallow anterior chamber after implantation of an implantable collamer lens.
oral acetazolamide every 12 hours (two doses), topical moxifloxacin 0.5% every 8 hours, and tobramycin 0.3%
[J Refract Surg. 20XX;XX(X):XX-XX.]
together with dexamethasone 0.1% every 6 hours. On postoperative day 1, uncorrected distance visual acuity
in the left eye was 20/32, IOP was 19 mm Hg with a
ulfonamide drugs have been associated with deep and quiet anterior chamber and a vault of 370 μm. choroidal effusion, although this adverse event
Three weeks later, the ICL was implanted in the right
is infrequent.1 We present a case of acetazol-
eye without complications (VICH 13.2 +6AQ1). The
amide-induced bilateral choroidal effusion with nar-
same treatment was prescribed for the left eye.
row chamber after insertion of an implantable collamer
Twenty-four hours later, uncorrected visual acu-
lens (ICL). Although rare, both malignant glaucoma and
ity was less than 0.05 in both eyes (counting fingers)
pupillary block glaucoma are well-known complica-
and improved to 20/30 and 20/50 with refraction of
tions of the procedure, that also present with shallow
-8.25 -0.75 ϫ 10° and -8.25 -1.5 x 180° in the right and
chamber and high intraocular pressure (IOP) early after
left eye, respectively. Biomicroscopy showed a shal-
surgery. Thus, choroidal effusion should be included
low chamber with vault 0 in both eyes (Figure 1) and
in the differential diagnosis of high IOP and shallow
an IOP of 27 and 22 mm Hg in the right and left eye,
anterior chamber following implantation of an ICL.
respectively. The Seidel test results were negative. Iri-dotomies were patent, and gonioscopy revealed appo-
From Clínica Baviera, Instituto Oftalmológico Europeo, Spain
sitional angle closure in both eyes. Funduscopy was
(VR, FG-L, JB); and the Department of Ophthalmology, Complexo
not performed to avoid pupil dilation in this setting
Hospitalario Universitario, A Coruña, Spain (VR).
of appositional angle closure, and B-scan ultrasonogra-
Submitted: January 12, 2013; Accepted: April 18, 2013
phy showed flat choroidal thickening consistent with
The authors have no financial or proprietary interest in the materials
choroidal effusion syndrome in both eyes.
Because of the bilateral involvement, a drug etiol-
Correspondence: Victoria de Rojas, MD, PhD, Clínica Baviera, Plaza
ogy was considered and a causal relationship with oral
de Galicia, 2, A Coruña, Spain. E-mail: [email protected]
acetazolamide was suspected. The patient was treated with hourly topical prednisolone acetate 1%, topi-
Journal of Refractive Surgery UÊ6°ÊÝÝ]Ê °ÊÝ]ÊÓä£8
Bilateral Choroidal Effusión After ICL Implantation/de Rojas et al
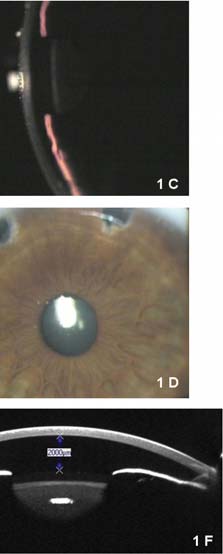
Figure 1. Slit-lamp photography of the (A and B) right eye and (C and D) left eye 1 day after surgery in the second eye (right) showing bilateral shallow anterior chamber with vault 0 and patent iridotomies in both eyes. Pentacam (Oculus Optikgeräte GmbH, Wetzlar, Germany) Scheimpflug imaging of the anterior segment revealed an anterior chamber depth of 1,820 and 2,000 μm in the (E) right and (F) left eye, respectively, on day 2 after surgery of the right eye. Vault was 0 in both eyes.
To our knowledge, we present the first report of cil-
iochoroidal effusion after implantation of an ICL. How-ever, this condition has previously been considered a theoretical component in the differential diagnosis of shallow anterior chamber early after implantation of an ICL, with the following alternatives2-4: pupillary block glaucoma, oversized ICL, incision leakage, cil-iochoroidal effusion, suprachoroidal hemorrhage, and malignant glaucoma. In our case, the finding of patent iridotomy and vault 0, which indicated forward dis-placement of the natural lens, ruled out pupillary block induced by occluded iridotomy or excessive vaulting.
Figure 2. Slit-lamp photography 5 days after surgery in the (A) second
The negative Seidel test result and the slightly high
eye (right) showing complete resolution, with a deep and quiet anterior
IOP enabled us to rule out wound leak. The condition
chamber and appropriate vaulting in the right and (B) left eyes. Pentacam
could only have been caused by malignant glaucoma,
(Oculus Optikgeräte GmbH, Wetzlar, Germany) Scheimpflug imaging of the anterior segment revealed vaulting of 400 and 360 μm in the (C) right
ciliochoroidal effusion, or suprachoroidal hemor-
and (D) left eye, respectively, and anterior chamber depth (endothelium
rhage. B-scan ultrasound revealed diffuse choroidal
to anterior surface of intraocular lens) of 2,400 μm 5 days after surgery
thickening consisting of a ciliochoroidal effusion,
which results in anterior rotation of the entire ciliary body and forward shifting of the lens–iris diaphragm,
cal timolol 0.5% every 12 hours, topical moxifloxa-
thereby obstructing trabecular outflow. The annular
cin 0.5% every 8 hours, and oral prednisone 50 mg
ciliochoroidal effusion decreases the diameter of the
every 24 hours. Five days later, the complication had
ciliary body and produces zonular laxity, thus leading
fully resolved (Figure 2). Uncorrected visual acuity to thickening of the crystalline lens and a further for- was 20/20 and 20/30 with vault of 400 and 360 μm in
ward shift of the lens. This series of events results in
the right and left eye, respectively. Anterior chamber
depth was 2,400 μm and IOP was 19 mm Hg in both
Because the presentation was bilateral after uni-
eyes. Topical medication and systemic corticosteroids
lateral surgery the previous day, surgery was ruled
were tapered and withdrawn within 1 week.
out as the cause of the choroidal effusion and a drug-
Bilateral Choroidal Effusión After ICL Implantation/de Rojas et al
associated etiology was suspected. Oral acetazolamide,
their case led to quicker resolution. Fortunately, in our
which was used to prevent IOP spikes associated with
case, IOP was slightly elevated in both eyes but angle-
the presence of a residual ophthalmologic viscoelastic
closure glaucoma did not develop despite the narrow
device behind the ICL, is known to cause ciliochoroi-
chamber. Because the suggested mechanism of angle
dal effusion, although this side effect is rare.1,5 Two
closure does not involve pupillary block, pilocarpine
cases of bilateral acute angle-closure glaucoma have
and peripheral laser iridotomy were not useful; in fact,
been reported after unilateral cataract surgery, and our patient had two patent iridotomies in each eye both were related to administration of oral acetazol-
amide after surgery.6,7 Topical dorzolamide has also been involved in several cases of choroidal effusion.8,9
The exact pathogenic mechanism of ciliary body
Study concept and design (VR, FG-L, JB); data collection (VR,
swelling induced by sulfonamide drugs is unknown.
FG-L, JB); analysis and interpretation of data (VR, FG-L, JB); drafting
Although an allergic reaction has been proposed of the manuscript (VR, FG-L, JB); critical revision of the manuscript by some authors, Krieg and Schipper5 found that re-
challenge with the same medication failed to produce an identical event and speculated that the drug-in-
duced increase in prostaglandin levels contributes to
1. Panday VA, Rhee DJ. Review of sulphonamide-induced acute
myopia and acute bilateral angle-closure glaucoma. Compr
ciliary body edema. This could explain the absence of
Ophthalmol Update. 2007;8:271-276.
the complication when our patient underwent surgery
2. Kohnen T, Kook D, Morral M, Güell JL. Part 2: Results and com-
in the first eye, after which he also received 250 mg of
plications. J Cataract Refract Surg. 2010;36:2168-2194.
3. Bylsma SS, Zalta AH, Foley E, Osher R. Phakic posterior cham-
Final total anterior chamber depth from endotheli-
ber intraocular lens pupillary block. J Cataract Refract Surg.
um to anterior lens surface, as measured by Pentacam
(Oculus Optikgeräte GmbH, Wetzlar, Germany) was 4. Khalifa Y, Goldsmith J, Moshirfar M. Bilateral explantation
of Visian Implantable Collamer Lenses secondary to bilateral
2,400 μm from endothelium to anterior ICL surface,
acute angle closure resulting from a non-pupillary block mech-
plus 400 and 360 μm of vault in the right and left eye,
anism. J Refract Surg. 2010;26:991-994.
respectively, plus 450 μm of ICL thickness (Figures 2C
5. Krieg PH, Schipper I. Drug-induced ciliary body edema: a new
and 2D), which yielded a total of 3.2 mm of anterior
theory. Eye (Lond). 1996;10:121-126.
chamber depth in both eyes after the resolution of the
6. Parthasarathi S, Myint K, Singh G, Mon S, Sadasivam P, Dhil-
complication. This measurement compares well with
lon B. Bilateral acetazolamide-induced choroidal effusion fol-lowing cataract surgery. Eye (Lond). 2007;21:870-872.
preoperative anterior chamber depth as measured by
7. Mancino R, Varesi Ch, Cerulli A, Aiello F, Nucci C. Acute bi-
lateral angle-closure glaucoma and choroidal effusion associ-
It is essential to highlight the importance of early
ated with acetazolamide administration after cataract surgery. J
recognition of this rare side effect and of immediate
Cataract Refract Surg. 2011;37:415-417.
withdrawal of acetazolamide, which, in the setting of
8. Doherty MD, Wride NK, Birch MK, Figueiredo FC. Choroidal
high IOP, could be continued erroneously if the sur-
detachment in association with topical dorzolamide: is hypoto-ny always the cause? Clin Exp Ophthalmol. 2009;37:750-752.
geon is not aware of this rare adverse reaction.6-9 The
9. Davani S, Delbosc B, Royer B, Kantelip JP. Choroidal detach-
role of systemic corticosteroids is controversial, be-
ment induced by dorzolamide 20 years after cataract surgery.
cause these agents have been shown to cause choroi-
Br J Ophthalmol. 2002;86:1457-1458.
dal effusion10 and were ineffective in one of the cases
AQ2 10. Chandler, Grant. In: Shields BM, ed. Textbook of Glau-
quoted above.6 However, Mancino et al.7 speculated
coma, 4th ed. Baltimore: Lippincott, Williams, & Wilkins; 1997:339-342.
that the use of intravenous methylprednisolone in
AUTHOR QUERIES AQ1 Please provide the manufacturer and location. AQ2 Please provide the full names of the editors and name of chapter.
Journal of Refractive Surgery UÊ6°ÊÝÝ]Ê °ÊÝ]ÊÓä£8



 Bilateral Choroidal Effusión After ICL Implantation/de Rojas et al
Figure 1. Slit-lamp photography of the (A and B) right eye and (C and D) left eye 1 day after surgery in the second eye (right) showing bilateral shallow anterior chamber with vault 0 and patent iridotomies in both eyes. Pentacam (Oculus Optikgeräte GmbH, Wetzlar, Germany) Scheimpflug imaging of the anterior segment revealed an anterior chamber depth of 1,820 and 2,000 μm in the (E) right and (F) left eye, respectively, on day 2 after surgery of the right eye. Vault was 0 in both eyes.
Bilateral Choroidal Effusión After ICL Implantation/de Rojas et al
Figure 1. Slit-lamp photography of the (A and B) right eye and (C and D) left eye 1 day after surgery in the second eye (right) showing bilateral shallow anterior chamber with vault 0 and patent iridotomies in both eyes. Pentacam (Oculus Optikgeräte GmbH, Wetzlar, Germany) Scheimpflug imaging of the anterior segment revealed an anterior chamber depth of 1,820 and 2,000 μm in the (E) right and (F) left eye, respectively, on day 2 after surgery of the right eye. Vault was 0 in both eyes.